

James R Gordon
-
Posts
1,111 -
Joined
-
Last visited
Content Type
Profiles
Forums
Events
Store
Posts posted by James R Gordon
-
-
Greg,
I believe this image has been seen here before.
I seem to remember that it was taken from an upper floor window of a Hotel on Main Street.
James.
-
My comments in blue
I'm not arguing that the bullet didn't come darn close to the lung. Of course it came awfully close to it. The lung itself was bruised by the passage of the bullet. That's a fact. And another fact is this: That lung was not penetrated or damaged beyond just "bruising". And the pleura cavity was also bruised, but it was not struck or torn open by the bullet either.
Those are facts. Undeniable facts. (Unless you want to call the autopsy doctors liars.)
Yes we are in agreement here.
In my own opinion (which you are free to ignore if you wish), you, Mr. Gordon, are very likely attempting to micro-analyze the President's wounds (and their precise location in relation to the major organs of the body) in a fashion that probably cannot be done via standard schematics and charts and diagrams, etc.
I'm not saying that JFK's bodily organs and ribcage weren't located in the general locations where the standard anatomical charts place those organs and ribs, but I think we probably can agree that every human being is physically different in one way or another from other human beings.
The use of 3D anatomical software is of use in this kind of conversation. Unless the body of President Kennedy were to be exhumed [ a total impossibility ] we have no means to verify what has been said by Commander Humes et al. And even if we were allowed to exhume the body, only the skeleton structure would be left. And therefore a lot of the possible information that could be gathered is now lost to us. These models allow us to examine propositions in the way the body would have, had it been available to us.
You are absolutely right about every human bone structure having its own unique structures. These models create a generalized [ but highly accurate ] representation of the human body. There may be subtle difference with every human being, but those difference would not invalidate the findings of the model. Medical professionals use these models in teaching and learning.
So I disagree as to pertinence of using such models to converse on this topic.
