

James R Gordon
-
Posts
1,111 -
Joined
-
Last visited
Content Type
Profiles
Forums
Events
Store
Posts posted by James R Gordon
-
-
Without getting into the details just now, you can add Stewart to the list of those who believe (in Stewart''s case, because of what he was told by Perry) that JFK was struck in the left temple.
David,
There is a serious contradiction to the idea that JFK was shot in the left temple. As the copy of Z 312 below shows his left temple was turned away from a shooter in the North Plaza.

Anyone shooting from the North Plaza would be unable to make a hit there. The only area that had access to that aspect of JFK’s body would have to be on the South Plaza.
There has been no evidence that there ever were gunmen in the South Plaza.
The problem for a shot from the South Plaza is that the target has changed. From the North Plaza Jackie is behind JFK. From the South Plaza, JFK is behind her. Any shot requiring to strike JFK would first have to go through Jackie.
I do not question your research. It is amongst the finest in the history of the JFK assassination. However when the results of that research are placed on the historical reality of Dealey Plaza serious questions are immediately raised.
One response to this conflict of evidence is to just ignore it. However “Best Evidence” does not show you to be that kind of a researcher. So I am wondering, do you have a response and solution to this conflict?
James.
-
I typed up a response and then lost it...
David,
I sympathise, it is really irritating when that happens.
I always type up my responses in Word and check before posting.
That way I always have a saved copy that I don't loose. It also gives me a chance to reflect on what I want to say and edit it if necessary.
Just an idea and thought.
James.
-
Mike,
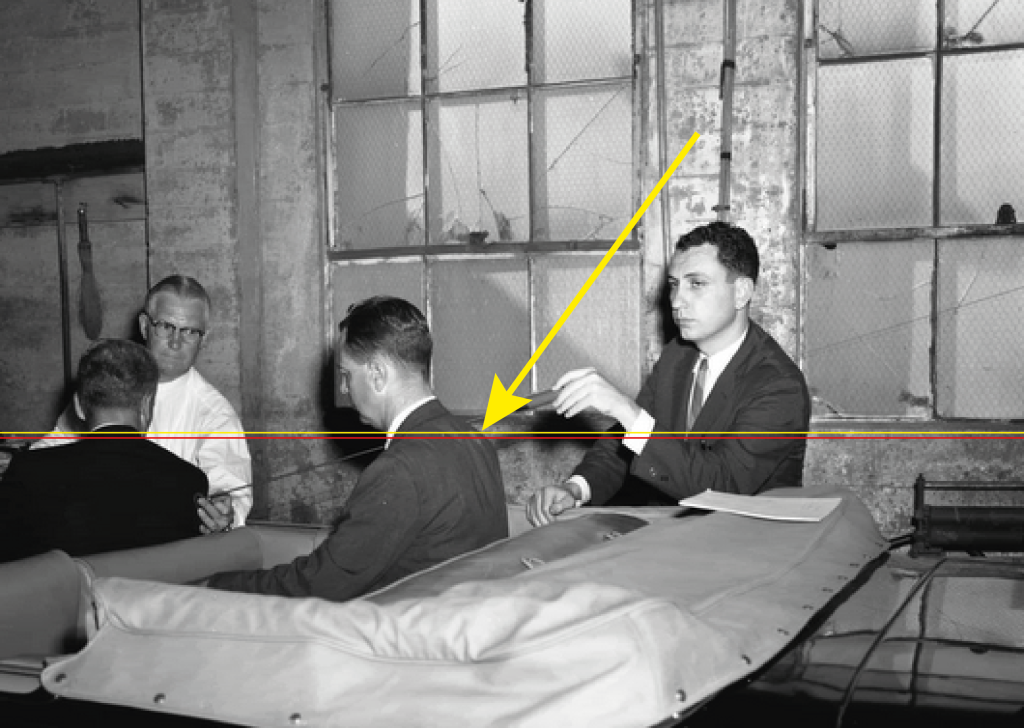
Did you actually even seriously look at the image.
Because Specter has the model bending forward it makes it much more difficult to clearly distinguish the position of the trachea wound from the back wound.
If you knew basic anatomy you would know that the position of the back wound at around T3 invalidates the theory.
However even with the model bent forward it still possible to show that the back wound [ The red line ] is lower than the throat wound [ The yellow line ] Albeit just lower.
Having studied anatomy I can better see the weakness in your arguments. For example you see nothing wrong with the back entry point in CE 903.
The difference between you and me is that I know that if the bullet is there then it is also around T3 and therefore there is no possibility of the lung not being pierced. It is anatomically impossible for the lung not to be pierced.
Bullets do not have satellite navigation.
When Specter created the SBT he never considered what the bullet would have to do to travel through the upper chest. He and the Commission gave that no concern.
All he was concerned with, just like you, is could he link entry and exit points so that two bodies can be injured by a single bullet. Now I do not deny that trajectories are important.
However people like you, with such theories, totally ignore the realities and laws of human anatomy.
Just because you can link entry and exit points does not make your theory a valid one, if in doing so you have given no thought to the implications of those trajectory points.
Anatomical laws may be inconvenient to you, but they are there all the same. And it these laws that make a nonsense of such theories as yours.
- - - - - - - - - - -- - - - - - -- - - - - - - - - - - - - - - - - - - - - - - - - - - - -- - - - - - - - - - - - - - - - - -
Also I take it you can see where the pointer is with regard to the throat exit point. It is below the collar.
With regard to your version of the SBT, how does a bullet the exits through trachea rings 3 & 4 yet go on to leave the body below the collar of the shirt. How is that possible??
James
-
Mike,
“You see a smudge.”!!!!
Is that really the level of your argument?
True is does look higher than it should because Specter had the model for JFK lean forward. If your know your anatomy you will realise that the spot is around T3.
It does not matter one iota where the shot came from, the central problem is that wherever it came from could an entry wound at this point exit through Trachea rings 3 & 4.
The answer is no! Having the entry wound at around T3 means that in order to get to the exit point the bullet needs to go through the lung. There is no other route for it to go.
If you are going to insist on the SBT, then you will need to raise the height of the back entry wound.
As a point of interest. Why do you suggest that your version of the SBT has two parts: when both parts are essentially what comprises the existing SBT. I do not see any difference between the WC SBT and yours
James.
-
Here is the image with a Yellow arrow pointing to the entry wound.
