

James R Gordon
-
Posts
1,111 -
Joined
-
Last visited
Content Type
Profiles
Forums
Events
Store
Posts posted by James R Gordon
-
-
Yes I can see the Adam's apple in post 160. However it does not help since JFK is leaning forward and we cannot gauge the exact position of the Adam's apple.
Going back to your B&W image you have misplaced the Adam's apple. The line in the image below points it out.
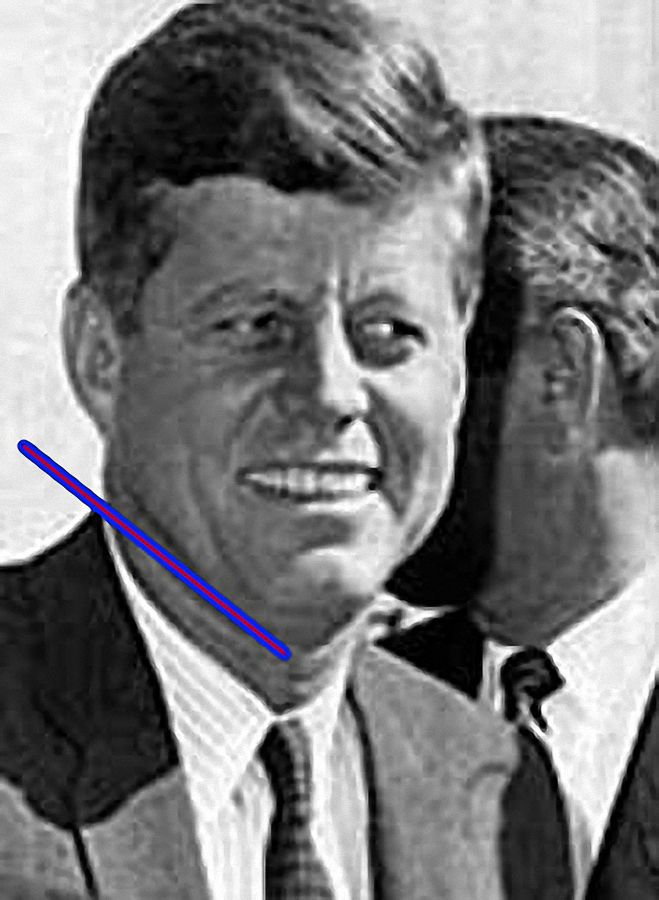
What you are suggesting is the Adams apple is a feature in the neck below the Adam's apple. In the Fort Worth image I have highlighted this feature that you are convinced is the Adam's apple.
Be careful - second warning. Saying anyone with "decent vision" can see the object is being insulting. You are suggesting that if people cannot see what you can see they have a vision defect.
-
Robert,
If you are talking about the B&W image on the left the Adams Apple is significantly above the buttoned area of the collar and therefore the tie. You cannot tell with the Coloured image.
At what Z frame do you contend the injury occurred. It would be helpful to establish the position of JFK's head. If it is similar to the B&W image then I am not sure your point can be upheld.
Finally try not to insult members, it is not a good idea. Whatever a members opinion treat it with respect. It is one of the basic rules of the forum!!!
-
Robert,
There are a couple of problems with your image:
a) Your image has a different size collar.
 It is also drawn together by a clip.
It is also drawn together by a clip.c) His head is positioned differently
but most of all
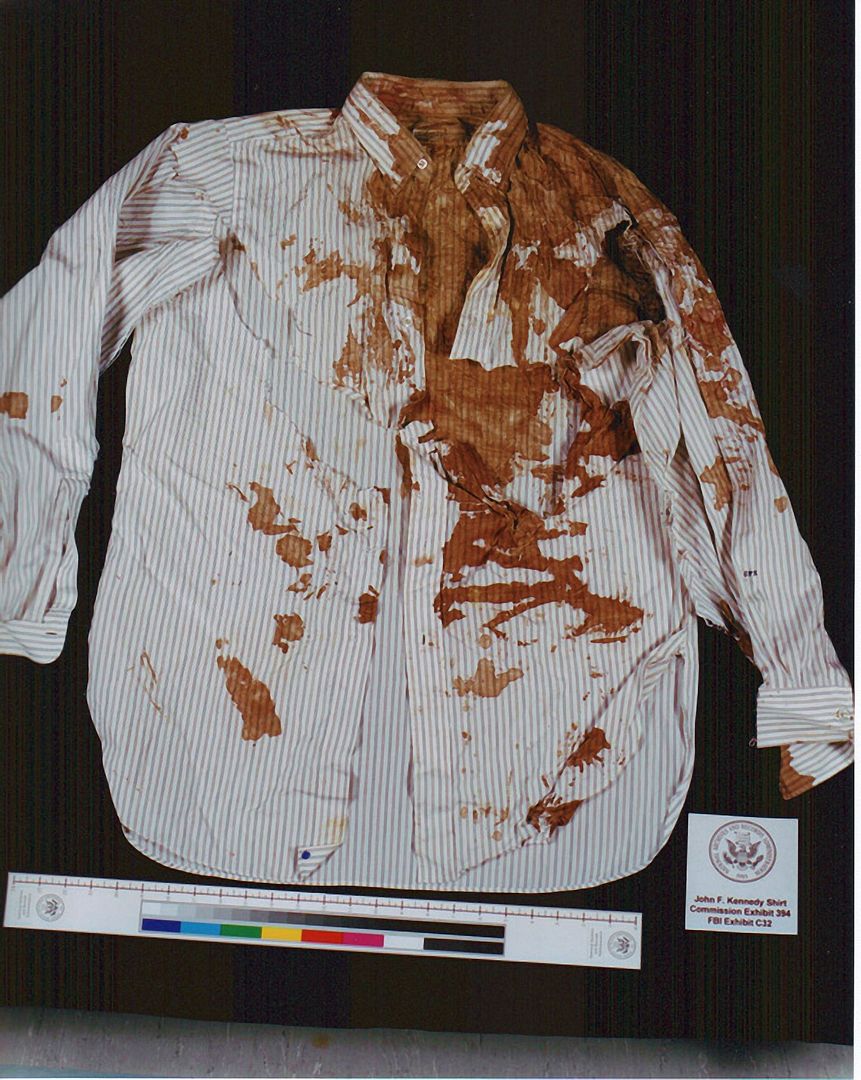
d) My images shows the shirt JFK was wearing when he was shot. JFK was not shot when wearing the shirt in your picture.
