

James R Gordon
-
Posts
1,111 -
Joined
-
Last visited
Content Type
Profiles
Forums
Events
Store
Posts posted by James R Gordon
-
-
I agree, this poorly researched juggernaut appears to be unstoppable.
Whatever credible evidence is presented to counter this ludicrous claim is just summarily dismissed.
Everyone else is wrong, while Ralph and Jim Fetzer are always right.
I would like to think this nonsense will end soon, but I fear we are just at the very beginning.
James
-
Even as your harshest critic I'm still a big fan! Thanks for the models, James!
Cliff,
Since in you previous post to this you were again quite severe I feel it might be worth walking back over previous discussions.
See image below:-
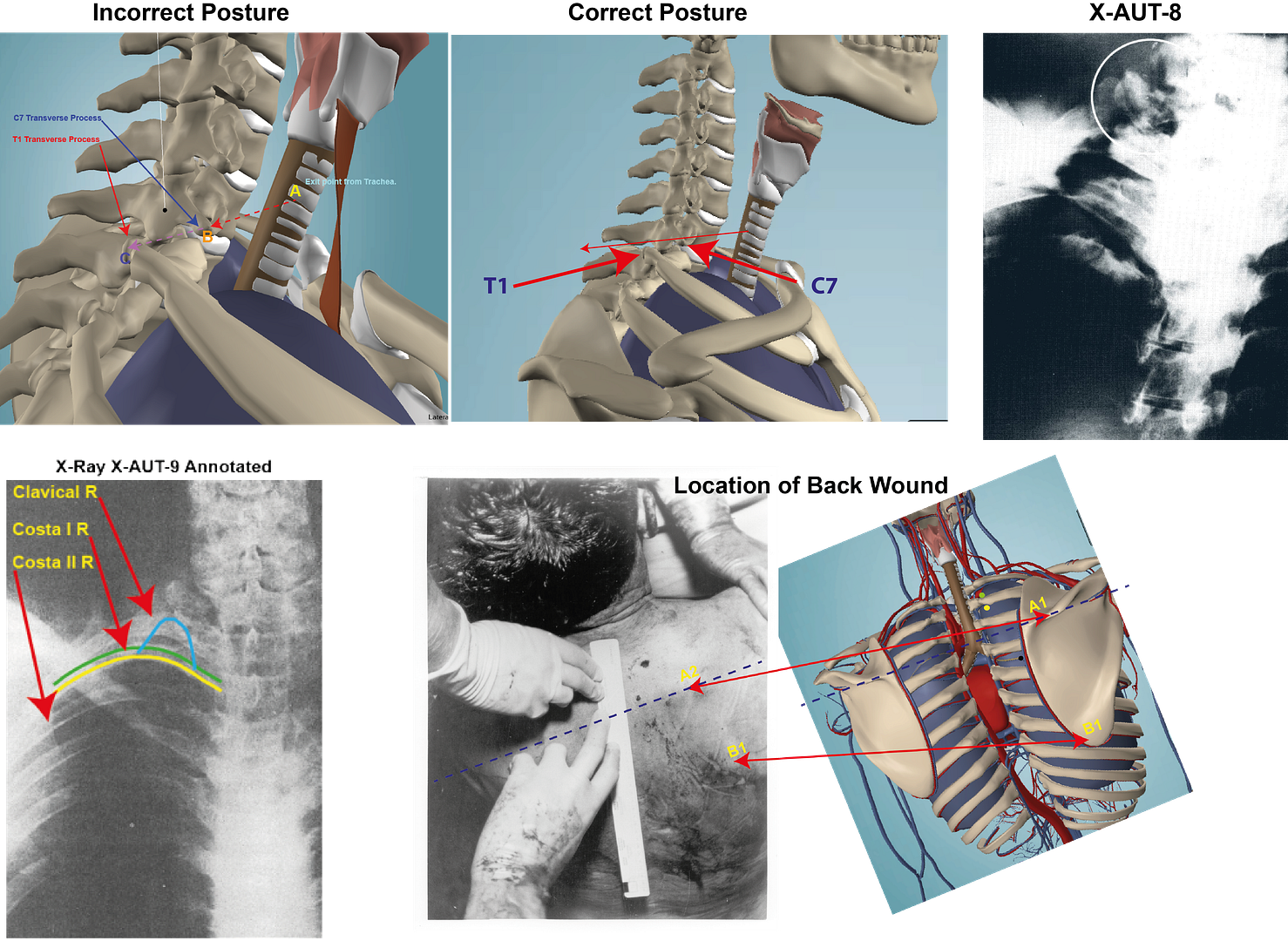
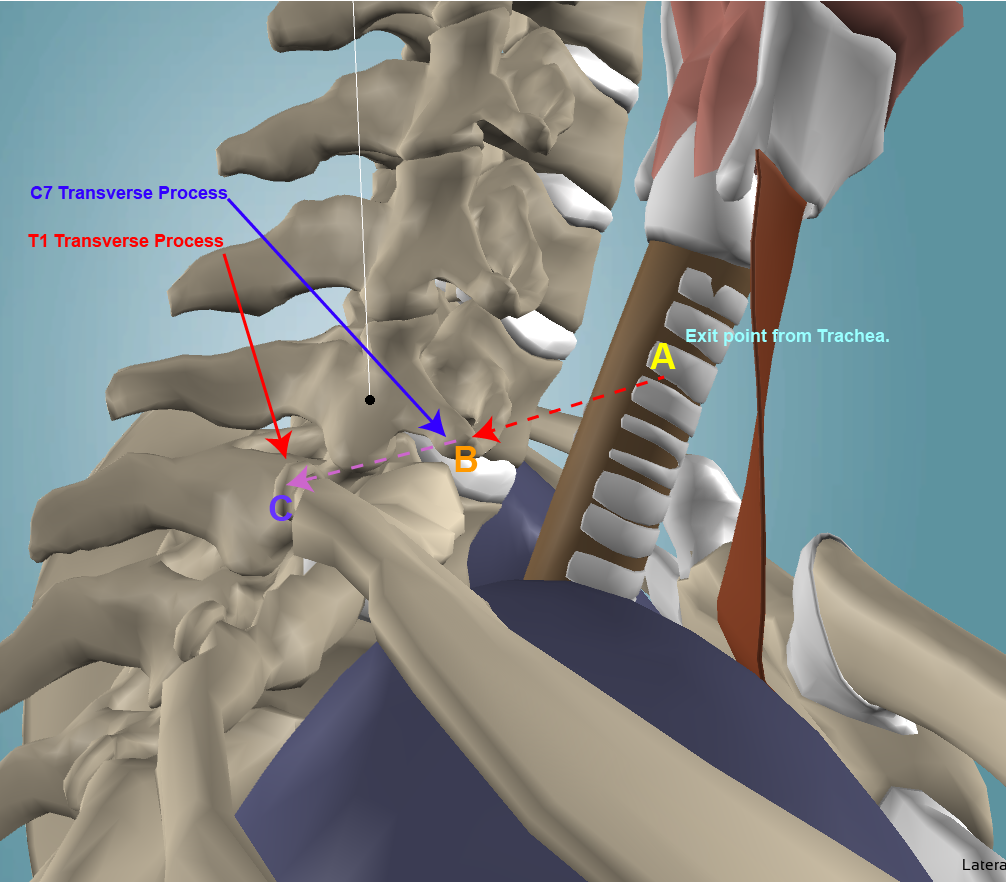
First I need to point out to you, I believe I have already done so, that the model you are so pleased with has incorrect posture. The model [labeled “Incorrect Posture”] is leaning forward. That was my mistake, I did not notice what I had done. The importance of this mistake is that is the only reason that C7 and T1 are reached.
James, your model is merely an approximation of JFK. There has to be a degree of variation, no? The x-ray shows a fracture at the T1 TP and an air-pocket overlaying the right C7 and T1 TPs. That air pocket points in the general direction of the nicked trachea. Co-incidence? You cannot presume that the round would take a perfectly straight line while damaging blood vessels, can you? No change of posture is going to significantly alter the trajectory from C7 TP to T1 TP.
Cliff, it is true that there is an element of approximation in the models....but only an element. In the essentials they are accurate.
First, the change in posture is going to make very significant difference. By allowing the model to stoop somewhat you allow a direct angle from C7 to T1, that was not possible if the model is sitting up straight. It is the SBT, in reverse. By stooping his model in the car, allowed Dale Myers to create a trajectory between the back wound and the throat. Actually I have no idea how he got a back wound that appears to be around T2 to come out the throat, but that is another argument.
Second, blood vessels and arteries were not damaged. That is clearly stated in testimony and the autopsy report. That was at the heart of my argument that the SBT is not possible. By showing these arteries and vessels in the throat I questioned how any bullet was able to transverse that area and not hit any artery and vessel. I still wonder how a frontal shot is able to do, but seemingly it did. It is nothing short of a miracle.
If you look at the model [labeled “Correct Posture”] the line can pass over C7 but it is unable to strike T1. Although the images on Elm Street show JFK sitting upright, maybe you will want to change your view as to JFK’s posture when passing down Elm Street.
He was seated up-right. How does that significantly change the angle between C7 TP and T1 TP?
I have explained that above. The seated position makes all the difference in the world to trajectory analysis.
That aside, lets (for the sake of argument) assume that either models is able to meet with C7 and strike T1. For the sake of this argument I will grant you that.
The problem is that even if the bullet achieves that it leaves major areas unresolved.
a) The position of the lung is too low for it to be damaged, however you want to describe. X-Ray-AUT-9 outlines that damage. However you want to describe it, damage to blood vessels – whatever – it was damaged. It is not just Humes, I believe Fink also mentions it.
Finck mentions it, where? We're talking about tissue swelling, correct? There is nothing in the x-ray that precludes the swelling having resulted from damaged blood vessels rather than a damaged lung. The ONLY evidence of bruised lung is found in the testimony of a proven serial xxxx.
I'll find the Fink reference. You surely are not saying that the object that is pyramid shape in X-ray-AUT-9 (see in above post) that is outlined in Cyan is a damaged blood vessel. It is a unique shape for a bruised blood vessels. The main blood vessels and arteries, in that area, are inside the lung. What we see, outlined in Cyan, is exactly what Humes described.