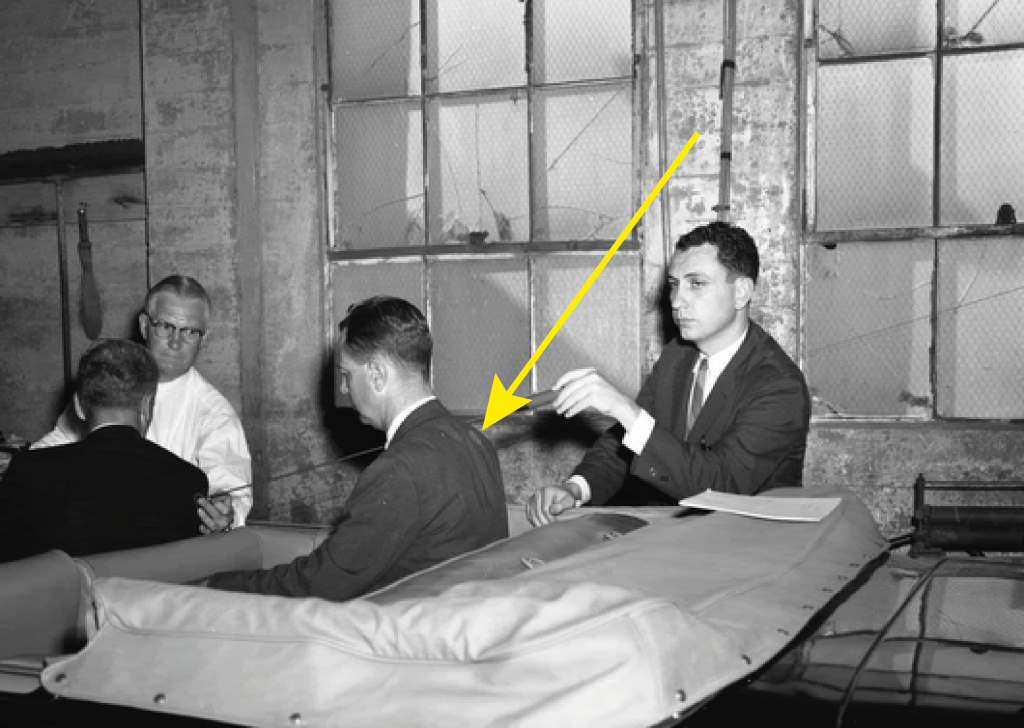
James
-
Sorry Mike,
Your image did not show at first and therefore I did not see it.
Like others you love to use CE 903 which because of the Photographers perspective actually hides where the entrance point is.
Here is CE 903 from a different angle. You can now clearly see the entrance wound is lower than the exit wound.
So again how are you able to explain that?

James
-
Mike,
It is a very poor tactic to dodge a question asked. That is the tactic of those who are weak about their position and don't want to be found out.
I admitted that the absence of bullets is a concern and a easy point to turn against us.
But that was not the question I asked you.
I asked you, how do you address how a low entry wound can go on to exit through a higher exit wound?
Are you able to answer that question??
James.
-
Mike,
How does the absence of the bullets which caused the back and throat wounds, validate the SBT?
Many forum members, such as Ray Mitcham, just above your post, highlight the problem of a low entry wound and a high exit wound.
True the absence of bullets is a problem, but such an absence does not go on and validate the SBT.
Why don't you address how a low entry wound can exit through a higher exit wound. How is that possible???
James.
-
On November 22, McClelland said the President died of a gunshot wound of the left temple. I have always assumed that sentence applied to the bullet entrance wound on JFK's head. (Certainly, he was not referring to an exit wound!)
David,
Earlier in this thread Pat suggested that Robert McClelland had made a slip of the tongue and really meant to say the wound was in the right temple. I tended to agree with Pat.
In this post by you, you make it very clear that this was not a slip of the tongue but an observation that McCellend was very definite about.
If the entry wound to Kennedy's head was actually on the left temple, as opposed to the right temple, that means the gunman had to be in South Plaza.
Because of the angle and position of Kennedy's head at Z 312 / Z 313 the left temple was hidden from any gunman in the North Plaza. Only someone positioned in the South Plaza could strike the left temple.
And there lies the contradiction with an entry wound in the left temple. I do not dispute your research and evidence, I know you have meticulously collected and analysed what the evidence demonstrates and are very proud of what your research has shown.
However if the left temple is the entry point, then the geography of the plaza insists that the gunman was somewhere in the South of the plaza.
I have a problem with that. There is a brevity of evidence to suggest any gunman was in the South of the Plaza.
James
-
James,
You mean that, in relation to David's CAT scan, the exit for the "magic bullet"
(entry for the throat wound) should be slightly the opposite side of the trachea?
Jim
Jim
David’s idea of using an MRI scan gave me ideas. In my amendment to that post I accepted David’s position. All Perry and Carrico said was that it was slightly right of center. We don’t know how much and therefore David’s position is fine.
Taking the lead from David to use a scan I have also modeled the SBT over an MRI scan. The only points I have not dealt with are:-
a) The damage to the Right Strap Muscle
 Nor have I included the real exit point through the throat, which had to be the rear of the trachea. You will find that in my article at the JFK Assassination Forum in the articles section. The article being “The demise of the SBT” You will see there my arguments for the bullet having to exit through the back of the trachea. As far as the SBT goes, that means that the bullet has to enter the trachea through the rear of the trachea. An utter impossibility.
Nor have I included the real exit point through the throat, which had to be the rear of the trachea. You will find that in my article at the JFK Assassination Forum in the articles section. The article being “The demise of the SBT” You will see there my arguments for the bullet having to exit through the back of the trachea. As far as the SBT goes, that means that the bullet has to enter the trachea through the rear of the trachea. An utter impossibility.See image below:-
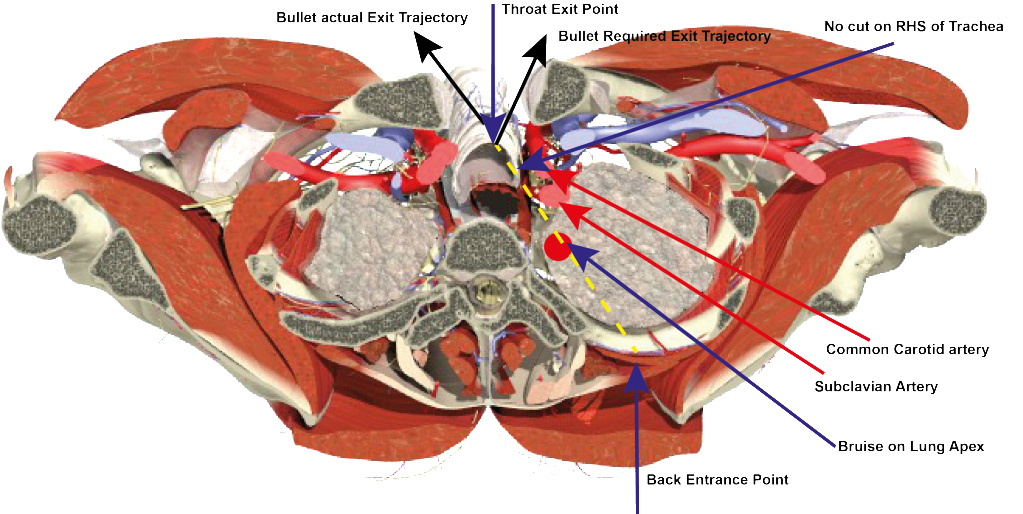
Unfortunately there is a direct line from the position (not taking into account level) of the back wound to the throat exit. And the level is important. The entry not to damage the lung has to be above Costa IR. Actually at the level, not position, that Humes placed it in CE 385. The correct level changes a great deal. So the direct line is a little misleading by suggesting there is a direct path from back to throat.
Also the line does pass over the Apex of the lung, which was bruised.
But there the good news stops for the supporters of the SBT.
a) In order for the bullet to exit through the trachea, as is documented it did, it would have to enter the trachea as indicated. Both Perry, Carrico and Humes are on record stating there was no laceration there. All have stated that the RHS of the trachea was bruised.
The bullet passes so close to the Subclavian artery it would have to be damaged. In addition the bullet is also very close to the Common Carotid artery. Humes is on record saying that no arteries were damaged.c) The Bullet’s exit trajectory would be left rather than right. There is no way for the bullet to continue on its path to John Connally from this exit trajectory.