One such example being: the precise location of JFK's mastoid process behind his right ear. When compared to another human being with a slightly different physique and build and neck length (etc.), if we were to measure 14cm. down from the tip of the mastoid process, we would likely get different results from person to person, with any "wound" located in the upper back being slightly lower or higher on the back depending upon that person's physical features.
Would you agree with me, James, on the above evaluation?
If it is your position, as I know it is, that the bullet transversed the upper chest area without piercing the lung and being able to exit through the throat, then there is only one area it could enter the body and that is above Costa IR.
See image below:-
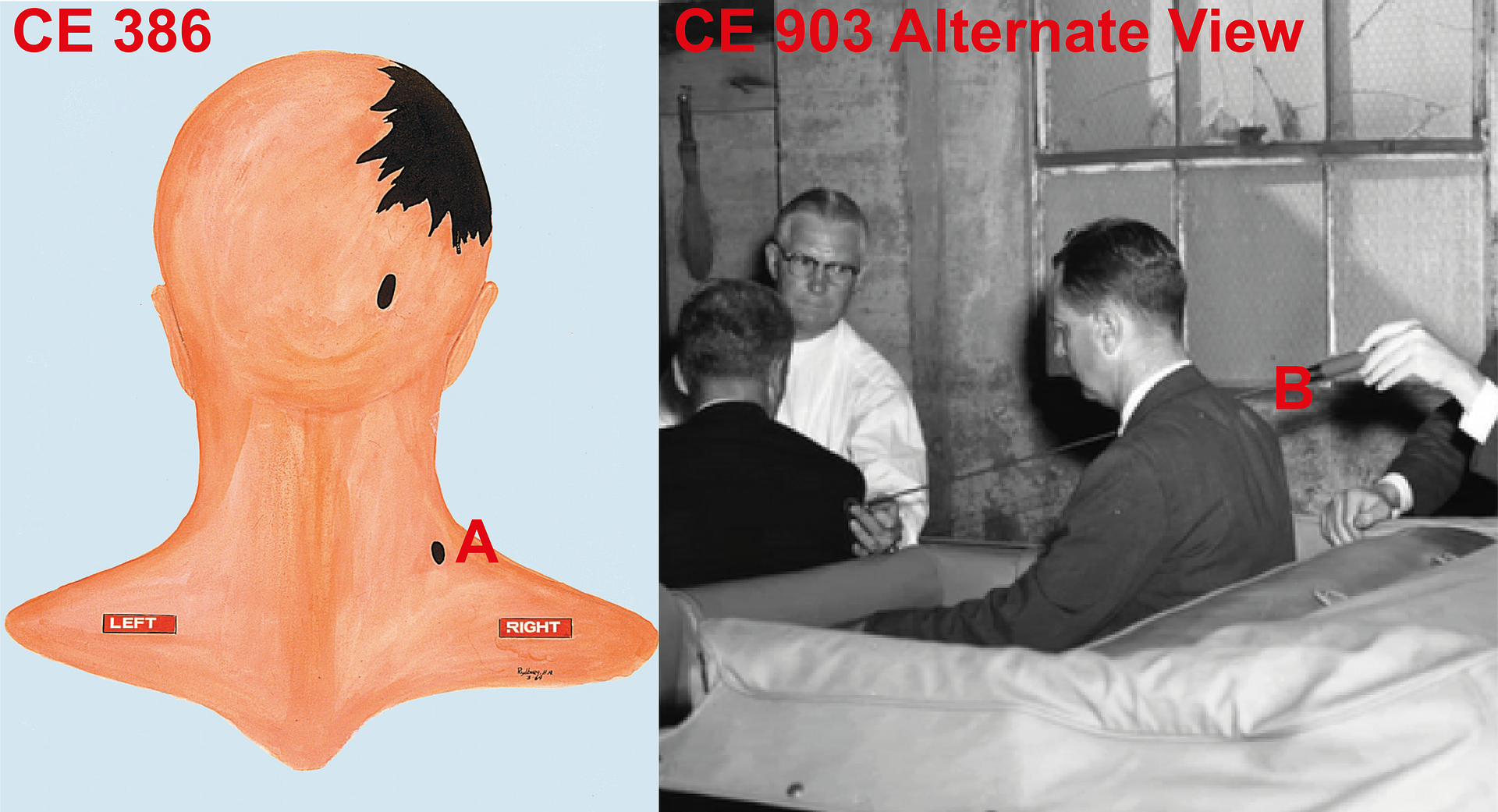
That is why Commander Humes place the entry wound above Costa IR. The entry point is probably still lower than the throat wound, but for the sake of argument lets say it is high enough.
However, as I understand it, CE 386 is not your position. Your position is CE 903. And that is where you have a problem. It is a gestimate, but I reckon than the entry point in CE 903 is just above T2 or just below it.
From that position any entry in that part of the body has to travel through the lung. There is no other route available.
While you maintain CE 903 is your position, it defies rational logic to maintain that a bullet entering at that point would not inflict grievous damage on the lung.
I think you get my drift by now, right? Each individual is unique in many ways. And attempting to make JFK's specific wound locations fit into the mold of a standard anatomical chart is, in my opinion, a potential mistake on the part of the person performing such an evaluation.
Now, yes, James, maybe JFK's body perfectly fits and matches every anatomy chart and diagram you'd care to post at this forum. Could be. I don't know for sure. But human beings being what they are--different from one another in a variety of very subtle ways--don't you think there might be room for some doubt about your conclusion that there was no way for a single bullet to have passed through President Kennedy's body in the manner suggested by the Single-Bullet Theory?
I accept that there may be subtle differences between the model and a particular human being. By that I mean, where I indicate T3 is might be actually slightly higher or lower in the body. But the inaccuracy would not be sufficient to argue that CE 903 could avoid damaging the lung. The inaccuracies are not as large as that.
And my last question is particularly relevant and logical since we know for a fact that the lung that you say would be hit by the SBT bullet was in fact bruised by the passage of that SBT bullet.