-
Robert Pruhomme said:-
“We know from looking at photos of JFK from earlier on 22/11/63 that the top of his shirt collar was resting against the bottom of his thyroid cartilage (Adam's apple), placing the wound in his throat well below the top of his shirt collar and, coincidentally, almost exactly where the "slits" in his shirt were.”
That is totally incorrect as this image taken at Fort Worth that morning demonstrates.

-
Robert Prudhomme said:
“The word "collar" is deceiving. You're right, the slits are just below the narrow collar band, but well above the actual bottom of the collar itself.” Post 140
I have no idea what you are saying here Robert. The fabric underneath the “collar strap” - as you put it - lies beneath the neck. But you say that beneath the “collar strap” is also part of the collar: as you say it is the “bottom of the collar.” Can you point out where that part of the collar is on the shirt? My understanding is that what is referred to as the “collar strap” is the collar of a shirt.
Robert Prudhomme said:
“Something we all should consider is that while we seem to be in agreement that the "slits" below the collar band were not made by a scalpel, they certainly had to be made by something, and I find it highly coincidental they are roughly in alignment with a nick in the tie that is adjacent to what appears to be a bloodstain.” Post 143
On page 598 of “Post Mortem” Harold Weisberg makes the following comment about the slits on the shirt. He says that Carrico said “that this damage to the shirt was done when the necktie was cut off by nurses under his supervision during the emergency treatment.”
We know Weisberg interviewed Charles Carrico and this comment makes clear that Weisberg clearly asked Carrico about these slits. Carrico makes stated that the damage was created by a scalpel. He also makes clear he was in the room when these cuts were made. If you disagree with this evidence from Carrico what evidence have you got that he is not telling the truth or that he did not see Diana Bowron - who I believe was one of the two nurses - use a scalpel to cut the tie and shirt off.
It is a common complaint that no one else said this. Well maybe the answer is that no other researcher asked that specific question to Charles Carrico: no one bothered to ask him how these slits were made. In addition the state of the front of the shirt supports the notion that a scalpel rather than scissors were used to cut the shirt off JFK.
-
Sandy,
I assume you have not looked closely enough. These slits are not similar in size. In screen pixels on my screen the R slit is 67.91 pixels whereas the L slit is 101.32 pixels.
With regard to the trachea rings I was referring to this:
"Note about the location of of tracheal rings: Tracheal rings are located in different places depending upon the person. For example, my first tracheal ring is located below my sternal notch when I'm holding my head upright. The top of my tie knot lies just below the bottom of my thyroid cartilage."
I am not at all sure what you mean by:
"The autopsy photos show the location of the tracheotomy incision, which of course is above the sternal notch. The number of rings (below rings 2 & 3 or 3 & 4) hidden by the sternum may not be many, judging by the x-ray of Kennedy's chest. You can tell by where the clavicle bones meet the sternum that Kennedy's sternal notch is unusually low. Which would tend to expose more rings. Maybe all the rings are above the notch. AFAIK there is no way of knowing."
Maybe it is me but I do not see what you mean by the point "The autopsy photos show the location of the tracheotomy incision." I know where the autopsy incision will have been, but I do not see that in the said Xray. Looking at the Xray above C7 is just below the notch protruding just above it. Above C7 we can see C6, C5, C4 and the beginning of C3. So I am not quite sure what is meant the above statement.
James.
-
Sandy,
So if I understand you what you are saying it is that a shard of bone - yet to be specified from where did the following:-
a) It penetrated the left side of JFK's shirt - Causing the damage we see on the highlighted by the R
Then this bone fragment continued to penetrate the left side of the shirt that was buttoned on top of the right side indicated by the letter L. However this time it created damage that is much larger than on the inside of the shirt.c) Jfk's tie was knotted so that the area that is damaged - and was probably a scalpel nick - was now at the back of the tie. Later the tie was re-knotted allowing this damage area to now be seen on the front of the knot.