Finally, a thank you to David Mantik. I had not thought of this method to illustrate the SBT.
James
-
The "magic bullet" theory is not even anatomically possible, as David W. Mantik, M.D., Ph.D., established long ago.
Jim
Although I absolutely agree with David Mantik, from what I can see, in the article you have a link to David has the entry point in the wrong place.
Both Charles Carrico and Malcolm Perry stated that the entry point was right of center. H6 P. 3 + H3 P. 370. It appears to me that David has it left of center
It does not change his outcome, the SBT is still anatomically impossible. But I felt I should point this error out.
Amendment:-
Having studied the MRI scan, I am probably being a bit finicky. It looks to me now that the entry point may be just right of centre. Neither Perry or Carrico stated exactly how far right the entry point was so David's point could well be where they saw the hole.
I was certainly wrong when I suggested it was left of centre. It certainly is not that.
James.
-
But the Parkland doctors by and large disavowed the statements and testimony in which they'd placed the wound on the back of the head, and said they'd been mistaken.
Pat,
That is a fair point that you make. However, this change in position by the Parkland doctors, how much of it was based on an actual change of view and how much on having read the Autopsy report?
In normal circumstances, as I know you are aware of because you have said it numerous times, the autopsy report tops observation. The change in the Parkland doctors views was because the Autopsy report said something different to what they initially witnessed.
In his WC testimony Malcolm Perry commented that the Pleural cavity had not been damaged. When being interviewed by the HSCA he was asked how he knew the cavity had not been damaged. He replied that he had read it in the autopsy report.
I feel there are now areas in the medical testimony when we may need to go back to the Parkland doctors view. I say this because, in my view, in the essential Bethesda record there are all sorts of conflicts that don't make sense. In normal circumstances one would never dream of questioning an autopsy report or the testimony of the autopsy pathologist. However in this case I am beginning to do so.
I absolutely agree with you analysis of McClelland's observation of the left temple.
James
-
The keyword is "model".
No Mike, the key word, well actually key phrase, is “accurate model.”
The quality of these models is such that they are used throughout the world for the teaching and learning of the medical profession.
They are the best thing we have to going back to 8:00pm on the night of 22nd of November 1963 and checking for ourselves whether what is said in the medical testimony stands up.
There is no exit wound to the back wound because it was a shallow wound. However, where the bullet went is a much much more difficult question to answer.
There is no exit wound to the throat wound because the bullet did not exit. I am of the opinion that the bullet had to have been removed. As you will have seen in posts I have made today, it is logic that has driven me there.
But back to the point I made earlier, that I noticed you dodged. Even if these models are not 100% accurate, and I am not saying they are not, they are sufficiently accurate to be able to replicate the SBT. You will find free 3D models online. Maybe not the most accurate, but they will do. Log on to one of these sites and try to apply the criteria of the SBT. It is then you will be confronted with the difference between theory and reality.
James
-
However, the single bullet theory being correct.........
Mike,
What you are saying is complete nonsense.
Humes established five criteria that the SBT had to comply with:-
a) That the entry wound was above Costa IR
That the bullet passed over the Apex of the right lungc) That the bullet bruised the right strap muscle
d) That the bullet exited between Trachea rings 3&4
e) no bones were damaged
Humes then conceded, Dr. Carrico’s observation, that the bullet exited through the trachea. That meant that it had to enter the trachea.
Thus he added a sixth criteria.
All of that you will find in his testimony in H2
Now you show me how a bullet could create a path to do all that. That is the difference between abstract theory and reality.
It is easy to rattle off quotes that support your position, the difficulty is being able to establish that what the theory suggests can also be replicated in the real world.
That is why I said at the beginning that what you are saying is complete nonsense. It is nonsense because when you apply the criteria of the SBT to the reality of the human upper chest area, what is demanded by the theory cannot be replicated. The theory at that point fails.
Don’t take my word for it, get a 3D model and try it out for yourself.
James.
-
a) Assuming you are not a supporter of the Warren Commission, then you will be aware that a bullet entered JFK's throat. However no bullet was discovered. As I see it there are only three options
i. The SBT theory is not a theory but a fact and that explains it. I have presented, along with many other members, reasons why that is not a valid proposition.
ii. That a bullet actually was discovered, but never registered. It is possible, but I find it difficult to see how such a find could escape the eyes of Sibert and O'Neil. For those reasons, although it has logic, I don't see this as avalid proposition.
iii) That just leaves the option that a bullet was removed at some point and that is why a bullet was not found.
There is another option directly indicated in the historical record.
From autopsy-attendee FBI SA Francis O'Neill's sworn affidavit for the HSCA:
Some discussion did occur concerning the disintegration of the bullet. A generalfeeling existed that a soft-nosed bullet struck JFK. There was discussion concerningthe back wound that the bullet could have been a "plastic" type or an "Ice" [sic]bullet, one which dissolves after contact.From autopsy-attendee FBI SA James Sibert's sworn affidavit:
The doctors also discussed a possible deflection of the bullet in the body causedby striking bone. Consideration was also given to a type of bullet which fragmentscompletely....Following discussion among the doctors relating to the back injury, Ileft the autopsy room to call the FBI Laboratory and spoke with Agent Chuch [sic]Killion. I asked if he could furnish any information regarding a type of bullet thatwould almost completely fragmentize (sic).The autopsists wanted to know if there existed rounds which would "dissolve after contact".
The correct answer would have been -- yes!
You are right Cliff, there is that alternative.
I have difficulty accepting that people serious in their determination to assassinate a President would use ice bullets.
But I accept that is an alternative.
Since I would discount that as a possibility, I would still be led back to removal.
James
-
Mike,
Had this question been raised, even five years ago, I would have been very skeptical of such a notion. However, today I am beginning to see it as the central question of the assassination.
I still have some reluctance to embrace that someone somewhere medled with the body, and the theories of Douglas Horne are just too extreme to accept. I have a high respect for David Lifton, and I will await his material on Zapruder manipulation, but I have always found it difficult to accept, especially understanding the enormity of what would be involved.
However, all that said, I am beginning to think that body alteration may well have taken place. And if that took place, then maybe it happened elsewhere.
As this forum will know I have spent he last few months looking at he medical evidence. In looking at this material too many questions are being raised.
a) Assuming you are not a supporter of the Warren Commission, then you will be aware that a bullet entered JFK's throat. However no bullet was discovered. As I see it there are only three options
i. The SBT theory is not a theory but a fact and that explains it. I have presented, along with many other members, reasons why that is not a valid proposition.
ii. That a bullet actually was discovered, but never registered. It is possible, but I find it difficult to see how such a find could escape the eyes of Sibert and O'Neil. For those reasons, although it has logic, I don't see this as avalid proposition.
iii) That just leaves the option that a bullet was removed at some point and that is why a bullet was not found.
A bullet entered the throat AND that bullet did not exit the body. From a logical perspective I can only see three possibilities, outlined above, and since two are non starters for me, that leaves only one option: at some point it was removed.
I am coming to his view, not from a theoretical perspective but from one of logic.
Although I have only just started my study of the head wound, there are already serious questions being raised that I can find no logical answer for.
The damage to the Pons being severed from the Midbrain makes no sense. Humes was not aware that this had happened until he turned the head over. Such damage was not visible from the top of the head. O.k. I am sure some of you will already being offering reasons why Fox 2 shows significant brain matter at the top of the skull.