So we're really only talking about a very small difference in the measurements here. I.E., the small difference between a bullet actually hitting JFK's right lung vs. a bullet passing so close to that lung that it caused bruising of the lung.
Is that very small difference enough to make you totally discount the notion that the bullet didn't strike the right lung of John Kennedy, but merely passed very close to it?
My contention that any bullet had to strike the lung is based on your position in supporting CE 903. Again it is a gestimate, but the entry wound, at CE 903, must be around 3 inches lower than Costa IR.
In Summary:
Regardless of your charts and diagrams and supreme knowledge of anatomy, this FACT remains:
The bullet that went into JFK's upper back did not directly strike the lungs and did not strike any other bony structure within the body.
That is absolutely right. However your position in supporting CE 903 makes it certain that the bullet has to strike the lung as it moves towards the throat.
And this additional fact also remains (which is a very important fact that deserves to be pointed out at least once a day to the anti-SBT crowd on the Internet):
No bullets or large bullet fragments were found inside JFK's body.
So, James, since you think the SBT is bunk, please tell me what you think happened with regards to the bullet(s) that entered John F. Kennedy's upper torso on 11/22/63? How did one or more bullets manage to enter JFK's upper body, never exit, and yet cause no major damage (other than bruises) to the areas of the body that were violated by the bullet or bullets?
This is by far your strongest argument. I accept that with the absence of a bullet there is a clear logic that allows an argument to be made to support the SBT. And it is an argument I do not have an answer for.
The only way I am able to counter this argument is to point out the weakness in placing the entry wound at CE 903. As I have pointed out throughout this thread, CE 903 invalidates the SBT.
After all, even without a "Single-Bullet Theory" and even without a "CE399", President Kennedy was injured by at least one rifle bullet in the upper back and neck regions on November 22nd, 1963. And in my view, the SBT fits like a glove. Whereas, any non-SBT theory reeks with far more speculation and uncertainties (and, of course, vanishing bullets) than does the single-bullet scenario.
Well this is an area we will just have to disagree on.