I'm sorry that does not seem logical to me. In addition if trachea rings 2 & 3 were - depending on the individual as you suggest - were as low as that, then where do you imagine trachea rings 4 to 7 were in this body????
James
-
Ray,
You are absolutely right, a bullet would not create such damage. This damage was created at Parkland.

It was most likely a scalpel when it was being used to cut the tie off. When the shirt is buttoned up - as it was when JFK arrived at Parkland - then the Left side would be over the left side. The importance of this is that when the scalpel touched the shirt - when cutting off the tie it also cut through the shirt. However the Right side - which when the shirt is buttoned is underneath - has smaller damage. This makes clear that the impact on the shirt was lighter here and the damage here smaller.
Below is an image of the tie - although we have no image from the 22nd of the tie - this suggests what it would have looked liked when cut off.

If we are to believe that this is damage caused by a bullet. It might be worth noting that this exit/entrance hole is below the collar line. We know the damage to the trachea was around rings 2 and 3. Well if this is bullet damage that is a quite a distance from there.
James
-
In the conversations I have had with Gary Murr, he was quite adamant that the 6.5mm Carcano ammunition, found in Oswald's rifle, was manufactured in 1954 by the Western Cartridge Company of the USA, despite my protestations that this ammo was made by the WCC prior to 1944.
Either way, this makes the WCC 6.5mm ammo either nine or nineteen years old in 1963; hardly what could be called "aged" ammunition, if the ammo was well manufactured and the cartridges were well sealed.
Regardless, though, of claims of cartridge deterioration, it must be understood the degree to which a cartridge, normally capable of propelling a bullet at 2200 fps, would have to deteriorate to propel a bullet at a low enough velocity (<300 fps) in order to make only a shallow flesh wound at a range of 50 yards. This is an astonishingly low velocity for this rifle, and a bullet leaving this rifle at this velocity would likely be so unstable it would be tumbling end over end on its way to JFK's back, and would make an oblong entrance wound in JFK's back instead of a round wound. Tumbling bullets are also more prone to air drag, and if this bullet were tumbling it would be slowed down much quicker.
As I have been pointing out in another thread, a shooter would not be expecting such a defective cartridge, and would be aiming in a normal fashion. If he did so, the bullet would land far short of the target, as this graph below illustrates:

Trajectories of a projectile with air drag and varying initial velocities
Robert,
I am very busy at the moment but I will get round to your question as soon as I can. I am planning soon to return to this thread that - since I posted it - I have done little with.
I am aware that Gary Murr has argued that the 6.5mm Carcano ammunition was very old and suspect. Gary does not make a statement unless he knows that point to be also a point of fact. His knowledge of the ammunition used in the assassination - and here I do not intend to be rude - is light years away from everyone else. The book from which this information comes from from is the product of 15 - 20 years of study.
From what I understand, there is no-one who has either undertaken a study of this nature OR who has accumulated the factual history on the ammunition used in the early 1960's that he has.
James.
-
I think this thread is an example of one of many I've read here where researchers try to speculate on what happened. There's actually nothing wrong with speculating. Cops do it all of the time when they're investigating a crime. But it seems like some researchers call out others for speculating where as their own information they post is also speculation (e.g., my speculation is right; yours is wrong). So does speculation on both sides of the aisle just basically cancel out everything? Perhaps.Meanwhile, I wanted to comment on the plastic/powder/frangible/not frangible bullet theory. I think we're giving the Bad Guys way too much credit regarding using some super-secret, super-exotic bullet/dart/projectile to kill the president. That's not to say they didn't plan this very well - my own speculation runs along the lines of Oswald was either supposed to be killed near the TSBD or, having failed that, be killed in the Texas Theater. When all of that failed, they said to hell with it and just sent in their Mobster to do it on live TV no less.But as far as the mechanics of the shooting itself, weren't there metallic fragments found all over the inside of the car? To me, it flies in the face of common sense to think that they'd mix the bullets up, using metal ones in some of the guns, and plastic/powdery/dart ones in the other guns. I think this is just one of several examples of researchers over-thinking what may have happened.As for the "he sat there between shots because toxins froze him" theory - I really don't think that happened either because, as I said earlier, no one can predict how one is going to react to gunshot wounds. I would encourage other researchers to look around on the internet because there are plenty of videos out there showing a variety of victims being shot. Some just collapse while others continue to stand or sit as if they're shocked.I think it's a really, really big leap of faith to think that the Bad Guys would use some kind of poison or toxic chemical to "freeze" Kennedy in place. As I also mentioned, Jackie was not shot or sprayed with anything but she looks confused and "frozen" too until Z 313.
Okay, Michael, here is a question for you. If the back wound at thoracic vertebra T3 was not made by a frangible bullet, care to speculate on what type of bullet made this wound? Do you think it penetrated the chest cavity or was it just a shallow wound?
Robert,
As i have pointed out numerous times, I believe the wound to the back was a shallow wound that never penetrated the chest cavity. It is true that Sibbert OR O'Neill left the autopsy room to check on “Ice bullets” [ they have testified that happened but always made clear that one always remained in the room to witness all that occurred there ] but that had nothing to do with the back wound. The enquiry about “Ice Bullets” was with regard to the throat wound and particularly the damage to the apex of the lung.