The first problem for me is that the top of the head, although damaged, has a significant portion of the brain matter still there and visible. Yet underneath this area, that is still contained within the head, is a major dislocation of critical areas of the brain. As well, the position of the Pons is well behind the skull damage that we see in Fox 2.
If it is to be argued that Pons could be damaged by the force of the explosive powers created by the passage of the bullet, then I find it curious that the upper brain matter was left essentially intact, as seen in Fox 2, yet below that extraordinary damage has been done.
However where this contradiction becomes extremely curious is when you map the damage on a 3D model. Then I become faced with a multitude of "Why's" and "How's". And it is these unanswered questions that lead me to wonder whether there is another process been going on. If this damage had been done by the consequence of the bullet, I would have expected to see much more damage in the upper brain area and hopefully see some of this damage to he Pons from above. But you don't, and neither did Humes. He only was aware of it when he turned he brain over.
David Lifton argues that this damage was done in order to find and remove bullets. he would argue that in cutting to find and remove the bullets that is how his was done. I noticed an interesting comment by Humes. In this lower area of the brain, Humes comments that there was a number of lacerations going in all directions. He suggests that the reason for all these tears was the effect of the power of the bullet on the brain. It is possible, but I could think of another reason for these tears.
Alteration or Non-Alteration. My movement towards alteration is not based on any particular theoretical perspective. For me it is based of impossible contradictions and unanswerable questions. Too many questions, which I am daily being confronted with, is making me more and more suspicious and my suspicions are leading me to the only logical conclusion: at some point the body was tampered with.
James
James, Dr. Kemp Clark told the New York Times a few days after the assassination that the bullet that entered his throat "ranged downward" and did not exit. I looked into this further and the best I can tell is that this information was relayed to him by Dr. Perry. Recall now that the FBI report and death certificate indicated a shallow back wound around T-3. So there would be no corresponding exit to the anterior throat wound. Think also if the autopsy description of the throat wound (its size and condition) sounds like a trach incision. Lifton has Perry on record as indicating the size as 2-3 cm in length. That's less than half the size of the wound appearing in the photos and described by Humes. I think one can reasonably connect the dots and ascertain that the bullet was removed by widening the trach incision somewhere between Parkland and the official autopsy beginning at 8:00 pm at Bethesda or shortly thereafter. That's alteration to remove evidence of the real nature of the killing. And if the perps were willing to dig into Kennedy's throat, they would certainly want to dig into his head, as gruesome as this sounds, to complete their job. That would certainly explain the horrible condition of the top of the skull as seen in the autopsy photos and the absence of such at Parkland, and would account for Humes' comment which the FBI picked up about surgery of the head area, at the top of the skull.
Daniel,
I am moving towards removal as the only logical answer. As I commented, I am getting more questions than answers...and it is that, that is directing me towards removal.
Laying the SBT aside for a moment, a bullet entered the throat and did not exit the body. No bullet was discovered during the autopsy and no bullet was recorded on the X-rays. Unless a bullet was recovered and not recorded, that logical only leaves one option open: the bullet was removed.
It is logic that driving me towards the idea of pre-autopsy removal.
It is the contradictions in the head wounds ( and admittedly I have only begun looking at it ) that are driving also towards removal.
I am uncomfortable with the idea of removal, but logic is compelling me towards it as the only solution.
James.
-
Mike,
Had this question been raised, even five years ago, I would have been very skeptical of such a notion. However, today I am beginning to see it as the central question of the assassination.
I still have some reluctance to embrace that someone somewhere medled with the body, and the theories of Douglas Horne are just too extreme to accept. I have a high respect for David Lifton, and I will await his material on Zapruder manipulation, but I have always found it difficult to accept, especially understanding the enormity of what would be involved.
However, all that said, I am beginning to think that body alteration may well have taken place. And if that took place, then maybe it happened elsewhere.
As this forum will know I have spent he last few months looking at he medical evidence. In looking at this material too many questions are being raised.
a) Assuming you are not a supporter of the Warren Commission, then you will be aware that a bullet entered JFK's throat. However no bullet was discovered. As I see it there are only three options
i. The SBT theory is not a theory but a fact and that explains it. I have presented, along with many other members, reasons why that is not a valid proposition.
ii. That a bullet actually was discovered, but never registered. It is possible, but I find it difficult to see how such a find could escape the eyes of Sibert and O'Neil. For those reasons, although it has logic, I don't see this as avalid proposition.
iii) That just leaves the option that a bullet was removed at some point and that is why a bullet was not found.
A bullet entered the throat AND that bullet did not exit the body. From a logical perspective I can only see three possibilities, outlined above, and since two are non starters for me, that leaves only one option: at some point it was removed.
I am coming to his view, not from a theoretical perspective but from one of logic.
Although I have only just started my study of the head wound, there are already serious questions being raised that I can find no logical answer for.
The damage to the Pons being severed from the Midbrain makes no sense. Humes was not aware that this had happened until he turned the head over. Such damage was not visible from the top of the head. O.k. I am sure some of you will already being offering reasons why Fox 2 shows significant brain matter at the top of the skull.
The first problem for me is that the top of the head, although damaged, has a significant portion of the brain matter still there and visible. Yet underneath this area, that is still contained within the head, is a major dislocation of critical areas of the brain. As well, the position of the Pons is well behind the skull damage that we see in Fox 2.
If it is to be argued that Pons could be damaged by the force of the explosive powers created by the passage of the bullet, then I find it curious that the upper brain matter was left essentially intact, as seen in Fox 2, yet below that extraordinary damage has been done.
However where this contradiction becomes extremely curious is when you map the damage on a 3D model. Then I become faced with a multitude of "Why's" and "How's". And it is these unanswered questions that lead me to wonder whether there is another process been going on. If this damage had been done by the consequence of the bullet, I would have expected to see much more damage in the upper brain area and hopefully see some of this damage to he Pons from above. But you don't, and neither did Humes. He only was aware of it when he turned he brain over.
David Lifton argues that this damage was done in order to find and remove bullets. he would argue that in cutting to find and remove the bullets that is how his was done. I noticed an interesting comment by Humes. In this lower area of the brain, Humes comments that there was a number of lacerations going in all directions. He suggests that the reason for all these tears was the effect of the power of the bullet on the brain. It is possible, but I could think of another reason for these tears.
Alteration or Non-Alteration. My movement towards alteration is not based on any particular theoretical perspective. For me it is based of impossible contradictions and unanswerable questions. Too many questions, which I am daily being confronted with, is making me more and more suspicious and my suspicions are leading me to the only logical conclusion: at some point the body was tampered with.
James
-
Arguing from a faked film is to me no evidence at all. No one at Parkland reported such a wound. Recall, if you will, Audrey Bell asking Perry where the wound was, because the face was clear, as well as the top of the skull. Perry turned Kennedy's head to the left and pointed to the right rear. Nurse Bowron reported only one large wound in the rear of the skull. See also McClelland's drawing for Thompson, and the FBI report of surgery, first unearthed by Lifton and published in Best Evidence. The FBI were recording words of Humes that night, and Humes said there was surgery to the top of the skull. The photo above shows the top of Kennedy's head looking like scrambled eggs and hair. Funny no one saw any of this at Parkland. Costella's list of mistakes in the extant film speak to 313 and would be good reading. The government has us fooled, and we have fallen for this fraud hook, line and sinker.
Daniel,
Where is the reference for Audrey Bell asking Malcolm Perry where the wound was.