James.
-
David Von Pein said:-
“Am I supposed to really just toss the SBT conclusions of both the WC and HSCA right in the garbage can because of your analysis? Really?”
Yes, I suppose the answer to that is “Yes”. But the operative word in that sentence is “analysis.” It is through analysis that I have come to understand that, on this issue, they are indeed wrong. Unlike you who agree with the WC and HCSA just because they say so, I have analysed whether what they have said stands up to scrutiny. And on this issue it does not stand up.
I returned to this debate with regard to the location of the back wound, and so I will restrict myself to that issue only.
See image below:-
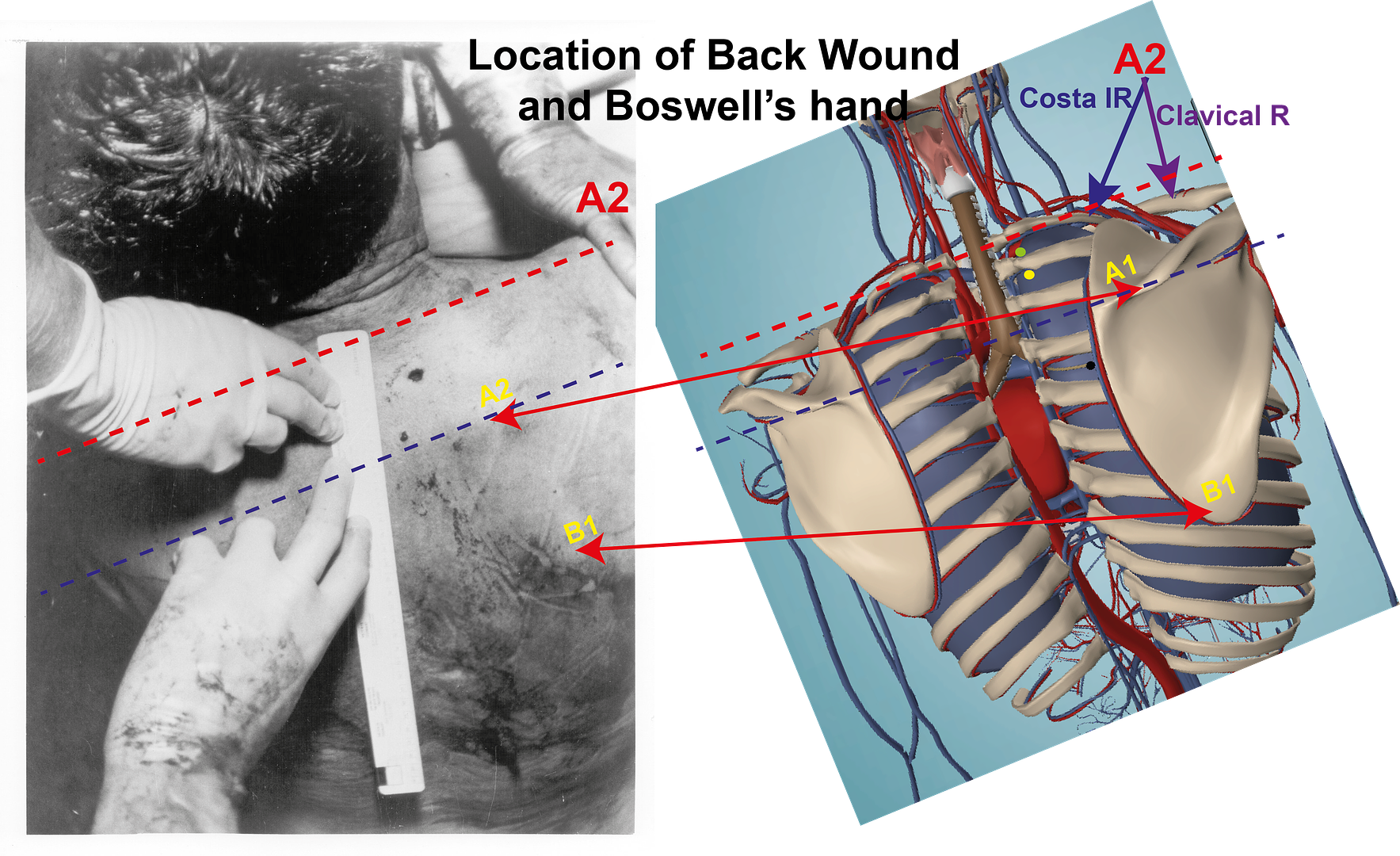
You are quite right the WC + HCSA and Cyril Wecht have pronounced on this issue. However there is another witness in this case: the body of JFK. Unless it has been tampered with, the body does not lie.
On the model there are two yellow labels: A1 + A2 point out the edge of the Scapular Spline. There seems no argument that we can clearly see the outline of the right Scapular on JFK’s body. There also seem to be no argument that the yellow A2 is the edge of the same Scapular spline identified as A1 on the model.
The blue dashed line is drawn to create a lower point of reference. It would appear to be just above T4.
The red A2 highlight's the position of Boswell’s hand. I assume it is his hand and it is Humes doing the measuring.
Although there is flesh and muscle above the bones, his hand is over Costa IR and Clavical R. I concede the positions of the arrow points are judgements, but they won’t be far out – if at all. The red dashed line has been drawn to indicate the position of this hand as well as an upper limit in the body.
Between these two lines is the wound. Even looking at the autopsy image on its own, it is clear the wound is very nearly lower than Boswell’s hand. It is at the level of the nail of the pinkie of Boswell’s right hand.
O.k. my analysis is not what the WC says or indeed what the HCSA say. Unless you are disputing the Autopsy image, please point out where this analysis is wrong.
It is clear to me that the wound is lower than Costa IR, I’ll leave it at that, and therefore the bullet is a clear danger to the lung.
James.
-
So that "changing body position" argument won't fly just because the Bethesda doctors decided to measure the back wound from an unusual location (the mastoid).