I know that it is a common belief that the wound to the back was at T3. As I have demonstrated a number of times, I believe it was higher. JFK's body and particularly the protrusion of his Scapular showing through his back, make it clear that wound was higher [ quite significantly higher ] than the outer edge of the Scapular spine which can be seen on the autopsy image. The outer edge of the Scapular spine is just below T3. As I view it anatomy physiology that ought to be beyond dispute. I have argued that according to anatomy physiology the wound appears very close to T2. It could even be argued [ based on how far one believes the wound is in relation to the Scapular spine's edge ] that the wound could be between T2 and T3.
In my view anatomy physiology trumps speculation and rough guidelines on an autopsy chart.
I am happy for you to argue that I am wrong, but I would like to to address the position of the wound in relation to the position of the scapula spine. Why do you feel that the wound is still close to T3 when it is well above the position of the Scapular spine's edge?
James.
-
Michael Walton said:-
Didn't these two FBI agents also say during their viewing of the autopsy that they saw "surgery to the top of the skull" or some such statement? And didn't these few words from two government officials, who had no medico experience to speak of, start an entire cottage industry in the JFK case, perhaps reaching its pinnacle when David Lifton wrote his "body alteration" book (which, when I read it at 18 years old I believed it but since then, I think it's way too outlandish for it to have happened)?
Just because these agents were in the room mere yards away from the body did not make them experts at what they were observing.
Michael you appear to misunderstand the role of Sibbert and O'Neill. They did not see “surgery to the top of the skull.” What they wrote down was a comment from Humes. He was the one who identified that - in his opinion - there had been surgery of the skull. All Sibbert and O'Neill did was record what was said, what happened and who was present. Nor is this a small issue. Parkland are adamant that there was no surgery while JFK was at Parkland. Whatever deficiencies members may feel about the competence of Humes - some of the criticism I feel to be unfair - it was he who recognised someone had worked on the body before he started the autopsy. What is not clear is what is meant by that statement. We have no idea what that statement means but one thing is clear something happened between Parkland and Bethesda.
As regards David Lifton we will have to agree to disagree. DSL's view that what happened at Parkland and Bethesda - and remember he has extensively interviewed nearly every medical personnel involved. All he said was that - in his opinion - the evidence left him with only one option: something had to have taken place between these two hospitals. Remember this theory was devised back in the 1980's. I suspect when his new book comes out we will be presented with a much more sophisticated explanation. Though I find his work useful, I do not share Doug Horne's description of what happened in Bethesda or his characterisation of Humes.
Finally Sibbert and O'Neill do not need to be “experts” all they needed to do - which is what they did do - was record what they saw and heard. It is for others to interpret what that meant. Sibbert and O'Neill have been interviewed a number of times through the years and one point they are definite happened is that Humes commented that he was sure he was seeing surgery had been done to the head. No one in that room said exactly what it was they were seeing, but Humes was clear that what he was seeing was that someone had tampered with the head.
James.
-
Sandy,
That Xray was taken before the autopsy began. For me the importance is the collapse of the neck to the right. Whatever caused this, it was not Humes. He had yet to carry out the autopsy procedures.
There is another - close up - which was taken after Finck arrived. I believe it was he who suggested another set of X-rays.
The second set were taken after the organs had been removed.
James.
-
Roy Wieslquist Said:-
Maybe the biggest problem, for researchers, with a South Knoll shooter making that early throat (and back) shot is they don't think a shot could have cleared the windshield (with visors up too) AND the wide roof-support over the back of the front seat. I have ways to demonstrate that it could be done.
I do not see how that is possible. Don Roberdeau's map has the North Parking lot at 426 Hasl. The rail line on top of the Triple underpass is 424 Hasl. Elm Street at 2o7 is 423 HASL. The Sixth Floor Museum the North and South Plaza are effectively and that the Post Office parking lot is 426 HASL. The Triple underpass is the sam at both ends: 424HASL.
So from what I can see, because of the geography of the Plaza, the shooter at the South Knoll does not have a heightened elevation to fire down from. Then there is the position of the occupants in the car, A shot from this angle is bound to put Bill Greer and Nellie Connally in some danger. In addition, any shot entering JFK's throat is not going straight forward it is going from centre to right.
I do not see this as a serious theory.
James.
-
Sandy,
Because I am so preoccupied with another task, I have not been able to return back to my JFK work. But when I was focused on JFK my approach was always based on trajectory analysis. When I looked at a wound my first question was where that wound came from.
The Car at Z 223/4:-

I did numerous trajectory analysis and the three options - aside from the Oswald window - was the TSBD West Window the Daltex building and The Records building. One thing I learnt was that there was not just one source of the shots - the view point of Warren Commission Apologists. My work made clear there were numerous sources. The question was always how reliable they were and that was always a judgement call.
Looking at the image above which has the car at Z 223/4 it is clear a shot to JFK's back would be troublesome to validate. If the shot to JFK's back was fired at this point you can see the effect of decline on where such a shot - if it ever did penetrate the chest - would end up.