Although Diana Bowron testified to the Commission that she only saw only the neck wound she also saw the back wound. In "Killing the Truth" P. 189 she informed Harrison Livingston that she also saw the back wound. That makes sense, because I believe she assisted in the preparation of the body for return to Washington.
I believe you will find that Dr. McClelland has commented on what he considered this drawing meant. I understand his view is that it did not reflect a wound as you have described. I cannot remember exactly what he said it really meant. But I am sure it is not the single exit wound that many take it to mean.
The Sibert O'Neill is still dynamite, even after all these years. True it is not clear what was meant, but somebody said it and all Sibert and O'Neill did was to record it.
I have never been persuaded by the Fetzer/Costella theory about Zapruder. The complexity of what would be required is what I find to seriously undermine the theory. And without the Zapruder film we have lost the visual evidence of the assassination.
James
-
I would have thought,the damage caused internally,would be more than apparent externally.Bone missing would appear to me,to make the face distort.I have had a significant head injury,and know from my experience,it can alter the way you look.His face is just,to pristine.IMHO.
Malcolm,
You are spot on about the extent of the damage. I have only just begun to look at the head wound, and at the moment I do not understand the head anywhere near as well as I do the upper chest area.
My interest was raised by the following exchange quoted at the bottom. Photograph 46 is not in the public domain. Clearly the HSCA panel are interested how the damage this far down in the brain was caused. They even wonder whether the damage was created by the work of the autopsy. Humes denies his autopsy work was responsible. It is pity we don’t have Photograph 46 to see what they are talking about. It was Humes reply that really interested me. In his view what has happened this far down in the brain was only partly caused by the bullet. Interesting what he thinks also contributed to this. It is interesting that as far as Humes is concerned the bullet did not need to be low in the brain to do this damage.
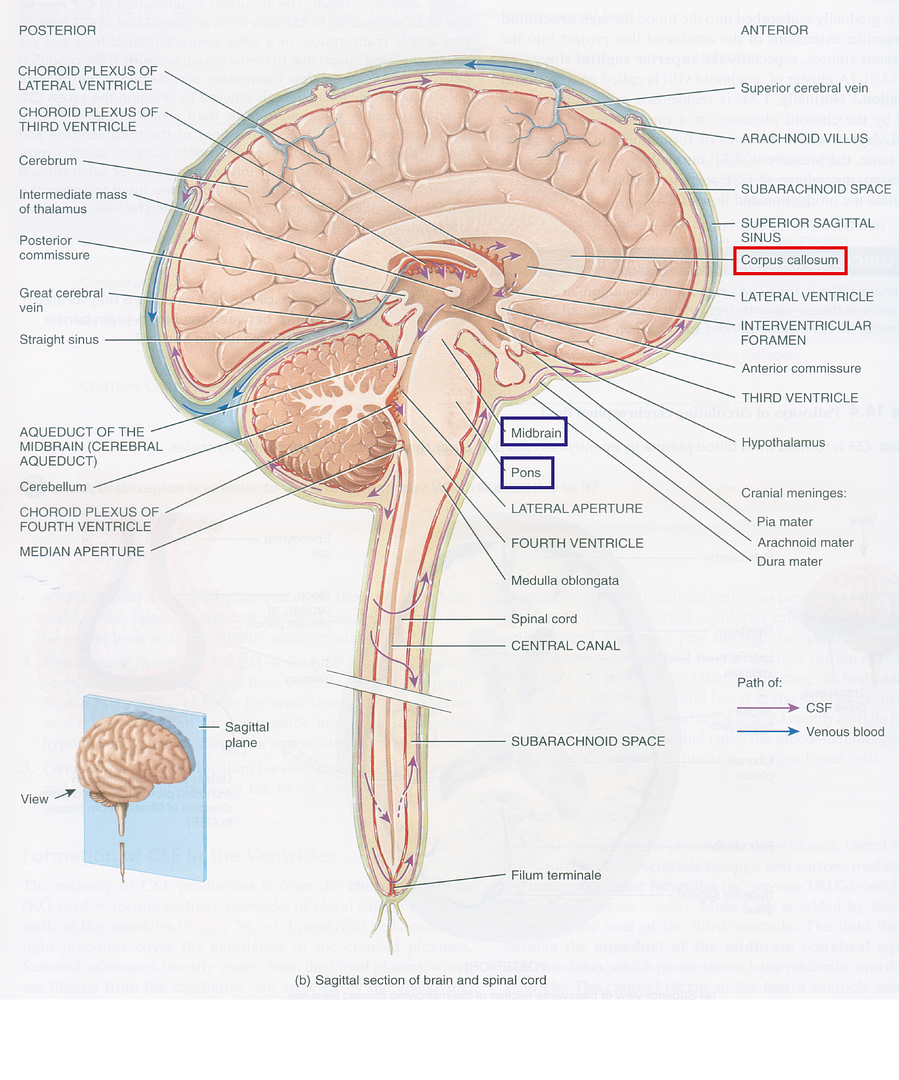
It is also of interest that the area in question is right next to the Cerebellum. This was an area of importance to the Parkland doctors. Comments on the Cerebellum caused a lot of grief to the Parkland doctors. However if damage in the brain was as low as this and that close to the Cerebellum I am surprised Cerebellum was not damaged.
The Pons is a substantial body, much more so than the Cerebellum and therefore I am beginning to believe that Cerebellum had to be damaged ( if a body like the Pons so close to it was torn ) and that the Parkland doctors were right all along.
Maybe the damage to the corpus callosum [boxed in red] is understandable, but the idea that the midbrain was torn from the Pons [boxed in blue] is what I find curious. What I find curious is how deep inside the brain the Pons is and how close it is to the Cerebellum. And that is why I believe Cerebellum had to have been damaged.
James
Dr. COE. Dr. Humes, looking at photograph No. 46, I am curious to know whether this destruction you feel is a postmortem artifact in removing the brain, or was part of this, was caused by the bullet you think perhaps? You have a junction between the cerebellum and the---
Dr. HUMES. No ; well, I think it was partly caused by the bullet.
Dr. COE. It was?
Dr. HUMES. It was great - it was a tearing type of disruption that basically had to go back to our description. The corpus callosum was torn, was it not Jay? And the midbrain was virtually torn from the pons.
Dr. COE. Thank you all.
Dr. HUMES. Now don’t misinterpret me that the missile necessarily passed through there because it was a great -
Dr. COE. But it must have come fairly close in there.
Dr. HUMES. Could have, yeah.
………………………………………………………………………………………………………………………………………
Dr. BADEN. You are completely satisfied - and Dr. Boswell - that there was no foreign object in this area?
Dr. HUMES. Absolutely, unequivocally, without question.
Dr. BOSWELL. Yes. HSCA 7 Addendum I P. 247
-
Bernice,
“..there is a great deal of evidence that a bullet was recovered from President Kennedy's body at the time of the autopsy..”
This point by Robert Groden makes no sense. It goes against everything we know so far. It would be great to discover that a bullet had been recovered. It would no longer be necessary to suggest that the bullet was removed from the body at some point prior to the autopsy.
Sibert & O’Neill make it clear that Humes was utterly confused when he had no bullets in the body to explain the wounds. The pre-autopsy X-Rays should no bullet in the upper chest area. In his HSCA interview Perry says that when he informed Humes about the throat wound, Humes replied “That explains it.” P. 306
In “In the Eye of History”, P. 186 Sibert denies he ever received a complete bullet or that one was recovered from the body. When O’Neill is interviewed he also denies a complete bullet recovered from the body.