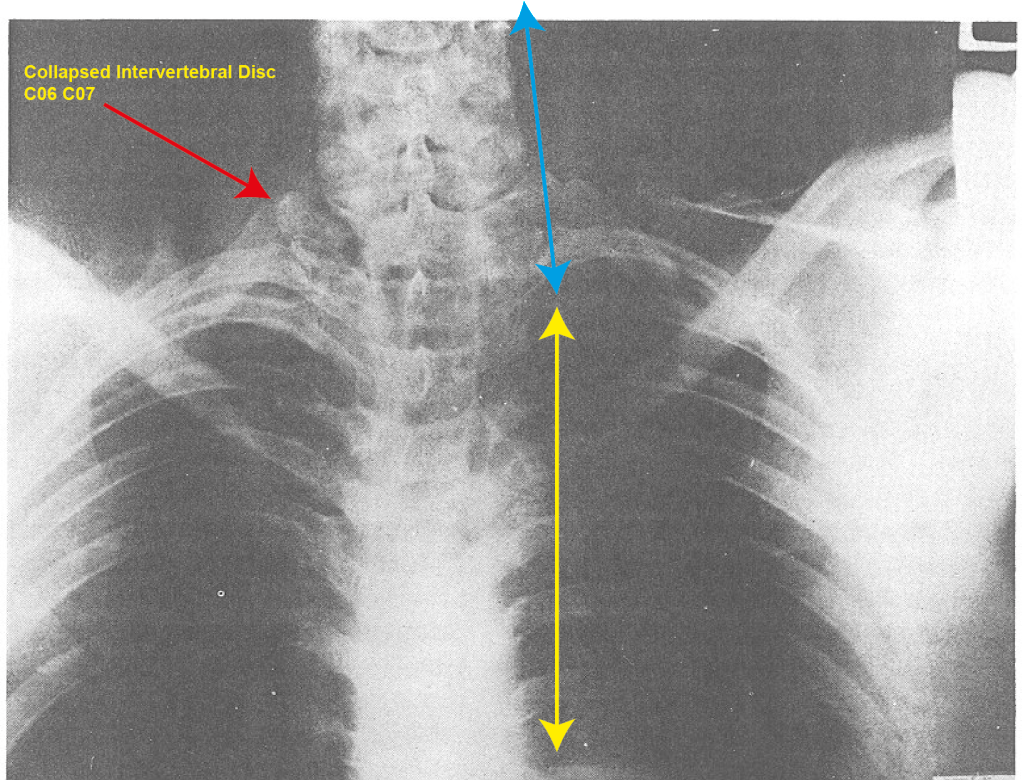
 The Intervertebral Disc C06 C07, seen in X-AUT-8 would not be damaged to the extent it is by the bullet’s just passing by. The X-Ray shows it is very severely damaged.
The Intervertebral Disc C06 C07, seen in X-AUT-8 would not be damaged to the extent it is by the bullet’s just passing by. The X-Ray shows it is very severely damaged.According to whom?
Well according to me, I suppose. But all you have to do is look at X-Ray-AUT-8 ( in post above). It is self evident that the C06-C07 muscle has been severely damaged. And what we are looking at is not C7 Transverse process. That can be clearly seen below it, as can C6 above it, although it is a bit blurred.
Unless you are suggesting that is how the muscle ought to look, it is clearly evident that it is damaged.
I agree with Pat, that the change in the posture of the neck was created when the body was placed in the coffin in Dallas. However, the fact that this change in position of the neck could take place at all, indicates the damage to C7.
Your argument is that C7 was not damaged. If so how was the Intervertebral Disc C06 C07 damaged and how could the neck change its position and end up sitting on top of T1 if there had been no damage in this area?
Correct me if I'm wrong -- but disc damage is according to *your* reading of the x-ray? I haven't noticed anything in the medical record about disc damage. Could you provide a citation?
Search for Transverse Process in Vol 7 and you will find references to it. One that caught my attention is P. 170 Vol 7. There is mentions that had a missile been several inches away from C7 (and you suggest it passed close by, and indeed has to to have contact with T1) these muscles would suffer severe damage. Since the bullet was much closer than that it is clear massive damage would occur. HSCA, talking about X-AUT-8, suggest what I indicate is the damage muscle is actually remnants of the bullet. I have gone and lost the reference for it. I admit I am no medical expert, and I am going to have to talk to some to ensure what I think I see is actually that. However I cannot see how the defect in that X-Ray is anything other than the C06-C07 muscle. I was reading yesterday, and again I have lost the reference, how the HSCA stated that what we see in X-ray 8 (the 8:30pm X-Ray) was not seen in X-Ray-9 ( the X-ray before the autopsy began). Unless I have miss-read the X-Ray it is a plain as a pike staff. I posted them in this thread somewhere.
As I mentioned earlier, I am going to have to seriously study this to see what they say, and most important, why they are saying it.
c) Now on this description I grant you that T1 has been damaged. But am I not correct that the damage was on the other side of T1, the external not internal side? How was the damage created on the external side if through this description it is the internal side that has been damaged?
Are you correct?
I assume that came from you. The HSCA state it can be seen in the X-Rays. I don' t see how because X-rays 8 + 9 don't show that part of the body. I'll check again, maybe I missed it.
d) With regard to the back wound, although I place the wound nearer T2, it is still close to T3, which is where you want it placed.
Great! Progress. At T2 the wound is to low to account for the C7/T1 air-pocket.
The HSCA in Vol 7 also talk about this air pocket.However they go on to suggest that it was the wound to the Trachea that created it.
It is often your custom to dismiss arguments you disagree with by stating Humes is a xxxx or certain data items are not to be trusted.
I have accepted that the bullet missed C7 and went on to strike T1. Why don’t you do me the curtsey of making an attempt to address these areas? For a shot to enter from the front, it is not just a matter of it missing C7 or striking T1, it must cause major damage to the muscle above C7.
Again, is this your reading of the x-ray?
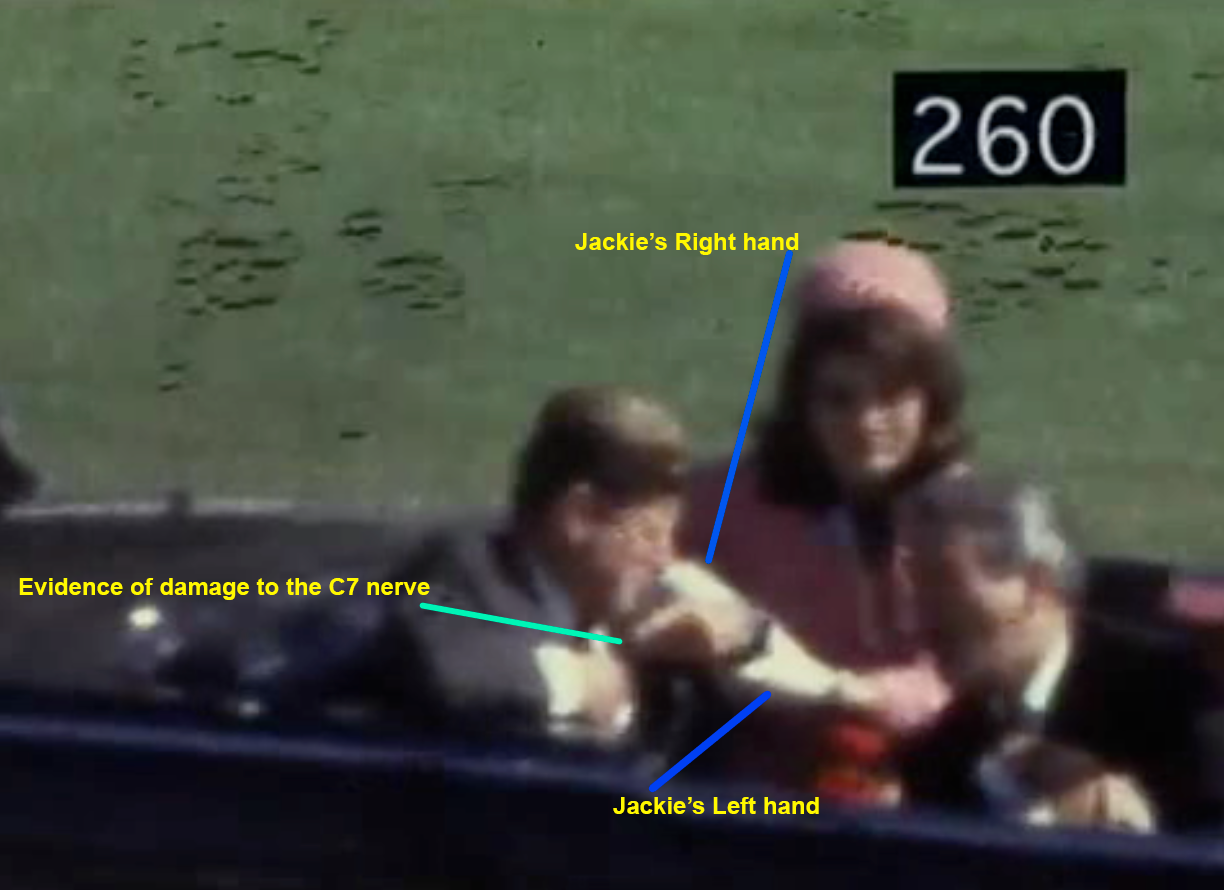
Yes, that is exactly what I am saying. But you can see that X-Ray it is in the above post. You are surely not suggesting the anomaly is a broken blood vessel. It importance is that connected to these muscles are the Cervical nerves. The C7 nerve, I understand has implications for the movement of arms and hands. Now they clearly are not functioning properly which leads to the conclusion that damage was done to the muscle and interconnected nerves.
It is mandatory that it is damaged, because it is the damage to the muscle and the interconnected cervical nerves that cause the arm movement we see JFK make after the bullet struck. They cannot be ignored.
Looks to me like he's making very specific movements with his hands -- the left index finger grasps at his collar-line, the right hand is cupped in front of his mouth. Those are conscious actions, not neurological responses.
This is not serious. You are seriously not suggesting that what JFK does with his hands and arms, after Z 224/5, are conscious actions?
The lung was also damaged. However your flight path for the bullet, takes it too high to do that kind of damage. If the lung was where Humes places it in CE 385, then yes it probably could be damaged.
So, it would be nice if this time you did not resort to the easy “cop-out” by calling Humes a xxxx or stating that the data evidence is fabricated.
What's changed?
Between you and me, probably not a great deal.
James.
-
Sure James. I'm interpreting the finger as the sunlit part of a deliberately gripping fist of both lapels to pull them apart. The thumb is behind the left lapel and the other three fingers in shadow.