David,
I suppose I should not be surprised that from my post all you can comment about is this quote
'You are absolutely right, these terms have indeed caused confusion. Of course, it is not helped by Commander Humes 14cm reference which changes depending on body position."
You are quite interesting. That part was the least important element of what I had to say. The main focus was pointing out to you that we can identify skeleton outlines that allow a confident analysis of where the back wound most likely struck. I take it that all of that went right over your head.
James
-
The terms "neck", "base of the neck", "back", "upper back", "back of the neck", and "base of the back of the neck" have been used interchangably throughout the Warren Report and the witness testimony. This causes confusion when people read these varying terms.
David,
You are absolutely right, these terms have indeed caused confusion. Of course, it is not helped by Commander Humes 14cm reference which changes depending on body position.
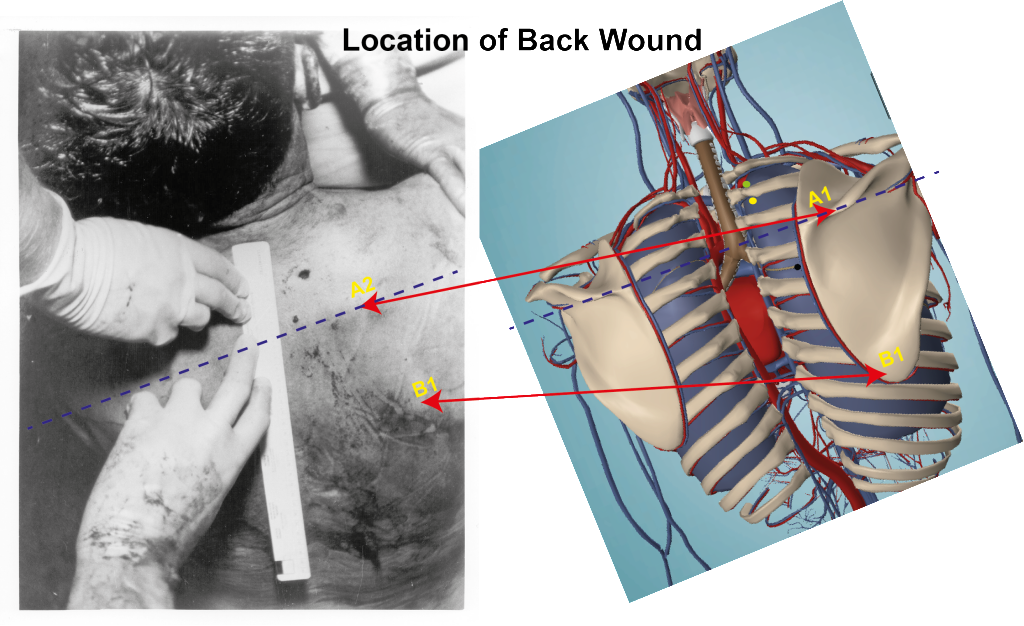
However, irrespective of the definition of these terms, there is within the contours of JFK's back examples of medical geographical points that are plain for all to see. In addition they are medical factual features that are outwith dispute.
You might want to debate your impression of where that wound in the back is, or is not. However the geography of the body can lead to a much more precise location. One identifying feature that is plainly evident on JFK's back [and beyond dispute] is the right hand Scapular. In addition, we can also see the Scapular spine and that again, is beyond dispute.
It is possible, therefore to be able to give a much more accurate assessment of where that wound is regardless of Commander Humes 14cm reference. The position of the Scapular on the human body as well as the position of the Spine, within the Scapular, are the same in all human bodies. As a consequence that allows us to have a much detailed assessment of where the wound is.
It would appear to me that the wound is where the yellow dot is on the model. Being generous, it could be as far up as the green dot on the model.
Commander Humes 14cm reference allows for a wide variety of interpretations, depending on body position. The Scapular and the Scapular Spine are much more precise locations. In addition both are clearly visible and are therefore outwith dispute. In addition, I take it that you can see that hand holding JFK's shoulder. The bone he is holding onto is the Clavical R.