So, although Robert Groden's comment would make it convenient had a bullet been found during the autopsy, evidence makes it clear that he is wrong and that no bullet ever was found during the autopsy.
James.
-
Don,
Great work. I had not been aware of your "Men of Courage" web site.
An outstanding version of Z206. I am amazed you could get such detail. I have been working on the throat wound and have been able to tie the shot down to Z204 onwards. The reasons are that the shot entered right of centre. That can be confirmed by Fox 1. It also slightly bent the trachea to the left. For such a wound to occur JFK would have to be sitting facing forward. He only does so from Z204 onwards.
I have heard you refer to a shot from the Daltex before. Can you elaborate a bit on your views for this shot.
Also, the Secret Service agent standing behind John Ready, Paul Landis - I have been wondering whether his presence [ given the very low angle JFK's head is at Z312 ] might seriously reduce to window for a head shot from the TSBD. Have you given any thought to that?
Thanks.
James.
-
Thank you James.
Now I can relate that Bronson frame to the Willis 5 photo which was taken at Zapruder frame 202.
Does Trask say when the Towner # 3 photo was taken?
Mike
On P. 218 Trask says that it was several minutes later that Towner #3 was taken
This by Don Roberdeau might help.
http://educationforum.ipbhost.com/index.php?showtopic=14115
I have seen other charts that time stamp the images. I sure Don has done others
Hope this helps.
James.
-
Does anyone know which Zapruder frame is equivalent to this Bronson frame?
Mike,
Trask suggests that image is somewhere between Z220 - 225.
I would certainly look more towards Z225 that Z220.
I feel it might even be Z226. In the Bronson image we see:-
a) The umbrella up.
The Cuban's arm right up. Which it is not in Z225c) The American Flag, on the car, unfurled.

It could also be later, but Trask is usually very accurate
Hope that is of help.
James
-
The Demise
Of
The Single Bullet Theory
Although the title may be a little pompous, I am convinced that I have discovered a fatal factor that critically undermines the credibility SBT.
The Achilles heel of the SBT has always been that point when the bullet traversed the upper chest area of JFK: the least examined element of the theory.
For those who want the conclusion at the beginning:-
The SBT states that a shot fired from the 6th floor east window of the TSBD struck JFK in the upper right back. This bullet then travelled through his body exiting his throat between Trachea rings 3 & 4. The bullet then continued to inflict five more injuries on John Connally.
Malcolm Perry, Charles Carrico and Commander Humes are all on record stating that the bullet either entered or exited through the Trachea. If the bullet entered the Trachea then, at some point, it had to exit it.
I can now prove that the bullet did so through the rear of the Trachea. Such a point is fatal for the SBT. This is so, because this area is hidden from view by the Cervical spine. There is no way a bullet entering the back, even where CE 903 places it, could reach this area of the Trachea. This point is blocked from the bullet’s path by the Cervial spine and the gap between the Trachea and the Cervical spine is extremely narrow.
This highlights one of the critical weaknesses of the advocates of the SBT. The details of what had to have happened had a bullet actually travelled through the upper chest area of JFK has not been one they have given any thought to. And that is the difference between generalised theorising and detailed study.
What follows is a description of the Path of the Bullet from the throat to the back:-
Although the SBT’s path is in the reverse order, it is easier for me to examine this path from front to back.
See Group Image 1 below:-
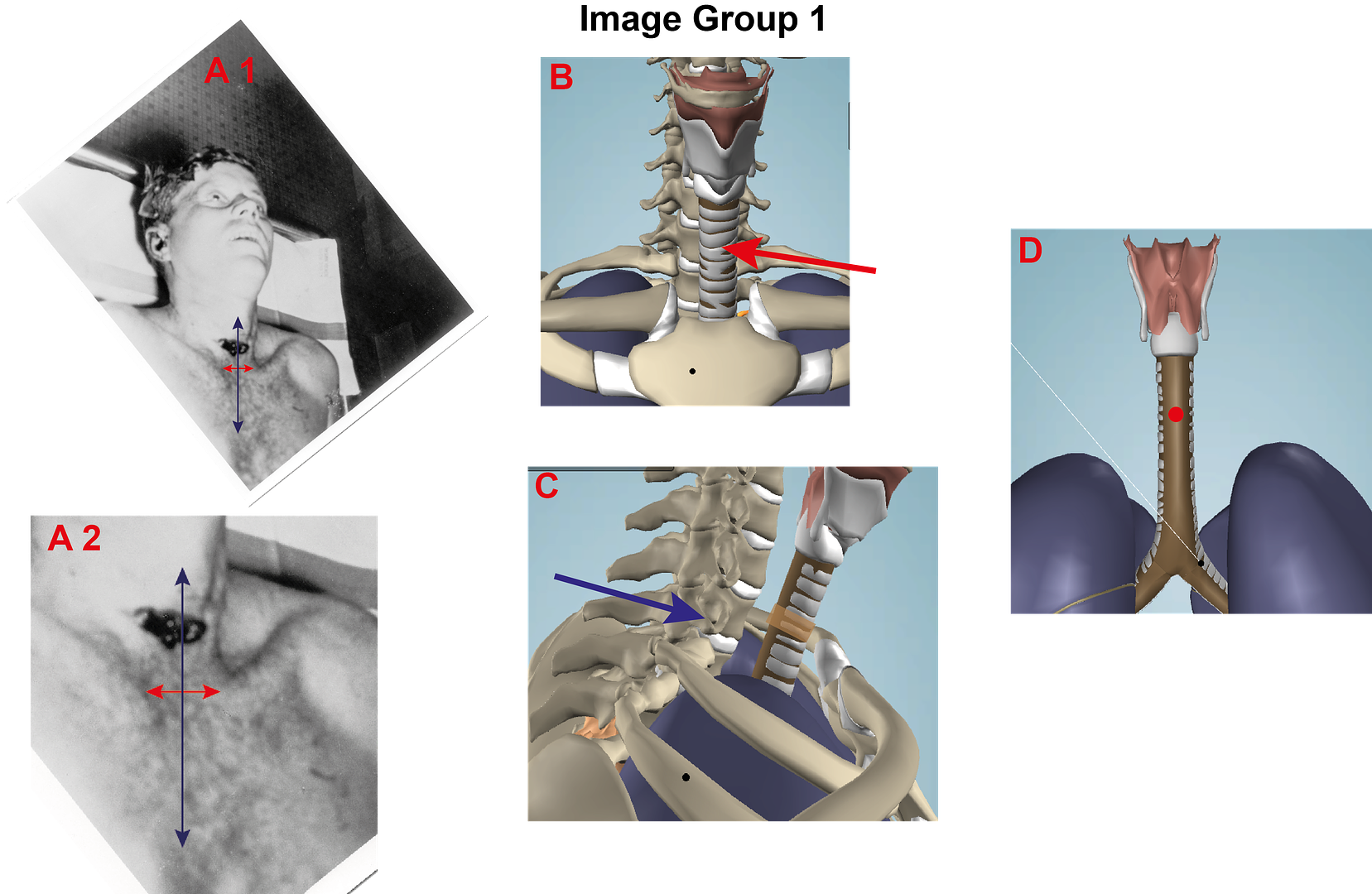
What you see:-
Image A1 is a rotated version of FOX 1 with a line drawn down the body’s center
Image A2 is a close up version of A1
Image B is an image of an anatomical model with an arrow pointing to Trachea rings 3&4
Image C is an image of an anatomical model with the bruise to the trachea highlighted
Image D is an image of an anatomical model showing the bullet’s exit point on the rear of the trachea.