John,
I have given quite a lot of thought to your suggestion that JFK is grabbing onto the lapels of his jacket. I can see how you came to that idea, but when you look over other frames he does not appear to be doing that. See image below:-
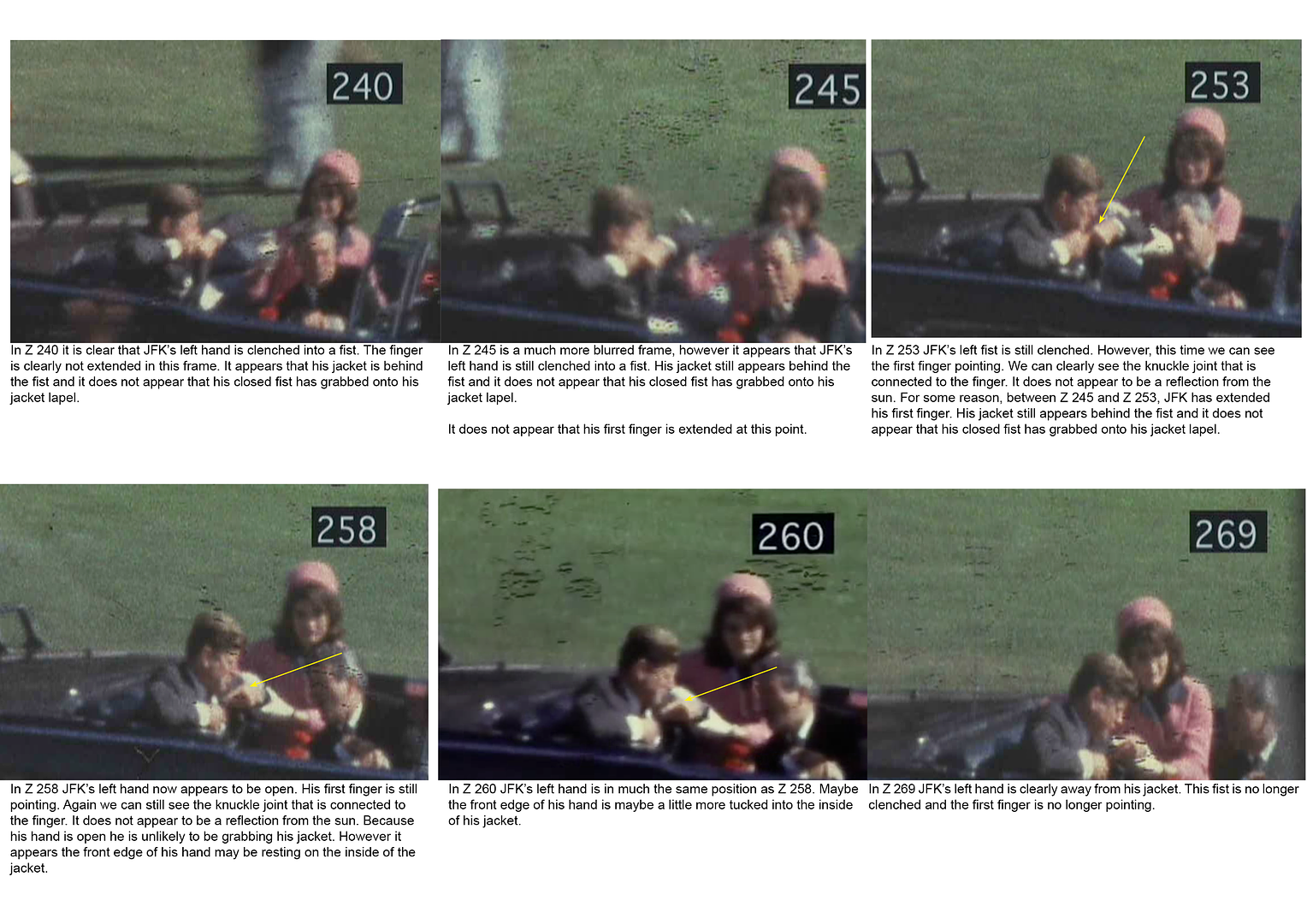
In Z 240 he appears to have left hand fully clenched. And in that frame he is too far away from the jacket to be holding it.
In Z 245, if anything he is even further away from the jacket.
In Z 253, we see the finger. It really does look like his first finger. We can see the fingers join to the knuckle. The finger itself does not appear to be the consequence of reflection.
In Z 258, the finger is even more visual. That said I may be mistaken in suggesting it is the first finger. In this image it looks like that hand is open. What I am suggesting is the finger might actually be the thumb.
Z 260 is the image that you believe the fist is grabbing onto his jacket.
In Z 269 we can clearly see that the hand is partially open and quite a distance from his jacket.
Overall, I understand how you came to your conclusion, but I am not sure it is the case. Looking at these images, what do you now think?
James.
-
Even as your harshest critic I'm still a big fan! Thanks for the models, James!
Cliff,
Since in you previous post to this you were again quite severe I feel it might be worth walking back over previous discussions.
See image below:-
First I need to point out to you, I believe I have already done so, that the model you are so pleased with has incorrect posture. The model [labeled “Incorrect Posture”] is leaning forward. That was my mistake, I did not notice what I had done. The importance of this mistake is that is the only reason that C7 and T1 are reached. If you look at the model [labeled “Correct Posture”] the line can pass over C7 but it is unable to strike T1. Although the images on Elm Street show JFK sitting upright, maybe you will want to change your view as to JFK’s posture when passing down Elm Street.
That aside, lets (for the sake of argument) assume that either models is able to meet with C7 and strike T1. For the sake of this argument I will grant you that.
The problem is that even if the bullet achieves that it leaves major areas unresolved.
a) The position of the lung is too low for it to be damaged, however you want to describe. X-Ray-AUT-9 outlines that damage. However you want to describe it, damage to blood vessels – whatever – it was damaged. It is not just Humes, I believe Fink also mentions it.
The Intervertebral Disc C06 C07, seen in X-AUT-8 would not be damaged to the extent it is by the bullet’s just passing by. The X-Ray shows it is very severely damaged. I agree with Pat, that the change in the posture of the neck was created when the body was placed in the coffin in Dallas. However, the fact that this change in position of the neck could take place at all, indicates the damage to C7.Your argument is that C7 was not damaged. If so how was the Intervertebral Disc C06 C07 damaged and how could the neck change its position and end up sitting on top of T1 if there had been no damage in this area?
c) Now on this description I grant you that T1 has been damaged. But am I not correct that the damage was on the other side of T1, the external not internal side? How was the damage created on the external side if through this description it is the internal side that has been damaged?
d) With regard to the back wound, although I place the wound nearer T2, it is still close to T3, which is where you want it placed.
It is often your custom to dismiss arguments you disagree with by stating Humes is a xxxx or certain data items are not to be trusted.
I have accepted that the bullet missed C7 and went on to strike T1. Why don’t you do me the curtsey of making an attempt to address these areas? For a shot to enter from the front, it is not just a matter of it missing C7 or striking T1, it must cause major damage to the muscle above C7. It is mandatory that it is damaged, because it is the damage to the muscle and the interconnected cervical nerves that cause the arm movement we see JFK make after the bullet struck. They cannot be ignored.
The lung was also damaged. However your flight path for the bullet, takes it too high to do that kind of damage. If the lung was where Humes places it in CE 385, then yes it probably could be damaged.
So, it would be nice if this time you did not resort to the easy “cop-out” by calling Humes a xxxx or stating that the data evidence is fabricated.
James.
-
John,
Thanks for the link and document. I don't feel it is Thorburn's Position.
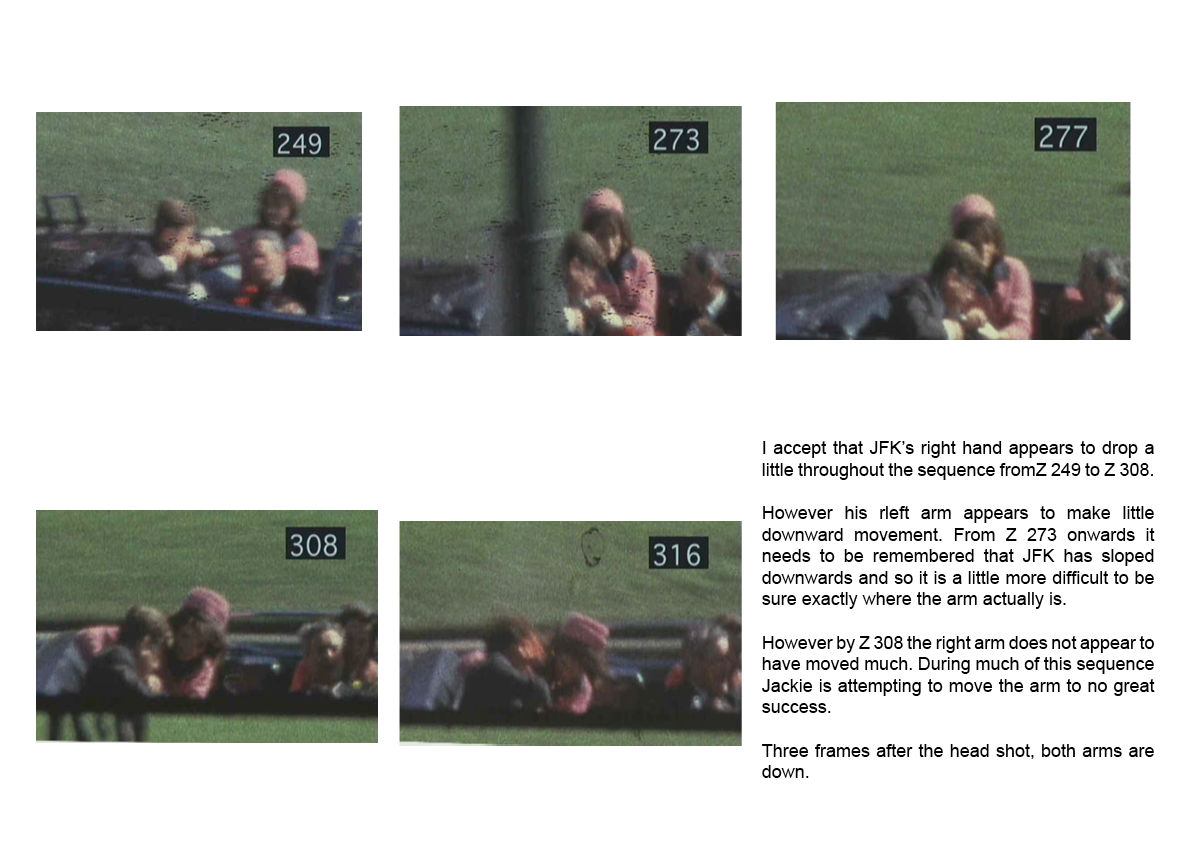
As I understand it, this theory suggests that the arms are locked once it takes effect. However between Z 225 to Z 312, JFK's arms constantly change position, even though basically they remain towards the upper part of his body.
I am about to start a massive amount of reading to examine what I have said has merit and what does not before I begin the work of collecting this study together. I believe I am onto something, but I now need to see what has merit and what may not have merit.
Again thanks.
James.
-
JFK was left on his own. It was up to him to save his own life. Under those circumstances, using a paralytic for the first shot makes perfect sense. If the SS does nothing, his only defense was to duck. The paralytic shot would have removed that option. JFK was upright and immobile as the Limo creeped into the Kill Zone.