An area of research that always troubled me was not whether we can have a shot from point A impact at point B. The point is should there have been a shot from point A that did impact at point B where would the angle of trajectory suggest it would end up in the body: point C That is why the SBT is complete nonsense. Yes you have a wound on JFK's back - though I argue it may not be as low as T3. And yes there is a wound just right of centre on JFK's throat. However there is no way to link these two points without doing considerable damage to the lung and chest area as well as severely damage the cervical spine and the nerve cord. That may not be part of the traditional SBT but it is fundamentals of human physiology.
James.
-
Sandy,
There is a couple of points I ought to make,
a) the Connally wound was down the outside of his rib. From what I remember the direction of the bullet traveled down the right side of his body in a straight line. The position of Connally - at that moment - as well as the position of the car at Z 230 made that possible.
Whereas Connally's wound entered just under his arm pit, the Kennedy wound is a few centimetres right of his spine. A missile entering that point from the west window will be moving in a right to left direction. That may have an impact on your calculations.c) Moving the car up to the position of the Stemmons sign will certainly affect to what degree any shooter could hit that point on Kennedy's back. Down at Z 230 the car is forward of the west window. At Z 220 - or thereabouts - the car is still forward of the East window, but I am not sure what it's location would be with regard to the West window.
Just some thoughts for you.
James.
-
Sandy,
It is a common belief to feel that shots fired from the 6th floor of the TSBD came from the Oswald window.
When I was working on my Connally project I became aware that the 6th floor west windows were both open during the Assassination.
For the Connally wound I needed a steep decline in order to travel down the 5th rib. The only window that allowed that was the 6th floor west windows.
One example of what I mean is were Connally wounded at 230 then the angle of the shot - at that point - I estimate was around 65º Yes that is outside your parameters but if the back wound occurred earlier then you would achieve a different result. Whatever the position of JFK, the Oswald window will always give you a smaller degree and could well be outside your parameters.
One thing I was very curious about was exactly what was the south wall of the 6th floor like. Thanks to Gary Murr I acquired an image taken on the afternoon of the 22nd. Behind the south wall of the 6th floor was a clear corridor allowing movement and coordination.
Do with this as you please. But if the angle of the back wound is legitimate then one source for it could well be the west window on the 6th floor.
See images.
James


-
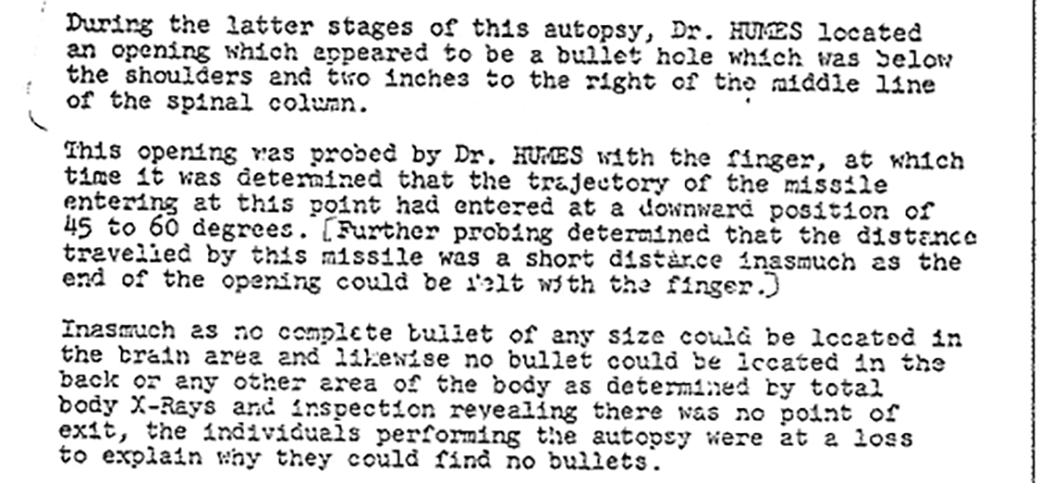
Things have been pretty dull around here lately so, I thought it might be a good time to take another look at JFK's "shallow" back wound; observed by many witnesses to be almost six inches below JFK's collar line (about the level of thoracic vertebra T3) and about 1.5-2 inches to the right of JFK's spinal midline.
First, let's see whereabouts on JFK's back that entrance wound would have been, and how it relates to the location of bones and organs in the upper thorax.

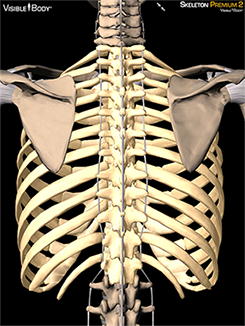
As seen in the top diagram, a bullet entering the back at the level of T3 and 1.5-2 inches to the right of the spine would have nowhere to go but into the Right Upper Lung (RUL). As the skeletal diagram shows, this bullet would miss both the vertebrae and the scapula (shoulder blade) and would have an excellent chance of passing between two ribs, without touching either of them.
As I have pointed out many times, it has long been held as fact that the bullet that hit JFK's back only penetrated the flesh of his back a mere inch; not far enough to enter JFK's right pleural cavity. This shallow penetration, supposedly probed by Commander Humes' finger, is credited to a phenomenon known as a "short shot", in which a rifle cartridge is either loaded with an insufficent gunpowder charge or the entirety of the gunpowder charge in the cartridge does not ignite, drastically reducing the muzzle velocity of the bullet.