1. Where did the bullet enter/exit the throat:-
Charles Carrico, the first doctor to see JFK, states that the wound was slightly to the right of the midline.
“This was probably a 4-7 mm. wound, almost in the midline, maybe a little to the right of the midline, and below the thyroid cartilage.” H6 P. 3
See Image group 1 images A1 and A2.
Carrico’s statement can be verified with FOX 1. See image A1 and magnified A2. What I did was draw a line between the two Clavical bones. The Red Arrow. Then I drew a vertical line through the middle of the red arrow. This may not be strictly accurate, but it is sufficiently accurate to verify that the bullet entered right of center.
2. Where did the bullet go next:-
See Image group 1 Image B
Because JFK was not breathing Dr. Carrico decided to insert an Endotracheal tube. While inserting this tube Dr. Carrico was able to glimpse the Trachea. He said that through the larynzo scope he saw “ a ragged wound of the trachea was noticed immediately.” CE 392 P. 4 + H2 P. 362
The importance of this statement is that first the report was written 3 hours and 20 minutes after JFK had been pronounced dead and 45 minutes before the plane carrying JFK’s body landed in Washington. Second this is noticed prior to Malcolm Perry entering the room and performing the tracheotomy. Therefore the damage cannot be ascribed as a consequence of the tracheotomy.
Malcolm Perry backs up Charles Carrico. In his testimony, he stated that he “noticed a small ragged laceration of the trachea on the anterior lateral right side.” H3 P. 370
This is important not just because he backs up Carrico, but like the bullet’s entry on the throat, the entry into the trachea is also right of the midline.
Malcolm Perry makes another observation. The impact of the bullet striking the trachea bent the trachea slightly to the left. The trachea was “deviated slightly to the left.” H6 P. 10
This bending of the Trachea is supported by Carrico in his HSCA interview on January 11th 1978 he commented, “I noticed at that time probably some deviation of the trachea to the left, very slight.” HSCA 7 P. 268
3. So where did the bullet go next:-
Once inside the trachea there were only four things the bullet could do.
i. It could remain in the trachea stuck.
ii. It could change direction and veer to the left.
iii. It could change direction and veer to the right.
iv. It could carry on forward.
1. Since no bullet was ever found in the body, the bullet clearly did not remain in the trachea.
2. There was no damage to the left side of the body, so it clearly did not veer left.
3. So did the bullet veer to the right?
In his HCSA interview in 1978 Carrico comments that he “saw some modest amount of hematoma in the recesses to the right of the trachea.” HSCA 7: P. 268 + H4 P. 360 So although Carrico saw bruising on the right side of the Trachea, he did not see a tear.
This bruising is illustrated by Image group 1, image C.
In his testimony and autopsy protocol Commander Humes made no mention of a tear of the lateral (right) portion of the Trachea.
Therefore the bullet did not veer to the right.
That meant that bullet exited the Trachea through the back. This is illustrated by Image group 1, Image D. the red dot indicates the point at which the bullet exited the Trachea.
4. What evidence is there that the bullet did indeed exit through the back of the Trachea and what impact did that have?
Just beyond the Trachea is the Spinal column and between the two there is very little space. Any missile exiting the rear of the Trachea would have no option but to strike the Cervical spine. There is not the room for it to veer to the right to avoid striking the spine.
Image Group 1, image C gives an idea of the short distance between the Trachea and the Spinal column. Image Group 1, Image C shows that the Cervical Vertebra 7 (C7) is on the same plane as Trachea rings 3&4. This highlighted by the blue arrow.
See Group Image 2 below:-
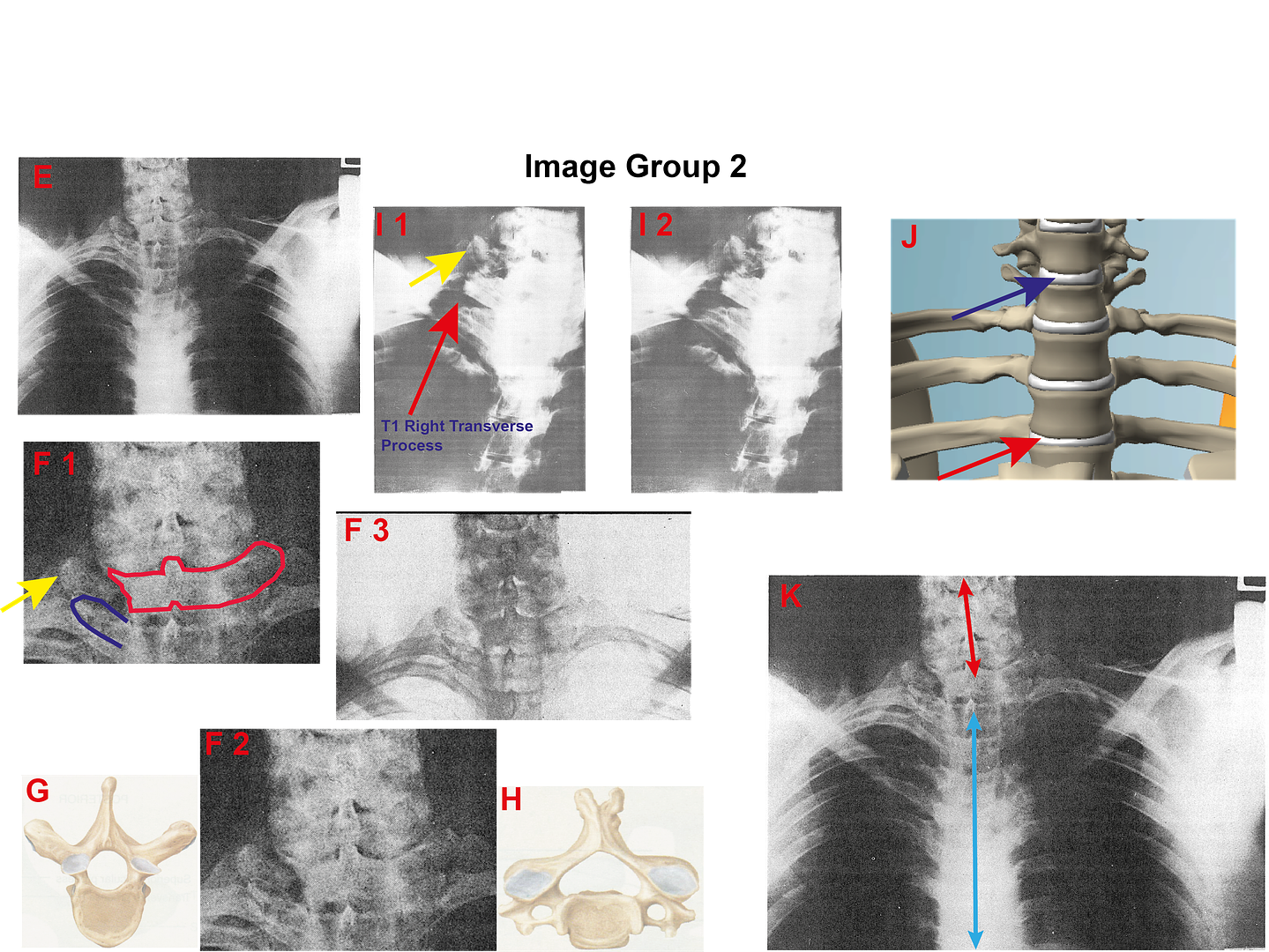
What you see:-
Image E is X-Ray 9. It was taken prior to the beginning of the autopsy taking place.