The flechette scenario fits the damage seen on the x-ray like a glove. The round entered between the 3rd and 4th trach rings with a straight shot to the right T1 transverse process right over the C7 transverse process, accounting for the T1 fracture and the air-pocket overlaying those structures. Significant possible hematoma noted on the x-ray, consistent with damaged blood vessels in the flechette's wake.
Cliff,
You say the bullet went right over the C7 TP. In the model, you are using, it is going under. We're the bullet to be above C7 it would totally miss T1.
This air pocket, that you refer to, was created long after the bullet completed its journey. After all the air had to have come from the damage to the lung.
And if this bullet, had completely missed C7, that leaves the problem of the C6 muscle above it that is shown to be severly damaged. In case you are tempted to suggest that that muscle is not a muscle, but actually a hematoma, remember that when x-ray 8 was taken the lung had been removed and therefore so had the hematoma, which was attached to it.
James
-

John,
I am not clear what point you are making.
Could you elaborate please.
James.
-
As far as the "middle finger", is that really what we're looking at? I'm not so sure. It seems too long. What is shown in the frames leading up to this one?
Pat,
I agree that it would help to see all the images with the finger pointing: Z 256 - Z 262.
Below you will see a montage of these frames. I have deliberately made it a large image so as to be able to closely examine what we are seeing.

It looks to me, that it is not JFK's middle finger, but his first one.
What is your view?
James.
-
Pat,
I thought I made it clear that the “Thorburn Reflex” was not necessarily my position. I certainly intended to make that clear. Having said that, what is described as this “Reflex” perfectly reflects what we see JFK doing with his arms.
The main point of my previous post was that the strange event of JFK’s arms were a direct consequence of the nerve damage when C7 was struck by the bullet. As I have pointed out the damage to that muscle is so extensive it was bound to have a consequence on the nerve structure attached to these muscle and the spinal cord directly behind the muscles. The reason I raised “Thorburn’s Reflex” was because that state suggests that once enacted it is difficult move the arms. The nerves that cause this don’t allow it. In the image below I have taken a series of frames to illustrate this point. Even with Jackie attempting to move the left arm it will not move. It is only when the head shot takes place, which destroys the entire nerve system, that the arms relax.
What I am trying to point out is that the impact with C7 did not just damage that Transverse Process, it also severely damaged the Intervertebral Disc C06 C07. And that damage had a major impact on the Cervical Nerves. It is that damage that caused the arms to rise and lock. They were only released when the entire nervous system was destroyed or severely damaged by the head shot.
With regard to the finger, I went back to the image to see whether I had miss-interpreted the image. It is clear to me that the object I pointed to cannot be anyones but JFK’s hand and most likely one of his fingers. It is clearly not anything to do with Jackie. Connally is too far away for it to be interpreted as something from him. That leaves only one possibility, it is JFK’s finger.
With regard to the damage to the Cerebellum, I only have this point. In the TV program “Nova” the Dallas doctors were taken to the National Archives to view the autopsy images. I can’t who, but after viewing one of the doctors stated that they were clearly wrong when they suggested that the Cerebellum had been damaged. The images made it clear that it was not severed.
James.
-
Thanks John,
Since I noted the damage to the C6 muscle, I have been looking in detail what would be the consequence of that damage.
I have to thank you for alerting me to the importance of the cervical nerves. That opened up a new avenue to be study.
What surprises me, is that the HCSA had very well qualified medical personnel studying this aspect of the case, yet their conclusions don't begin to examine the consequences of the throat wound: either as the SBT or as a frontal entry wound. For example they do mention the cervical nerves, but make no attempt to explore how their damage helps to explain what we see.
James.
-
Pat,
After some reflection I believe you are right. It is unlikely that in in the few seconds after the throat shot, that the neck changed its position. I suspect that the change in the position of the neck was a result of the body being placed in the coffin at Dallas.
Looking up the Internet for “Thorburn’s Position” I happened to notice this from David Von Pein’s web site:-
“We know that the spinal cord of JFK was not physically severed, nor was it damaged in any way at all. And we know that JFK is certainly reacting to a gunshot wound to his body at the time when he exhibits the "Thorburn" type of arm-raising.”
Reference:- http://jfk-archives....rm-raising.html
Boy!, is he wrong in what he says. Clearly not done his homework. I am not sure whether JFK is, or is not, exhibiting “Thorburn’s reflex” to give it it’s proper title. That said I found the following definition of the condition on the Internet.
“A reflex position assumed by the elbows immediately after injury to the spinal cord in the lower cervical region.”
And the damage is indeed in the lower cervical region.
What I found interesting was not Thorburn’s reflex per se, but the idea of the impact of the damage to the Intervertebral Discs C06 – C07 + C07 – T01. In seems absolutely logical to assume that the damage we see in X-AUT-8+9 had impact on the cervical nerves in that area. David Von Pein is absolutely wrong when he suggests that no damage was done there. Serious damage was clearly done. I have pointed out in previous posts the direct link to Spinal Cord from these Intervertebral Discs. There is a very high probability, seeing the damage that C7 sustained, that damage of some kind was also inflected on the Spinal Cord.
For example we all know the image of Z 260 when JFK’s finger is pointing to his throat. Some have suggested that this shows him pointing to the wound in his throat. He may well be also doing that, however the C7 nerve also controls the middle finger. I suggest that the movement of his finger is more a response to the damage to to the Cervical nerves connected to Intervertebral Discs C07 – T01 than an intent to point to the injury he has just sustained.
The “Thorburn Reflex” type reaction that we see after Z224/5 does not relax until after the head shot. In those moments before the head shot Jackie attempts to get JFK to lower his left arm. Right up until the head shot JFK resists, or more accurately his arm resists. I am beginning to wonder if the real reason he slumps to his left is a consequence of the arm resisting being pulled down. It is clear that what made JFK raise his arms in this way, is a direct consequence of the damage to the Cervical Nerves as a result to the damage inflicted on Intervertebral Discs C06 – C07 + C07 – T01.
And that is proof that the Cervical nerves as well, to some degree, the Spinal column have been damaged by the bullet’s impact on C7 Transverse Process.
It takes the damage from the head shot and the total destruction of nerves system for the arms to relax.
James.
-
Richard,
I would like to make very clear, that I was not directing my response at you. I had no idea who was being referred to in the comment. I read the comment to be referring to the moment of the head shot.
Reading the full quote, I fully understand your point and agree with your description of what happened.
Sorry for the confusion.
James
-
John,
Thank you the positive comment.
Whoever said he JFK was upright at the moment of the head shot is absolutely wrong. It would appear to me that he had sloped to his left somewhere around 20 degrees, maybe even more.
You have highlighted an important point. Little research has been devoted to the combined affect of his daily medications along with such injuries as the neck wound. I have no idea what the combined effect of that would be. It would, of course, only be momentary. A few seconds later he would effectively be dead.
James.
-
James,when I referred to the neurological aspect in post 215,I was meaning to infer,what with the collapse of his neck that nerve compression was likely.Has you have pointed out,the damage was quite severe.
So in my mind,he would have been in a lot of pain through nerve entrapment.I have busted a few bones and its the nerves that give you the acute pain.Also I believe his body would have gone into shock.And that would naturally explain the lack of movement afterwards,and cervical neurological damage can cause paresthesia in certain areas.
Malcolm,
After posting this revised position as well as the video, I began to have doubts and went back to my work to check it again. I wondered if I had gone a little too far. However the more I study it and particularly the damage to Intervertebral Disc C06 C07, that damaged muscle, I am convinced I am right. The slope of the movement of the whole neck towards this damaged muscle suggests only one conclusion: the neck moved downwards as a consequence of the throat shot and the consequential damage to the said muscle. I can find no other explanation why the neck is at a different angle to the spline. The only explanation I can arrive at is that the whole neck collapsed down onto C7 because of this damaged muscle.
In the video, I looked at his arm movements as well as his movement to the left and tried to explain them as a consequence of the change in the neck's position.
However you may well be right that a further consequence of this change in the neck position was that JFK was incapable of movement. Many researchers have wondered why he never made any attempt to move. You may well have highlighted the reason. I think you have raised an important point here.
James
-
James,I have a neck fracture at C5,also a couple of prolapsed discs in my back.The one thing that does cause excruciating pain,and I am talking from experience,is nerve entrapment.If the bones on JFK's neck trapped the nerve,then he would get a pain like a electric shock going through his neck.I get sciatica from the prolapsed discs and no amount of pain relief stops that pain completely.It is a pain that is so bad that its hard to sleep.Unless you dope yourself up enough that it forces sleep.
Malcolm,
Thank you for your contribution. I am sorry you have such pain. I am sure JFK will also have been in significant pain. I have no way of knowing whether a nerve was trapped, but I do believe I have established that the muscle between C7 and C6 was very severely damaged.
This morning I wondered if the detail in my posting was just too much to follow. So today I have added a video that goes over what I had to say yesterday.
Hopefully it will be easier to follow.
James.
-
An Amendment to my position on the damage to C7 and T1
In the last few days I have been in discussion, on the Lancer forum, with Charlie DeArmonde about my work on the SBT. Although there has not been the amount of response in Lancer as there has been here, in the last few days Charlie contributed a number of important comments. The most important, and the trigger for this posting, was his feeling that any damage to C7 would be most likely to affect T1. In total the comment that Charlie made, which has made me reflect on my position is as follows:-
“This part of C7 is where the downward counter-balancing muscle between C7 and T1 is attached. Damaging this area would easily account for the upward derangement of the broken section of the right C7 TP. That is to say that the muscle between C7 and C6 is probably responsible for most of the actual dislocation of this fragment, as it would no longer be countered adequately by the damaged muscle between C7 and T1.”
I am very grateful for this comment by Charlie. By focusing my attention on the issue of the muscles it allowed me to understand something that had always puzzled me since I posted my statement on C7. At that time I had been curious what that point below the damaged C7 ( as I then called it ) was. This is labeled A1 is X-AUT-8. Eventually I just ignored it, and that was my fatal mistake in that posting. This was because, as I now realize, what I then called C7, was not C7 but the muscle above it, Interventebral Disc C06 C07. The object I could not understand and had eventually ignored is in fact C7. If you look closely at X-AUT-8, you can even see C6 above the damaged Interventebral Disc C06 C07 muscle.