In order to reduce the penetrating power of a 6.5mm Carcano bullet, at a 50 yard range, to the point where this bullet will not penetrate more than an inch in soft tissue, its normal muzzle velocity of 2200 feet per second would have to be reduced to less than about 400 feet per second (fps). This presents all kinds of problems in a) accurately hitting within 20 feet of your target and
actually getting the bullet to its target.If you have a rifle that is properly sighted in at a range of, for argument sake, 100 yards, and you chamber a good round into the breech, hitting a target at 50-100 yards is a simple matter of aiming and squeezing the trigger. However, bullets begin to drop as soon as they leave the barrel, and if that bullet leaves the barrel travelling at 1/5th the expected velocity, and the shooter is aiming in a normal fashion and expecting his bullet to be travelling 2200 fps, that bullet will end up impacting the ground (or pavement) far short of the aim point. In the case of JFK, I would not even expect it to hit the back of the limo. This is why it is called a "short shot", as the bullet impacts far "short" of the point of aim.
The next problem you would have with such a slow moving bullet is stability in flight. While the rifling grooves in the rifle's barrel that impart a gyroscopic spin to the bullet in flight account for most of the bullet's stability, the velocity that bullet is travelling at also plays a big part in whether the bullet remains stable in flight, or whether it begins to yaw and tumble on its way to its target. I have seen this problem when handloading rifle cartridges and experimenting with different types of gunpowder, different loads of gunpowder and different weights and styles of bullets. Just by changing the velocity of the bullet slightly, by adding more or less gunpowder, it is possible to over- or under-stabilize a bullet, with the resulting "keyhole" effect on a paper target. A "keyhole" is when a tumbling bullet goes through a paper target side on, leaving the inevitable "keyhole" in the target instead of a round hole. If a bullet still travelling in excess of 2000 fps can be under-stabilized by a reduction in velocity, imagine the lack of stability in the typical 2200 fps bullet reduced in velocity to only 400 fps.
Quite frankly, I don't believe such a slow bullet could have ever made it to JFK's back, making the shallow back wound a myth; at least in my eyes anyways.
Bob, I realize this thread is now examining the medical evidence, and I do not want to go OT, but your original post touched on something I have considered and suggested many times in the past.
In my research I have come to conclusion that, where Oswald's rifle was concerned, the problem was not so much with the firearm itself but with the ammunition it chambered. When the FBI visited Klein's in Chicago, (I believe this was in early 1964), a rifle identical to Oswald's was test fired for them by the same employee who claimed to have mounted Oswald's scope. During this test firing the shop employee recalled that the rifle experienced several "hang-fires" which he believed the FBI may not have even noticed.
I'm sure you are aware Bob what a hang-fire is, but for those reading this post who may not be... a hang-fire is a delay between the pulling of the trigger and the moment at which the round discharges. This can be caused by either a faulty primer, (the small round chamber visible at the base of the cartridge which is struck by the firing pin causing the powder within the casing to ignite), or by the introduction of moisture into the powder within the casing itself. Here is a quote from the same time period in which the MC's ammunition was initially manufactured...
"A paper from 1885 laments that "Gunpowder is such a nervous and sensitive spirit, that in almost every process of manufacture it changes under our hands as the weather changes." Pressing times to the desired density could vary by a factor of three depending on the atmospheric humidity.[89]"
My point is this Bob, if Oswald experienced a hang fire, or a combination of perhaps two related malfunctions during his first shot, could this not have caused the shallow back wound? As someone who has a moderate degree of experience with firearms I can tell you that a hang fire would certainly effect the striking point of a projectile on a moving target.
At any rate, this is quite an interesting subject in particular.
Regards,
Craig C.
Spot on Craig! This is - I believe - the topic of Gary Murr's yet unpublished book on the guns and the ammunition used in the early 1960's. Gary has shared much of his research with me but he has been reluctant to share his work on this book. I believe he has broken new ground that no one is remotely aware of and would shed tremendous light of the wounds JFK sustained including the origin and nature of the back wound.
Next to David Lifton's new book, “Forgotten” is the book I am most eager to read.
James.
-
Some time ago I wrote an article that outlined my reasons why I became convinced the throat wound was a wound of entrance and not one of exit.
In that article I outlined what damage the bullet would have had to create had it entered JFK's throat and traveled through his body.
A copy of that article can be found here:-
https://www.transferbigfiles.com/85d3031a-e837-4c73-9827-fe5021ae2719/0UluhDdPcejZiC-gTezDdg2
James.
-
Bob,
I have not read Lipsey's testimony. I accept you have. Might I ask is Richard Lipsey your central source and if other sources contradict him are those sources discounted by you.
Five centimetres is 2 inches. We are talking about a 2 inch damage from the apex of the lung. On the 6th of December 1963, the Supplemental Autopsy report was submitted. And it was in that document that Humes acknowledged that indeed the right lung had been damaged. “Sections through the grossly described area of contusion in the right upper lobe exhibit disruption of alveolar walls and recent hemorrhage into alveoli.” CE 391 P. 2 My emphasis added.
The consequence of this damage was what caused blood and air to escape into the Mediastinum. It was this situation that persuaded Dr. Perry to request chest tubes to be inserted.