That means the wound is lower than the Clavical R, but higher than the Scapular Spine. That places the wound most likely where the yellow dot is, and no higher than the green dot.
Either way your SBT is in serious problems. Be it the position of the yellow dot or the green dot the wound is behind the lung. Hence, if the SBT is a reality, the lung has got to be punctured.
This is the difference between generalised theorising and medical factuality.
James
-
Just because these bullets were not found, does not make the SBT right as a consequence.
But it sure as heck makes the SBT much more likely to be true (particularly when we factor in the common-sense observation of John Connally ALSO having been hit by a rifle bullet in his UPPER BACK at just about the exact same time that Kennedy was being hit by one).
Can you deny the logic of my last statement, James? If you do deny or sidestep its built-in garden-variety logic, then maybe Occam should pay you a visit and show you his Razor.
You may have read my post above, but it is clear you have not listened to what I said. Yes, one advantage of the SBT is that it does answer what happened to the bullet [provided you accept that CE 399 was that bullet, which I do not] but it does not answer the more serious questions both I and others have levelled about the theory. You clearly [although you have skilfully sidestepped the question] accept CE 903 as your position.

Although this is not CE 903 it is an opposite angle view of that picture. On your web site you make the following comment about it.
“this photo is just about spot-on perfect, in that the angle being depicted (if it is exactly the same 17-43-30 angle that we see depicted in CE903) would be TOO STEEP of an angle for any shot at precisely Z224. The angle in the photo below would, therefore, have to be lessened slightly to accommodate a shot going through both victims at exactly Z224.”
So aside from the trajectory angle adjustment, this is exactly the same as CE 903. That means with regard to the placing of the wound on the back, this is exactly the same as CE 903.
And there is your problem. If your stance regarding the position of the wound on JFK's back is CE 903, as you have stated on your web site it is, then by implication the SBT is impossible.
That position for the wound on JFK's back would require the bullet to pass through the lung in order to get to Trachea rings 3&4. It is anatomically impossible for any bullet entering the back as described by CE 903 to find any way to the Trachea except through the lung. That is an anatomical indisputable fact.
It is an illogical position to say that just because we could not find these bullets that has to mean that the SBT is the answer."
It doesn't have to mean it's the answer...but, as I just said above, the lack of ANY bullets (or even fragments of bullets) in JFK's upper body sure as heck makes it much more likely that one single bullet tore through JFK's body, leaving behind very little damage and leaving behind, of course, no bullets at all.
In fact, the #1 factor for Arlen Specter (as he has said in televised interviews) in arriving at a single-bullet conclusion was that same troublesome fact that CTers have no reasonable or logical answer for -- there were no bullets in Kennedy's body.
It stands to reason, therefore, that one single bullet passed cleanly through the President's upper back and neck, exiting his throat.
I concede there is a logic to this argument, but it falls and must fail if your position is as described by CE 903. CE 903 trajectory demands that the bullet has to pass through the lung and thereby damage it. For as long as your position is that of CE 903, your arguments for the SBT are meaningless.
And when you then factor in the Connally back wound, the math becomes even simpler. Connally was sitting in a direct line to accept any bullet that would have exited JFK's throat.
And here you jump to another point before dealing with the issue of CE 903.
It is an interesting factor that you appear oblivious to the point that the wounds to John Connally are irrelevant to the SBT if the wound to JFK do not adhere to its principles. Put simply, if the wounds to JFK do not adhere to the criteria of the the SBT, then the wounds of John Connally are of no importance. The wounds to John Connally are only important if the wounds to JFK meet the criteria of the SBT.
And so far they do not, because your position is CE 903 and because CE 903 demands that the lung has to be damaged the SBT fails at that point.
Given these variables, where can logic take a reasonable person? Should it take me to MULTIPLE DISAPPEARING BULLETS hitting Kennedy from opposite directions -- even though I know that CONNALLY too was struck in his UPPER BACK with a bullet at nearly the very same instant on Elm Street?