See combined image below:-
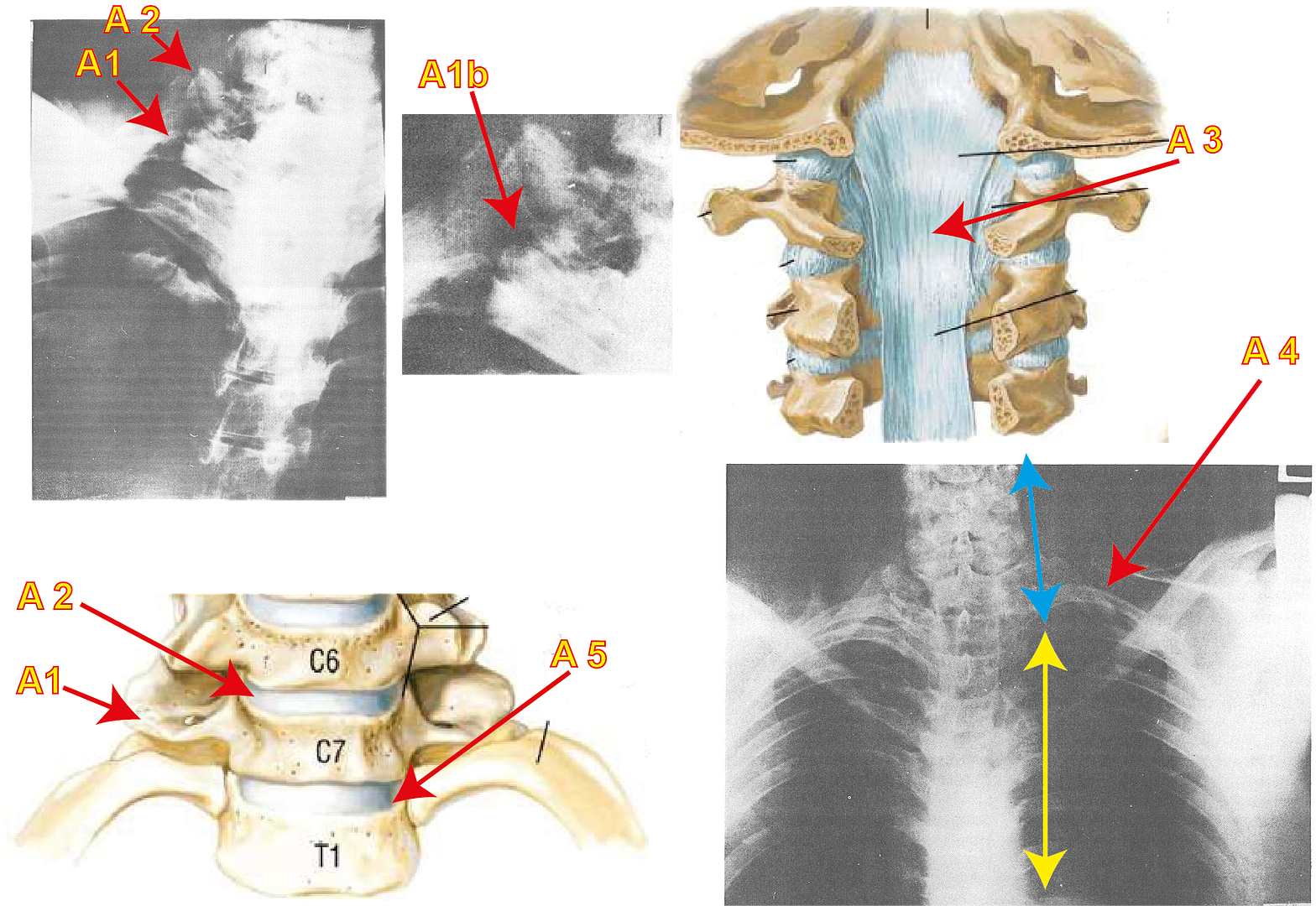
What does the Image show you:-
(1) X-AUT-8 has two pointers.
A2 points to the Interventebral Disc C06 C07
A5 points to the Interventebral Disc C07 T01
A1 points to C7
(2) X-AUT-8 shows a close-up of the damage to C7 as pointed to by A1b.
(3) Shows the back Trachea vertabrae’s and the Temporal Membrane. This is highlighted by pointer A3.
(4) Shows a close-up of the Trachea and points out Interventebral Disc C06 C07 pointed out by A2 and the C7 Transverse Process pointed to by A1
(5) Shows X-AUT-9. With the help of arrows the slope in the neck is highlighted.
So what is my amended position?
In this description I will invoke three kinds of statements.
a) Fact. This is where the evidence, e.g. X-rays, clearly support the point.
Logical Assertion. This is where, although there is no factual evidence .e.g. an X-Ray, the logic of what must have happened is irrefutable.c) Assertion. This is where the point has no evidence to support it and the conclusion is debatable.
The first three points described are the same as in the original C7 positing:-
1. The bullet enters between Trachea rings 3&4.
This is a fact. The Autopsy report, the testimony of Commander Humes, the observations of the Parkland doctors all testify to this point
2. The bullet damages the right strap muscle as it passes it by
This is a logical assertion. Humes testimony and the Autopsy report state that this muscle was damaged. It can also be said that the trajectory of the bullet is such that it seems certain that damage would have been done to the strap muscle as the bullet passed by. However there is no external evidence to prove it.
3. The bullet strikes the C7 Transverse Process at the A1 position. It is not possible for the bullet to strike Interventebral Disc C06 C07 because it lies at a higher position than the trajectory of the bullet. The damage to C7 can be seen in X-AUT-8 at the A1b position. It appears that a chip has been removed from the edge of C7
This is a fact. X-AUT-8 point A1b supports this. In addition damage to Interventebral Disc C06 C07 ( See A2) could only be accomplished had C7 be struck hard by an object and the vibrations of that strike impacted on Interventebral Disc C06 C07 thus damaging it.
The essential elements in the change in my position are described in what follows:-
4. The bullets impact with C7 does the following
a) It diverts the bullets trajectory and allows it to pass over the lung and damage it.
This is a logical assumption. This is because we know from testimony that the lung was damaged. It is logical to assume that having struck C7 this could well have an impact on the bullet’s trajectory. Any bullet striking a solid surface, like a bone, invariably changes its direction. And because the lung’s Apex was damaged the assumption is that the bullet changes direction towards the Apex of the lung.
It causes significant damage to the Interventebral Disc C06 C07, damage that is very visible in X-AUT-8 at A2This is a fact. X-AUT-8 demonstrates this at point A2.
There is also a logical assumption built in here. A strike that hard on C7 that causes such damage to Interventebral Disc C06 C07 is bound to have had an impact on Interventebral Disc C07 T01. ( See point A5 ) Although it does not show the kind of damage that Interventebral Disc C06 C07 does, it must have been damaged and weakened by this same strike.
c) That damage to Interventebral Disc C06 C07, most likely had an impact on the Tectorial Membrane that lies behind these muscles ( See Point A3 ). This membrane links all the Interventebral Discs. It is likely that this damage/weakness to this muscle continued down to the C7 level.
This is a bridge between an Assumption and a logical assumption. All these muscles are interconnected and it would seem unlikely that the kind of damage that Interventebral Disc C06 C07 suffered would not also impact on the Tectorial Membrane. That said there is no evidence to support this.
d) What now happens is now is that the neck ( from C6 and above ) moves and slopes to the right a bit, because the damaged muscle Interventebral Disc C06 C07 as well as the likely damage to the Tectorial Membrane, are now not able to sustain the weight above them etc.
This is a Fact. X-AUT-9 demonstrates that as indicated by point A4. The upper neck has clearly shifted and sloped to the right and also moved downwards.
d) That movement may well have damaged Interventebral Disc C07 T01 ( See point A5 ) thereby allowing C7 to slip down onto T1 and to damage it.
This is a bridge between logical assertion and assertion. It seems logical that when the neck from Interventebral Disc C06 C07 ( Point A2 ) moves it is logical to assume that it impacted with Interventebral Disc C07 T01 ( Point A5 ) and that continued a movement down onto T1 and thereby damaged it on the right T1 Transverse process.
And so my revised position is this:-
a) The damage that we see on X-AUT-8 is not to C7 but infact to the muscle above it the Interventebral Disc C06 C07
As a consequence of the damage to this area, JFK’s whole neck slopes slightly to the right and slips down a bit.c) It is now possible that T1 could well have been damaged, not by a bullet striking it, but as a consequence of the neck slipping down because of the damage to Interventebral Disc C06 C07 as well as damage/weakening of Tectorial Membrane which combined have an effect on Interventebral Disc C07 T01. It is this damage, the Interventebral Disc C07 T01, that allows C7 to fall onto T1.
Two thoughts:-
1. Although Jackie gives some assistance when JFK slopes down to his left, is it not possible that a further reason for this slope is because of the damage to his neck? He is needing to find support for his neck.
2. Everybody has thought, and that includes me, that when JFK’s arms rise to upper neck it is a response to the throat wound and his difficulty in breathing. It may still be partly about that. However I am now wondering is it also a response to what is going on in his neck. If the upper neck has sunk slightly because of the damage to Interventebral Disc C06 C07 that would be excruciatingly painful. It is bad enough to have damage to the bones in the neck, but to also have the bones in the neck move, that must be extraordinarily painful.
Addition:-
Although I tried very hard to make this posting very clear, I began thinking that the amount of detail I included may have made it very difficult to follow.
Therefore I have included a video today that hopefully will explain my position a little clearer.
http://s1187.photobucket.com/albums/z388/jamesg27/Movies/?action=view¤t=RevisedPosition.mp4
James.
-
Jim, my comments in Red
Pat:
There are so many problems with these photos that one could go on all night about them.
When the ARRB got McDonald, Stringer's student, to actually survey the extant photos, he was stunned. He could not believe how poorly shot and posed they were.
You are absolutely right about the quality of the photos. As I have mentioned in this thread I have tried to get the photos professionally restored. I am having great difficulty because all those I have approached have reported back on the very poor quality of the images. Specifically their being data "washed out" by the closeness of the camera to the subject along with the use of flash. It is apparently a common complaint when a camera using a flash is so close to the subject data is washed out. What also surprised me was how out of focus some of the images were.
Further,he could not buy the fact that there were no perspective shots. That is, he said, that whenever you were shooting an area of the body impacted by a bullet, you had to shoot a long shot, medium shot, and then a close up of it. In order for there no to be any question about where the bullet hole was on the body. Where are those shots in this series?
I agree about the scarcity of images. I would have thought there would have been more. I remember the "Nova" program when the Dallas doctors were taken to the Archives to see the images. An area that had been the focus of considerable discussion was the damage to the back of the head that had been reported to be have seen at Parkland. I can't the name of the doctor, it could have been Dr. Jones, anyway when this doctor came out from seeing the images he commented that there are images that show that when the hair of the scalp, that is seen being stretched over the head in one image, is lying behind the scalp you can see the damage in the back of had. No one seems know of such an image. From what I can see, there is no image that shows this. However the doctor was quite emphatic about such an image existing. I would not want to think that he came out from seeing these images and deliberately lied on camera about an image he knew did not exist. But from what I can see such an image does not exist.
Further, why did Humes not use the correct anatomical landmarks to place the shot? He gave us markings that meant you had to line up the bullet hole with a T square to find it. That is ridiculous. Why was this done?