Like many others I had read this before and I had been blinded by the word “haemorrhage” and just thought it was description of a bruise to the lung the collection of blood around the lung: something we all had known before.
Actually what Humes was saying something quite different.
a) The trachea eventually branches into two pipes called the Bronchi one for each lung.
As these pipes grow within the lung they continue to subdivide and branch out.c) As they do so they get smaller and continue to do so until they have covered the entire area of the lung.
d) At the end of each branch line is a small air sack called an Alveoli. Each lung has around 300 million of these Alveoli, which gives you an idea of the number of branches that have subdivided within each lung
e) Each Alveoli is connected to a Pulmonary ( a lung ) artery and a Pulmonary ( a lung ) vein.
d) And basically what the Alveoli do is transfer air from the arteries to the veins. It is the process by which air gets into our blood.
So what Humes is actually describing is this:-
a) When the bullet landed on the Apex of the lung it ruptured a significant number of these Alveoli. This is my view that the bullet that couse the throat wound came to rest on top of the right lung and it was this that caused damage to the Apex of the right lung.
That meant these Alveoli’s associated arteries and veins were also damaged.c) As a consequence of these vessels being damaged, blood now poured into the Lung.
d) One consequence of this flow of blood was that it created the bruise Humes talked about.
e) However a second consequence was that the blood also broke through the Visceral Pleura as well as the Parietal Pleural.
d) It was through this damage that air from the lung also escaped: the air that Malcolm Perry had noticed and caused him to ask for the Chest Tubes to be inserted.
e) Blood also escaped through this damage and collected in the Mediastinum – the upper chest area. This was some of the blood that Malcolm Perry noticed once he had cut the Tracheotomy.
f) Once the right lung was damaged, the Trachea now deviated to the left .. towards the undamaged lung.
Now it is true that Malcolm Perry is on record stating that as far as he was concerned the Pleural cavity was not damaged. When Malcom Perry was interviewed by the HSCA he was asked about the Pleural cavity, the space between the two Pleural skins:-
“PURDY “How did you determine that the pleural cavity was not violated?”
PERRY “Found that out later in the autopsy report.” HSCA1 304
So Malcolm Perry is on record stating that the Pleural cavity was not damaged, not from personal observation, but because the Autopsy report said it was not damaged. His personal observation was quite different and was the reason he had asked for the Chest Tubes to be inserted in the first place.
And hidden in CE 391, the Supplemental Report, was confirmation that Malcolm Perry’s initial judgment had been right all along: the right lung had indeed been damaged.
From what I can see there is significant evidence that the top of the right lung was damaged. From what I have read there is no evidence that the central portion of the right lung whereas there is critical evidence that the top of the lung was damaged.
James.
-
Bob,
Like Sandy I am not here to interrupt your thread which I find interesting. However, though I agree the right lung was indeed damaged, it was damaged at the top and not in the body of the lung. In a document I wrote about JFK's injuries I described this observation. It is a wonderful description by Humes. Senator Cooper asks him what was the character of this bruise at the top of the lung. Humes reply is wonderful and I am not sure he was fully aware of what he actually said. Below is the section describing this moment.
A few pages later, Senator Cooper interrupts Commander Humes and asks him what was the character of this bruise that he saw. Humes replies and in doing so describes just what an incredible anomaly this “bruise” was. This is just such an important point I will parse what he says.
First Commander Humes reply.
Commander HUMES. “The bruise here, photographs are far superior to my humble verbal description, but if I let my hand in cup shaped fashion represent the apical parietal pleura, it was an area approximately 5 cm. in greatest diameter of purplish blue discoloration of the parietal pleura. Corresponding exactly with it, with the lung sitting below it, was a roughly pyramid-shaped bruise with its base toward the surface of the upper portion of the lung, and the apex down into the lung tissue, and the whole thing measured about 5 cm., which is a little - 2 inches in extent, sir.” H2 369
a) First Humes describes the shape of the Apical Parietal Pleura.
“if I let my hand in cup shaped fashion represent the apical parietal pleura, it was an area approximately 5 cm. in greatest diameter of purplish blue discoloration of the parietal pleura.”
• So what he is saying is that the Apical Parietal Pleura was rounded like his cupped hand.
• He then says that this area of the Apical Parietal Pleura was bruised and the size of the bruise was 5cm.
• Then he describes the colour of the Pleura as purpilish blue.
Now this first reference of 5cm refers not just to the size of the Apical Parietal Pleura that was damaged but also the size of the base of the anomaly, which was underneath it.
Now Humes goes on to describe the shape of the anomaly.“Corresponding exactly with it, with the lung sitting below it, was a roughly pyramid-shaped bruise with its base toward the surface of the upper portion of the lung, and the apex down into the lung tissue, and the whole thing measured about 5 cm., which is a little - 2 inches in extent, sir. ”
a) “Corresponding exactly with it, with the lung sitting below it,” The “it” refers to the bruise on the Apical Parietal Pleura. He then says that the lung was positioned below the Apical Parietal Pleura .. as indeed it is.