Image F1 is an annotated cropped version of X-Ray 9.
Image F2 is a clean copy of the cropped version of X-Ray 9 for you to verify my findings.
Image F3 is a clean negative copy of the cropped version of X-Ray 9. It highlights the data of the XRay in a different way.
Image G is a drawing of a Thoratic Vertebrae. The two wings are referred to as the vertebrae’s Transverse Process’s.
Image H is a drawing of a Cervical Vertebrae. The two little grey cups are referred to as the vertebrae’s Transverse Process’s.
Images I1 + I2 are cropped copies of XRay 8 that was taken at the suggestion of Pierre Fink when Humes informed him that he was puzzled he could find no bullets. The autopsy was well under way when this XRay was taken. I1 is an annotated version, I2 is a clean version.
Image J is a model of the of the upper chest area of a human skeleton.
Image K is an annotated version of XRay 9.
Without digressing too much, in 1978 when the HCSA examined the case one aspect that they were concerned with is arrowed in yellow in Group 2 images in E and I1. Basically they did not know what it was and during the months of February 1978 to August 1978 the Committee contacted four Professors about this problem: Professors Chase, Seaman, McDonnel and Davis. There was considerable dispute between these four Professors as to what they were seeing. Members can read their reports in HSCA Vol 7. In the end the opinion of the Committee was to cite Professor McDonnel: “The panel noted an interruption in the continuity of the right transverse process of the 1st thoracic vertebra much more clearly delineated in the computer-assisted enhancement of film No 8.” HSCA 7 P. 98 Number 8 XRay is image I.
Unfortunately, the HCSA omitted from their reference to Professor McDonnel, his hedging. The Professor was not sure whether what he was seeing was T1 or Intervertebral disk C6 C7. HSCA Vol 7 P. 219 Addendum C You can see an example of such a disk which is arrowed in Red in image J. The particular disc he is talking about is the one between C7 & C6 cervical vertebrae’s. This is arrowed in blue. This comment was omitted from the report and so the HSCA report is on record stating that what was damaged was the right transverse process of T1.
Unfortunately they were wrong. Professor McDonnel was right when he suggested it could be C7.
What had got the committee so curious is the anomaly highlighted in yellow in Images F1 & I1. That is the reason they contacted the four professors. Although these vertebrae’s are next to each other, they are also very different. If you look at Image G, a drawing of a Thoracic Vertebrae, you will see that it has unique wings for its Transverse Process. You will also notice that the Transverse Process of the Thoracic vertebrae is very different from those of Cervical Vertebrae.
Although the C7 vertebrae is right above the T1 vertebrae they are distinguishable from their positions on the bodies spine.
If you look at Image F1, you will see that I have highlighted an area blue. This is the right Transverse Process of T1. In both F2 & F3, you can clearly see an outline the image of the Transverse Process that I have drawn around. If you look at image I1 you can see, arrowed with the Red arrow, the Process even more clear, and in particular the unique wings of the Process
In image F1 you can also see this anomaly which appears to be adjacent to the T1 Process. However images I1 + I2 lets you see that this anomaly is not adjacent to the T1 Process, but above it. And what is above T1 is C7
What appears to have happened is that when the bullet exited the rear of the trachea, it struck C7 Cervical Vertebrae. This is outlined in Red on image F1. Image F3, the negative version, gives a clear account of the damage to the vertebrae. The complete right transverse process has been destroyed. There is nothing there to be seen.
But it is even worse than that. It is not just the C7 process that has been destroyed; the Intervertebral disk C6 C7 ( that lies above it ) has also been destroyed.
How can we say, that disk has been damaged? These disks of muscle support the vertebrae’s above and below: and together they support the neck and the head. If you look at image K, you will see that the entire neck has collapsed to the right exactly where C7 is. The destruction of the muscle is what has allowed the neck to fall. It is no longer there to support to support the neck and that is why the neck has fallen. XRay 9 was taken before the autopsy began, so the damage cannot be ascribed to the work of Commander Humes.
No one can say precisely when the neck dropped onto T1, but it was sometime between the assassination and the body arriving at Bethesda and being X-rayed. Most likely it was when the body was laid in the coffin in Parkland to be flown back to Washington.
But there is no documentation that the back of the Trachea was damaged:-
That is true, but what is equally true is that Commander Humes did not dissect the throat area. He was completely unaware that the throat wound was anything more than a Tracheotomy, until he conferred with Malcolm Perry. At that point it was too late to examine the wound. So to suggest that, because the Autopsy protocol says nothing about a wound in the back of the Trachea, means there was no wound: that is wrong. There is no mention of a wound in the back of the Trachea, not because there was none: it was because the back of the Trachea was not examined.
And XRays 8+9 make it clear that damage was done to the cervical spine. And evidence makes it clear the bullet exited the rear of the trachea. Together they are proof that although there is no mention of damage to the rear of the trachea in the Autopsy Protocol, there was indeed damage to the rear of the trachea.
5. What has this to do with the SBT:-
It has everything to do with it.
i. Testimony has established that the bullet entered the trachea.
ii. It has been established that the bullet exited the trachea through the rear of the trachea.
That means for the SBT to be viable, the bullet must:-
i. Enter the body above the shoulder bone. Any lower and the bullet will pierce the lung.
ii. Pass above the lung and bruise it.
iii. Damage the C7 vertebra and intervertebral disk C6 C7.
iv. Enter the trachea between the Cervical Spine and Trachea.
v. Exit the trachea between trachea rings 3 & 4 and damage the right strap muscle.
vi. Exit out the throat, and continue on its journey to wound John Connally.
I’m sure many imaginative arguments can be made for much of the above. But no one can show how a bullet moving from back to front can squeeze between the Cervical spine and the Trachea. That is one of the criteria for the SBT as it travels through the upper chest because we know it exited out of the trachea. So if the bullet cannot be shown to enter the trachea from the rear then the theory fails.
That is the world of difference between the external trajectories ( from the TSBD to JFK’s back ) and the internal trajectory through the neck. The external trajectories have no obstacles in their path: the internal trajectory is full of obstacles all of which must be met.
And that is why the SBT fails and must fail.
James.
 Nor have I included the real exit point through the throat, which had to be the rear of the trachea. You will find that in my article at the JFK Assassination Forum in the articles section. The article being “The demise of the SBT” You will see there my arguments for the bullet having to exit through the back of the trachea. As far as the SBT goes, that means that the bullet has to enter the trachea through the rear of the trachea. An utter impossibility.
Nor have I included the real exit point through the throat, which had to be the rear of the trachea. You will find that in my article at the JFK Assassination Forum in the articles section. The article being “The demise of the SBT” You will see there my arguments for the bullet having to exit through the back of the trachea. As far as the SBT goes, that means that the bullet has to enter the trachea through the rear of the trachea. An utter impossibility.
Lifton and Morningstar, nice but no cigar.
in JFK Assassination Debate
Posted · Edited by James R Gordon