This has been commented on numerous times in this thread. Humes, under pressure is distorting the truth in order to meet the needs of the SBT.
And then why do so many witnesses place it lower than where it appears in the photos? And when Finck asked for JFK's clothing that night, it was nowhere to be found.
In video and image where I have attempted to locate the back wound you will note I was able to draw a base line. That line is below T3. It is possible, I'm sure, from that model an image to place the back wound around T3. I placed it higher but I could envisage someone taking that model and drawing and placing it nearer to T3. I placed it higher because it is clear in a number of Elm Street images JFK's jacket had risen a little.
Finally, you do know that the pathologists did not see the photos until three years later right? And this was done specifically so they could counter the growing chorus of criticism begun by Epstein's book, which showed the bullet holes in the shirt and jacket. Both Boswell and Humes then lied their heads off about this location in the media.
It is true that Humes does distort the truth in places, but I would say that in the main what he says in his description on the condition of the body and in his autopsy report, e.g. the lump, to use that kind of word, on the top of the lung, I have shown is absolutely true. Humes is aware of where he has played fast and loose with the truth (brought about by pressure being placed on him ) which is why he repeatedly asks that the autopsy images are used to better define what he saw the night.
James
-
My comments in Red, Pat
James, in my videos and on my website I try to track down the lies of the autopsy doctors. Prior to the testimony of the doctors, WC General Counsel Lee Rankin noted in executive session that a "picture"--which I assume to be the face sheet--showed the back wound lower than the throat wound. He wondered how this could be if the shot came from above, and said he would seek the doctors' "help" on this. Soon thereafter, the doctors were then told to prepare the Rydberg drawings--which it seems clear were meant to demonstrate what they'd assumed had happened. It seems clear, however, that they (primarily Dr. Humes) were uncomfortable with this situation, as Humes repeatedly testified that the photos would be helpful.
This led Specter to request Humes be allowed to look at the photos and confirm the accuracy of the drawings. Rankin then ran this by Warren in exec session, and Warren agreed that this should be done. And that's where the trail ended.
I have not followed the trail in the Executive meetings. I had not been aware of this point. Thanks for pointing this out.
Until Warren's posthumous memoirs came out. There, Warren revealed that he looked at the photos by himself, and thought them too gruesome for anyone to see. Well, this is preposterous.
Humes had tore Kennedy's head apart, for crying out loud.
I don't understand what you mean here. Were the autopsy images, before the autopsy began, not gruesome enough? What is it that Humes had done in addition?
The photos were created for him. While it's possible Warren was a sentimental fool, without any concept of what he was doing, it seems far more likely that he knew full well after looking at the photos and comparing them to the Rydberg drawings that the back wound location was problematic. And he just didn't want to deal with it.
I agree. To allow the truth to come out in 1963/64 would have been dynamite. Heavens knows what would have happened to the country had Americans known the real truth.
Within a short time of this, moreover, on the day of the re-enactment, Arlen Specter got a look at the back wound photo. He also failed to reveal that they proved the Rydberg drawings in error. Now, it's possible he did this because he was ambitious and scared. But there's another possibility, suggested by him, strangely enough. In 2003, he said that the SS agent showing him the photo was Elmer Moore. He'd previously said it was Thomas Kelley. Well, if it was Moore, or even Moore with Kelley, the trail leads back to Warren. You see, while Moore investigated the assassination for the SS, his job was over by the time the WC began its own investigation. He was then assigned to stick to Warren and work as his bodyguard. So, if Moore showed Specter the photo, it would suggest that the photo came from Warren, with Warren's blessing. Which would in turn suggest that Warren was sending a message to Specter: "YES, WE KNOW IT DOESN'T ADD UP.. BUT WE JUST DON'T CARE."
I had not known that, but I agree. Your logic is impecable.
In any event, the critics latched onto the different back wound locations on the face sheet and Rydberg drawings. This led to a re-examination of the photos in 1966. Dr. Boswell then went public claiming the photos supported the accuracy of the Rydberg drawings. He was under a military order of silence at the time. The next year, after receiving "talking points" from the Justice Department telling him to say the autopsy photos support the accuracy of the Rydberg drawings, and not the face sheet, Dr. Humes repeated Boswell's lie, in a televised interview with Dan Rather.
So, to sum up. It seems clear to me that the doctors LIED about the back wound location, but not on the night of 11-22-63, and only after their arms were twisted by the WC and Justice Department.
Yes, I agree. Sibbert and O'Neil have made it clear that nothing got into their notes, and later their report, that was not said in the autopsy room.
I was aware of your videos, but I had not paid too much attention to them. I am going to address that lapse and study what you have to say.
James
-
As might be expected, I strongly agree with Cliff here. I don't understand the reluctance on the part of some CTers to understand the significance of the holes in JFK's clothing, which are corroborated perfectly by Boswell's original autopsy face sheet, the description on the death certificate by Burkley and the testimony of Sibert and O'Neill. The "bunched up" theory is, imho, just as ridiculous as the SBT. JFK was the most immaculately dressed politician of his generation. It's ludicrous to imagine that he would permit both his expensive tailored shirt and his expensive tailored jacket to ride up so extensively in public. And how did they both happen to bunch up in a completely equal way, so that the holes match perfectly?
There is no rational reason to dismiss such solid evidence that proves conspiracy, in and of itself. There are no x-rays or belatedly released photos here to muddy the issue. The rear entry location is far too low to permit the SBT to work, which destroys the lone assassin thesis all by itself. I see no evidence whatsoever to just accept the HSCA's higher entry mark. Moving that back entry wound up even slightly plays into the hands of those who continue to ignore all indications of conspiracy.
Pat, my comments are in Red.
The significance of the clothing evidence, Don, is that it proves the Rydberg drawings inaccurate, and the trajectory pushed by LNs for the SBT to be in error. Cliff and I AGREE on this point. He, however, chooses to believe that it also proves the autopsy photos fake, and this despite the fact NOT ONE of the witnesses he cites in support for his proposed "lower" back wound has ever said they thought the back wound photo was a fake, and that several, in fact, have claimed it as authentic.
As far as the HSCA "higher" entry...what you seem unwilling to process is that the HSCA's drawing of the back wound photo is the single most important piece of medical evidence released by the government. It proved the Rydberg drawings inaccurate. It proved the autopsy doctors to be liars when they said the autopsy photos confirmed the Rydberg drawings.
I absolutely agree, when creating the Rydberg drawing he knew perfectly well they were lies. After all he had autopsied the body and he knew exactly where everything was. However, in his defense, I will point out that on a number of occasions he suggested that the autopsy images were much more accurate than what he had to say or had drawn for the Commission. I believe, although he had agreed to thoroughly distort the evidence, he was very unhappy with having done so.
It proved Arlen Specter dishonest, as he'd introduced testimony saying the SBT trajectory approximated the back wound location in the Rydberg drawings after viewing this photo, which showed the Rydberg drawings to be grossly in error.
To suggest Specter was dishonest, is being very kind.
Let's go back. The T-1 location proposed by the HSCA FPP is equidistant between the shoulder tip and mastoid process, exactly where it is shown on the face sheet, and exactly where the measurements on the face sheet place it.
I agree Pat. I had not noticed this before. When you first raised it I went back to the Facesheet and measured it. Both these points were equidistant to within 1 pixel. All Cliff has to do is measure it for himself to see that what you say is true.
This location, moreover, was, according to the HSCA FPP, TOO LOW to support the single-bullet theory, UNLESS...Kennedy rapidly leaned forward while behind the sign.
However, even had JFK leaned forward to provide the trajectory for the throat and Connally wounds, this location would still invalidate the SBT. That is because that wound in below Costa IR, which means the only path the bullet would have had in order to find a route to the neck would be to create a path through the lung, which in itself would invalidate the SBT.
Since Blakey et al understood this as their disputing that the bullet could have struck as early as 190, moreover, he hid this by having a trajectory expert MOVE the wound for the trajectory analysis, which, of course. showed everything in alignment.
So, in effect, the back wound drawing shows Blakey and Canning to be liars as well.
So WHY is it again, that we're supposed to go around pretending the single-best piece of evidence we have is fake?
I agree. Cliff constantly harps on about this image being faked. I am beginning to wonder if it is only fake for him because it is so inconvenient to his argument.
To debunk the SBT? The back wound photo does that all by itself.
I mean, if there was a photo of Bush taking a kickback from Enron, whose authenticity had been confirmed by a panel of experts, and which no one involved said was a fake, why oh why should we dispute it, when it PROVES something we've long suspected, and which the government has sought to deny?
P.S. I'm still waiting, Cliff, for you to show us where a wound at T-1 would be marked on the face sheet.
-
As might be expected, I strongly agree with Cliff here. I don't understand the reluctance on the part of some CTers to understand the significance of the holes in JFK's clothing, which are corroborated perfectly by Boswell's original autopsy face sheet, the description on the death certificate by Burkley and the testimony of Sibert and O'Neill. The "bunched up" theory is, imho, just as ridiculous as the SBT. JFK was the most immaculately dressed politician of his generation. It's ludicrous to imagine that he would permit both his expensive tailored shirt and his expensive tailored jacket to ride up so extensively in public. And how did they both happen to bunch up in a completely equal way, so that the holes match perfectly?
Don, I have on occasions commented that the jacket did ride up a bit. There are a number of images from Elm street that make that plain. How much it had risen I am not certain about except to say that It was certainly not anywhere near enough to place the jacket damage up by T1
There is no rational reason to dismiss such solid evidence that proves conspiracy, in and of itself. There are no x-rays or belatedly released photos here to muddy the issue. The rear entry location is far too low to permit the SBT to work, which destroys the lone assassin thesis all by itself. I see no evidence whatsoever to just accept the HSCA's higher entry mark. Moving that back entry wound up even slightly plays into the hands of those who continue to ignore all indications of conspiracy.
The placing of the wound is a different matter. In the image below I have given logical reasons why I have placed the wound where I did.
See image below.