“was a roughly pyramid-shaped bruise.”He now describes what the shape looked like. He likens it to a pyramid.
c) “with its base toward the surface of the upper portion of the lung.” Normally pyramids have their pointed portion facing upwards. However, this anomaly is actually upside down and it is the base, or bottom, which is facing upwards. However there is another point he makes here. Humes says that the base of this anomaly is towards the surface of the lung itself. Above the surface of the lung are the Apical Parietal Pleura, the Parietal Pleura and finally the Visceral Pleura. If the base is toward the surface of the lung, then it has to be below these three surfaces.
d) “and the apex down into the lung tissue.” The pointed end of this pyramid is not just facing downwards, with the use of the word “into” Humes is saying that this part of the anomaly is actually inside the actual tissue of the lung.
e) “and the whole thing measured about 5 cm., which is a little - 2 inches in extent, sir.” The use of the word “thing” refers to the shape of the anomaly. This part of the description has been about where the base of the anomaly was in relation to the top of it. Therefore this reference to 5cm, refers to distance between the base and the top. It is that which is 5 cm. Hence the anomaly is 2 inches tall. The first description of 5cm, although describing the area of the Apical Parietal Pleura that was bruised, is also describing the measurement of the base of the object that lies below it.
In his description Humes has just admitted that the right lung was damaged. He has said that:-
a) The base of this anomaly is towards the “surface of the upper portion of the lung.”
AND
“and the apex down into the lung tissue.” The top of this pyramid is inside the lung itself. He is therefore saying that the tissue of the lung has been pierced.What caused this damage is another matter. However, Humes is quite clear that the damage is at the top of the lung and not the middle and body of the lung. Unless you have evidence that I had been unaware of, there is no evidence that the body of the lung was damaged or pierced.
I disagree that the wound to the back was anything but a shallow wound. However I am not going to interrupt your thread by arguing my corner. Nor am I going to interrupt the thread by arguing where I believe the lung was damaged. However I did want to place my opinion into the record.
James.
-
Robert,
“How close were Sibert and O'Neil to JFK when Humes supposedly probed the back wound with his finger? Were they standing right beside Humes, looking down, or were they in the gallery many feet away? Where does it actually state Humes used his pinkie finger?” Robert Prudhomme Post 11
Sorry I have not been able to get back to this thread for a few days, I have been very busy.
Siberia and O'Neil were inside the mortuary. They were not in the Gallery. They were under instruction not to leave until the autopsy was complete and report everything they saw and heard. Whether they were watching over Humes shoulder or not I do not know, but you will be aware that the mortuary was a small room. So to get back to the critical point - unless you doubt their veracity - their report makes clear that they did see Humes prod the wound with his pinkie and explain to all in the room that it was a shallow wound.
That suggests any thought that - whatever caused this wound - was able to pass intthe rib cage let alone into the lung is simply not possible. Whatever this wound was it was not a deep or penetrating wound.
James.
-
Robert,
The Sibert O'Neil report is quite specific. They witnessed Humes making this probe. The report reads that they witnessed Humes probing this wound. The idea that Humes fooled them does not seem realistic or probable. We know both had been instructed to witness everything and report back. Just because you could not do so, is not proof that Humes was also unable to do so?
I take it from your expression "it is time to let the shallow wound go" that you feel this may be a through wound. If I am right I will be interested how you can establish that.
James.
-
Robert,
I do not have all my notes with me at the present, however I recollect that Sibert and O’Neil stated that Humes did indeed probe the wound with his pinkie. An that he concluded that it was a shallow wound.
I agree that the lung was damaged, but not anywhere near where T3 is located. Humes in testimony describes a wound - which he refers to as a bruise - was at the top of the lung.
Commander HUMES. “The bruise here, photographs are far superior to my humble verbal description, but if I let my hand in cup shaped fashion represent the apical parietal pleura, it was an area approximately 5 cm. in greatest diameter of purplish blue discoloration of the parietal pleura. Corresponding exactly with it, with the lung sitting below it, was a roughly pyramid-shaped bruise with its base toward the surface of the upper portion of the lung, and the apex down into the lung tissue, and the whole thing measured about 5 cm., which is a little - 2 inches in extent, sir.” H2 369
The ammunition that you describe in post 4, had that kind of ammunition penetrated JFK’s body it would have created damage that could never have been concealed.
You are right to raise the issue of the back wound. It is indeed a problematic wound. If the wound did not enter the body - as I believe - then what caused that damage and where is the object that created that wound.?
I hope you do not intend to link the back wound with the throat wound. Such a link is impossible.
I will follow this thread with interest and reflect on your thinking on this subject.
James.
-
Ken,
My preference is to still require registration. The restoration is being done for the benefit of EF members - as well as fulfilling a promise we made to Debra Conway. It is not a public forum - in a sense it is a private forum for the use of members of the EF.
As far as scheduling is concerned it is likely to be more like September before it is complete.
James


 It is also drawn together by a clip.
It is also drawn together by a clip.







JFK's "SHALLOW" BACK WOUND REVISITED (FOR THE UMPTEENTH TIME)
in JFK Assassination Debate
Posted
Sandy two issues worth considering.
a) The image of JFK on Main Street is taken from above. Therefore it is not clear exactly where his Adam apple is with respect to his shirt collar. From above the Adam's apple appears closer to the shirt's collar than it may be.
James