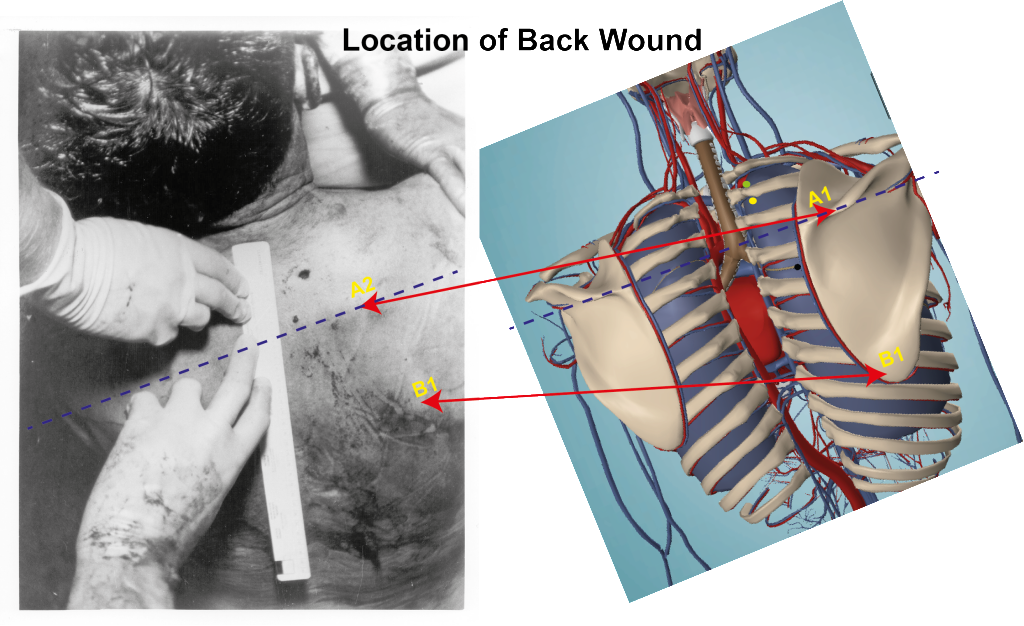
I believe, though you can correct me if you feel I am wrong, I have located the location of the Scapula Spline on the back of JFK's body. I have labeled that A2. I have drawn a line across the body in order to create a base line. I acknowledge the line of the JFK body is not quite straight, however the A2 point is fine. It is now a matter of judging where the wound is placed, with respect to that line. The first Vertebra above that line, on the model, is T3. It is now a debatable issue whether the Yellow dot should be closer to the T3 vertebrae or around where I placed it just below T2. It is a matter of where, in relation to the dotted line, you consider the wound should be. I placed it up towards the T2 vertebrae, I take it you would prefer it towards the T3 vertebrae. The green dot reflects those who feel it was beyond T2 and between T2 and T1.
I believe my placing of the line is correct, but I acknowledge it is a matter of opinion and judgement as to where you feel the wound should be placed in relation to that line.
James.
-
Here is the link to the video on damaging C7:-
Here is the link to identifying the location of the back wound:-

James.
James, your assumptions haven't changed. You insist that the lung must be damaged, while there is no credible evidence of damage to the lung.
Yes, my assumptions have not changed. They cannot change because they are the criteria for the SBT.
And what establishes that criteria as historical fact? That an assertion is convenient to a pet theory hardly seems like a logical measure of validity. Is your argument self-validating? JFK's back wound was at T1 because the pet theories of Pat Speer and James Gordon depend on it?
I don't think things work that way...
The purpose of that video was to establish how a shot from the front could do exactly what the supporters of the Warren Commission state the SBT did. In showing that a shot from the front can do exactly what the SBT can do was another attempt to undermine the SBT. I cannot change any of the assumptions/criteria, because they are the criteria of the Commission.
But by what leap of logic do you conclude that the criteria/assumptions of the Commission were based in fact? Because your pet theory requires it?
If I did so, e.g left one out, the supporters of the Commission would immediately accuse me of changing the criteria.
So what? I mean, I doubt if they will pay much attention to you, and if it comes down to it they'll find something else to throw at you. They are well versed in just making stuff up.
That is why those criteria have not, and cannot, change. Otherwise any attempt to demonstrate that a bullet from the front can do exactly the same as the SBT would be invalid.
[
The criteria of the Warren Commission is invalid, and neither you or Pat has made a fact-based argument otherwise.
With Pat it's all rhetoric.
The credibility of the evidence is Humes testimony and the Autopsy report.
That evidence has no credibility. Humes lied about the back wound location and Humes lied about the bullet transiting.
Earlier today I quoted David Lifton’s support for the authority of Humes observations and Autopsy report
Hold it. Lifton supports the observations Humes made during the autopsy, the observations you dismiss. The final autopsy report contains too many lies for Lifton to support, such as the "base of the neck wound" and the "transiting bullet."
and you said I can’t use that when referring to the back wound. Well, in this case, I am not referring to the back wound and I do now cite it.
The evidence for the damage of the lung is the Autopsy report.
You ignore the air-pocket overlaying the right C7 and T1 transverse processes.
When do you think this “air-pocket” was created that apparently overlay C7?
From the throat shot, as the obvious trajectory indicates.
Where, on earth, could such air come from I wonder?
It comes from an object tapping on the tissue.
The answer has to be the damaged lung.
No, it doesn't.
Now the bullet could never have come into contact with this air pocket.
It created the air-pocket when it came to rest at T1.
That is because the speed of the bullet meant that the bullet had long since finished its journey before that pocket was created.
That doesn't follow. A flechette lodging at that location would tap the tissue and create the air-pocket.
The air pocket did not just instantaneously appear.
Yes, it did. As soon as the round came to rest at T1 there was an air-pocket.
It had to take time, though I have no idea how much time it required to settle there. And certainly if it travelled as far as T1, which is some distance from C7 it would take quite a bit of time.
Okay, it took a period of time. Fine.
How could the air-pocket "overlay" the C7 transverse process if it struck underneath?
As I pointed out the air pocket was not created when C7 was damaged.
There is no evidence C7 was damaged. The x-ray shows T1.
It was created after the lung was damaged.
More self-validating assertions based on the words of a proven, serial xxxx.
The video describes the sequence of the bullet’s entry into the throat. The lung was last organ to be damaged. You cannot create a credible trajectory if the lung is damaged before C7 so it had to be the last organ to be damaged.
Garbage in, Garbage out...
Your reliance on the authenticity of Fox 5 is misplaced, given its poor quality and lack of a chain of possession.
I grant you the quality of Fox 5 is poor, but it is not so poor so as not to be able to identify features of the scapula. Being able to identify the edge of the spline allowed me to draw a base line. From there it was a matter of judging where above that line the bullet’s entry point was.
No, from there you have to identify the person who developed the photo and when they did it, and you have to find something in the photo which identifies the subject as JFK. Without a chain of possession those photos are worthless.
James.
Cliff,
I am sorry but I can see no point in continuing this conversation. There is no common ground between us. Everything I say you consider wrong and everything you say is right. There is no common ground between us through which we could have a reasoned conversation. You appear unable to acknowledge any aspect of my position and I see myself constantly arguing your position and defending my own position.
I believe the time has come to accept that we are diametrically opposed and will never agree.
james
-
Here is the link to the video on damaging C7:-
Here is the link to identifying the location of the back wound:-
James.
James, your assumptions haven't changed. You insist that the lung must be damaged, while there is no credible evidence of damage to the lung.
Yes, my assumptions have not changed. They cannot change because they are the criteria for the SBT. The purpose of that video was to establish how a shot from the front could do exactly what the supporters of the Warren Commission state the SBT did. In showing that a shot from the front can do exactly what the SBT can do was another attempt to undermine the SBT. I cannot change any of the assumptions/criteria, because they are the criteria of the Commission. If I did so, e.g left one out, the supporters of the Commission would immediately accuse me of changing the criteria. That is why those criteria have not, and cannot, change. Otherwise any attempt to demonstrate that a bullet from the front can do exactly the same as the SBT would be invalid.
The credibility of the evidence is Humes testimony and the Autopsy report. Earlier today I quoted David Lifton’s support for the authority of Humes observations and Autopsy report and you said I can’t use that when referring to the back wound. Well, in this case, I am not referring to the back wound and I do now cite it.
The evidence for the damage of the lung is the Autopsy report.
You ignore the air-pocket overlaying the right C7 and T1 transverse processes.
When do you think this “air-pocket” was created that apparently overlay C7? Where, on earth, could such air come from I wonder? The answer has to be the damaged lung. Now the bullet could never have come into contact with this air pocket. That is because the speed of the bullet meant that the bullet had long since finished its journey before that pocket was created. The air pocket did not just instantaneously appear. It had to take time, though I have no idea how much time it required to settle there. And certainly if it travelled as far as T1, which is some distance from C7 it would take quite a bit of time.
How could the air-pocket "overlay" the C7 transverse process if it struck underneath?
As I pointed out the air pocket was not created when C7 was damaged. It was created after the lung was damaged. The video describes the sequence of the bullet’s entry into the throat. The lung was last organ to be damaged. You cannot create a credible trajectory if the lung is damaged before C7 so it had to be the last organ to be damaged.
Your reliance on the authenticity of Fox 5 is misplaced, given its poor quality and lack of a chain of possession.
I grant you the quality of Fox 5 is poor, but it is not so poor so as not to be able to identify features of the scapula. Being able to identify the edge of the spline allowed me to draw a base line. From there it was a matter of judging where above that line the bullet’s entry point was.
James.
-
green it
Lifton doesn't agree with anything Humes said about the back wound. One of the things I appreciate about David Lifton is his steady regard of the T3 location as an historical fact. A base-of-the-neck wound would be massively convenient for his body mutilation theory, but David knows better.
I think its the head wound(s) where Lifton gives Humes a pass, not the back wound.
Cliff, can you give me your references for that for the idea that Lifton does not agree with anything Humes said about the back wound. Maybe I miss-read him.
Best Evidence, pg 155:
There was just too much evidence indicating the wound was "low."My responses in Blue:-
Yes, I see that. However I also note that on Page 501 of the hardback edition and P. 584 in paperback he also wrote "I trusted Humes and his ability to observe and report what he has seen" That is my position also.
Recently Pat made clear that the 14cm dimensions took you to T3.
No, that's not what Pat was aiming at. 14cm takes you to C7/T1, even though the properly filled out part of the face sheet shows a wound consistent with T3. Pat's trying to pull a fast one.
I don't agree. I checked his measurements and I found they worked perfectly. I posted that earlier in this thread. I checked his figures and they stood up. Pat's argument as to where that 14cm starts and ends takes you to T3.
I have said a number of times that my position in this thread is to work at dismantling the SBT from within the ground rules set by the WC. I know this is not your view, but if I can dismantle the SBT using their ground rules then they have nowhere to go. The criteria I am using to dismantle it are the very criteria they used to create it. That is why I accept, in the main what Humes says and why I accept the Autopsy Report.
This is the Pat Speer approach, as well. But neither of you are able to provide any intellectual justification for accepting the post-autopsy work product of proven liars. You think that buying into the fraudulent talking points of Lone Nuttery allows you the rhetorical upper hand against WC defenders, as if historical truth serves solely at the convenience of a public relations campaign? You guys accept the words of proven liars because it fits your pet theories, nothing more and nothing less.
I do not understand why you are so critical that I have decided to accept the Warren Commission position as a basis by which to attack them. I am not a Warren Commission supporter, far from it. I am using their own arguments and facts to destroy their findings. I do not see why that is so wrong.
You suggest that the anomaly was a "hematoma", well that won't wash. This distortion of the C7 transverse process is still seen in X-AUT-8.
According to the analysis for the HSCA it was the T1 transverse process which suffered the fracture.
You are quite right, that is indeed their view. You will have noticed that at the beginning of that posting I listed all four references to their view on T7 being injured.
However, they are wrong, if it is their view that it was injured internally in the throat. I have shown on numerous graphics that T1 is behind Costa IR. There is no way any missile could get to it, through the throat area, without first damaging Costa IR.
The physical position of the bones within the human body make it impossible for any bullet to damage T1 without first damaging Costa iR.
That's not what your A-B-C trajectory showed! There was a near perfect straight line from the nicked trachea to the T1 transverse process by way of the C7 transverse process on the same line of trajectory.
James, with all due respect, repeating your assertions over and over isn't the same as making a case for them.
That is not quite true Cliff. I believe my arguments, along with the supporting images, are what has made my case. I have shown numerous images that support the point that the T1 transverse process is behind as well as below Costa IR.
This excellent graphic shows an obvious path from the nicked trachea to T1 with just the right angle to leave an air pocket overlying the right C7 and T1 transverse processes -- and given the likely presence of hematoma on the x-ray, damaged blood vessels in that part of the neck are a given.
The are a number of problems with that graphic. First it does not include the arteries and veins that are in that area. Second the trajectory is far too high to be able to damage the lung. Third, the position of the body is not upright. It therefore gives the impression that T1 can indeed be damaged, should the bullet even be able to reach it and avoid damaging the veins and arteries. Fourth, in the video I posted yesterday on C7 I show exactly why T1 could not be damaged.
That is why it cannot be damaged. In addition, to be fair, if I am just repeating assertions then is that not also what you are doing?
Frankly, no. I'm making a fact-based argument as to why the Humes-Boswell work product is illegitimate, due to the lack of proper autopsy procedures, and the conflicts with the physical evidence, the properly prepared documents, and the consensus witness testimony.
You say the final autopsy report/Humes testimonies are acceptable because all of that fits in with your strategy of rhetorical combat with WC defenders. You offer no logical argument for why anyone else should accept it.
Now this is a little unfair of you. Is it your position that all the graphics I have created have no logical basis?
Is there not an element of truth that much of what you have said throughout this thread is assertion. Where is the evidence that Fox 5 is fake. And the operative word is "evidence." I note that on P. 505 of Best Evidence (Hardback Edition) Lifton wonders about the legitimacy of Fox 5. The problem he is not stating it is a fake, he is wondering whether that would answer the problems he was facing.
Even Lifton trusts that Humes has observed and written down what he has seen. That would suggest that the Autopsy report has some authority to it.
The video I posted yesterday on the locating the back wound gives real reasons why T3 may not be the location for the back wound. You talk about Humes not using correct body positions to measure from, well what is more stable than the Scapula to measure the position of the back wound. I have shown very clearly where on Fox 5 it can be seen we can therefore draw a base line from which to judge where the wound ended up. I have given my reasons that it was between T2 and T3.
I am a little surprised that you can suggest my work offers no "logical argument." Given the body of work I have produced here I feel that is unfair.
Humes was a proven xxxx, the autopsy photos are inadmissible in court.
I agree Humes lied with respect to CE 385. He knew very well that the position of the lung was wrong. You seem to be suggesting that everything he said was a lie.
Everything in the final autropsy report concerning the back wound is a lie. "14cm below the mastoid process" is not the same location as "just above the upper border of the scapula".
As I point out above, even David Lifton disagrees with this point.
I can't go along with that.
Well, the upper border of the scapula is clearly below the base of the neck, is it not? That's why Gerald Ford moved the back wound from that location in the WCR up to the back of the neck. Upper border of the scapula is too low. The final autopsy report was a pack of lies in regards to the back wound, pure and simple.
I suspect you have not looked at the video I posted yesterday. The model says differently.
Garbage in...Garbage out...
I am somewhat surprised that you consider everything I have been doing is "Garbage", that certainly is not my view.
Please do not mis-understand. Your models are wonderful! It's the data base and conclusions you draw from that data base which are garbage. The final autopsy report and James Humes testimony are rubbish, and cannot be intellectually defended.
Aside from CE 385 and the spurious decision to choose the 14cm measurement where is the "rubbish" in both his testimony and autopsy report. I have not found reasons to believe that he lied either in that document or in his testimony. I do not see what foundation you have to describe them as rubbish. Aside from the Rydberg drawings and the 14cm measurement for the back wound, could you point out one area where Humes has deliberately lied about what he saw and described?
James.
-
Malcolm,
Thanks very much. I am conscious this is an area of the study I have not paid a great deal of attention to. I am going to spend time studying this and see what way it contributes to my study.
I have ignored this area so far and I can see that was wrong.
Again thank you.
James.
 The Intervertebral Disc C06 C07, seen in X-AUT-8 would not be damaged to the extent it is by the bullet’s just passing by. The X-Ray shows it is very severely damaged.
The Intervertebral Disc C06 C07, seen in X-AUT-8 would not be damaged to the extent it is by the bullet’s just passing by. The X-Ray shows it is very severely damaged.
Dismantling the Single Bullet Theory Pt 5
in JFK Assassination Debate
Posted · Edited by James R Gordon
Was T1 Transverse Process damaged?
This is the first in a series of comments on issues that have arisen out of my posting on the SBT. In this one I examine the issue of the damage to the T1 Transverse Process. Throughout the thread the issue of T1 and whether it was or was not damaged was an issue that constantly arose.
In their work the HCSA stated that in their belief the T1 Transverse process had been damaged.
“The panel noted an interruption in the continuity of the right transverse process of the 1st thoracic vertebra much more clearly delineated in the computer-assisted enhancement of film No 8.” P. 98
They used as their authority the study by Dr. McDonnel whose full report can be found at P. 217 Addendum C
Read in isolation, there appears to be no dubiety about the issue: the T1 Transverse Process appears to have been clearly damage and of that there is no doubt.
However a close study of the report and their references demonstrates not only that this issue is nowhere near as clear as the HCSA would like us to believe, but ( in fact ) it is quite possible that T1 was never damaged.
At the heart of the issue were the X-rays and the interpretation of them.
Initially the Panel interviewed two eminent Professors from New York on the 27th February 1978.
a) Norman Chase Professor and Chairman of Radiology, New York School of Medicine.
Their comments can be seen on P. 99. Basically both were of the opinion that the T1 Transverse Process was undamaged.
Professor Chase is doubtful there is any damage to T1. This is because he says that if there was a fracture it was peculiar that there was no displacement of the bone. Basically he is saying that the bone shows no evidence that it has been damaged.
Professor Seaman goes further. He said the T1 Transverse Process appeared normal. In his opinion the T1 was undamaged.
Six months later, on August 4th 1978, the Panel approached Dr. G.M. McDonnel of the Department of Radiology of the Hospital of the Good Samaraitan.
Note:- I used the date of the report, as the date of contact. I acknowledge the contact was probably earlier but the HCSA don’t give a contact date.
From Dr. McDonnel’s submitted report the Panel were able to make the following statement. “The panel noted an interruption in the continuity of the right transverse process of the 1st thoracic vertebra much more clearly delineated in the computer-assisted enhancement of film No 8.” P. 99 His full report can be found on P. 217 Addendum C
However the above statement that the HSCA report made is not what Dr. McDonnel said. What he said was as follows:
“There is an undisplaced fracture of the proximal portion of the right transverse process of T1 (or the region of the costovertebral junction.)” P. 219 Addendum C.
Unlike Professor Chase who also saw no displacement and concluded that there was no damage, Dr. McDonnel also sees no displacement but does suggest there might be damage.
Grays Anatomy says this of Costovertebral Joints: “Together, the costovertebral joints and related ligaments allow the necks and the ribs to rotate around their longitudinal axes.”
It is clear that the “junction” Dr. McDonnel is referring to is the junction of the cervical vertebrae’s, in particular C7.
With the use of the brackets, it is clear that Dr McDonnel is not prepared to commit himself to stating that the T1 was damaged. In his opinion the damage could be elsewhere which is why he uses parenthesis to highlight this point. However that is not how the HCSA described his finding. There is no mention in the main body of the work that highlights that Dr. McDonnel was unsure of whether T1 was damaged and that he thought that the damage may well have been in the cervical spine. In their report the only point that is highlighted is Dr McDonnel's comment on T1. His doubts are removed from the report.
Nineteen days later, on August 23rd, the Panel contact their fourth expert: Dr. David O. Davis of The George Washington University Medical Center.
Unlike the previous three he is quite clear that T1 was indeed damaged. As the report states “David O. Davis M.D. professor and chairman of the Department of Radiology at the George Washington University Hospital and Medical School Washington D.C. also observed these same findings both on the original X-ray films and on the computer-assisted enhancement” P. 98/99 The “same findings” described are those of Dr. McDonnel. Dr. Davis’ full report can be found on P. 222 Addendum D
It is interesting that, as has been shown, Dr. McDonnel was not convinced that T1 was indeed damaged, but in the report not only is he portrayed as being convinced he is shown to be supported in this conclusion by Dr. David Davis.
Between February 1978 and late August 1978 the panel contacted four people to assess the X-rays and comment on them. Two of the experts were emphatic that T1 was undamaged. One was uncertain and only one, the last person contacted, was prepared to state that T1 was damaged. It is interesting, that in writing the report, David Davis is not the lead expert on the damage to T1. After all he is the only one who come out in favor of it being damaged. The lead expert, in the report, was Dr. McDonnel, who was not convinced that it was T1 that was damaged and thought it may be C7. David Davis was used to support Dr. McDonnel. See P. 98/99
John Hunt in an essay on JFK’s head wound says this about David Davis determination to show where the bullet’s exit point was “Why it “seem[ed] reasonable” to Davis “to assume that the exit point” was anywhere is left entirely to the imagination of the reader, for Davis never explained the rationale upon which he based his assumption. Davis’ unsupported and equivocal speculation not withstanding, the X-rays did not reveal any outshoot points. That left the FPP with only the photographs to make their determination.”
In the end, four experts examined these X-rays. Two decided that T1 was undamaged. One was ambivalent, and only one was prepared to state T1 was damaged. It is interesting that David Davis in his report on X-Rays says “there is evidence of a right T1 transverse process fracture.” P. 225 Addendum D. He can see clearly something nobody else saw, and the very feature, whose absence, determined Professor Chase to declare there was no damage to T1, makes me think that T1 was not damaged.
The process by which the HCSA went about contacting these experts leaves open the interpretation that they wanted someone to agree T1 was damaged, and therefore I suspect had David Davis not agreed the Panel would have contacted a fifth expert.
My conclusion from all this is that the T1 Transverse Process was not damaged.
James.