Or should logic take me in the direction where Dr. Cyril Wecht has travelled -- i.e., the bullet does go through Kennedy, but it totally misses Connally (and the limo). And Wecht purports such a theory even though he knows full well that the man sitting almost directly in front of John F. Kennedy also sustained a bullet wound to his upper back at an almost identical point in time in Dealey Plaza on 11/22/63.
I mean, come on. Let's be sensible. (That is allowed in a SBT debate, isn't it?)
Of course sense is appreciated in this discussion. However while you are in denial that CE 903 has to invalidate the SBT, sense appears to have left the conversation. In an earlier conversation I commented about the need for analysis. Why, do you think Humes had CE 386 created? Why would he place the back wound in that position in CE 386 and not as described in CE903? The answer is very simple: he needed the bullet's trajectory to miss damaging the lung. I have very serious questions about CE 386, as indeed I have about CE 385, but I understand why he had them drawn that way. Unlike you, at least Humes was being rational about the requirements of the SBT. Although there were questions that could be made about it, it had a major advantage over your position: Humes position ensured that the wounds to JFK met the criteria for the SBT. Your position does not meet those criteria.
The SBT can only become a legitimate solution when you can answer the number of criticisms laid against it. So far I have not seen you do that.But I have far more criticisms of any "anti-SBT" theory that might be used to substitute for the SBT.
Any anti-SBT theory must contain several aspects that are So Close, But Not Quite Close Enough to the SBT.
E.G.:
1.) The wounds on JFK's body in any anti-SBT theory are Close, but not close enough to where the wounds are really located in JFK's upper body (per the autopsy pictures and the Boswell Face Sheet measurements and in Commission Exhibit No. 903).
David, CE 903 is going to have a bullet pass through JFK's lung and collapse it. Now where is that in the SBT?
2.) John Connally is positioned Close, but not close enough to the position he needs to be in to make the SBT work. (CTers like Tony Marsh like to micro-analyze this aspect of their anti-SBT theory down to the exact number of inches, practically centimeters, that separated JFK & JBC, as if that figure can be established with 100% accuracy; it cannot be established with pinpoint precision, which is something I've always said since the first day I ever started talking about the JFK case on the Internet.)
As I have said above, the wounds to John Connally are irrelevant while the wounds to JFK do not meet the criteria of the SBT.
3.) The reactions we see exhibited by JFK and Connally in the Zapruder Film are Close, but not close enough to support the notion that both men were reacting to severe external stimulus at the very same time.
have you not noticed that JFK is already reacting to the wound in Z224, which is the frame you suggest he was wounded?
James
In the final analysis, it is my opinion that the Single-Bullet Theory is (to quote my favorite author, Vincent Bugliosi):
"So obvious that a child could author it." -- V. Bugliosi; Page 302 of "Reclaiming History" (Endnotes)
-
James, I have argued the merits of the SBT with David Von Pein on a number of forums, and the outcome is always the same. He always starts off claiming CTs are obviously wrong, because they dare disagree with "experts," but, by the end, he ends up admitting that, in order for him to believe the SBT, he has decided the last group of "experts" to look at the SBT, the HSCA's experts, were wrong on TWO key points: the moment Kennedy was hit and where he was hit.
You have to keep that in mind when you argue with him. He is not a WC defender, nor an HSCA defender. He only acts as though he is because it gives him someone big to hide behind. He is a theorist, pure and simple, much like the rest of us, only his theories all end up pointing to Oswald's sole guilt.
Here is a slide I created to prove to David the error of his ways. It shows that, in his analysis (and that of his fellow LNers, Tom Lowry and Jean Davidson) there's nothing wrong with claiming Kennedy's shoulder attaches Kennedy's neck above the level of his chin, as long as it helps them create the illusion the back wound was above the throat wound.

While I, too, appreciate much about David and his research, there is no middle ground with someone who won't even admit that Kennedy's shoulder attached his neck below the level of his chin.
Yes Pat, I see what you mean.
James
-
Follow-Up to my last post.....
I have what I think is a sensible and logical question for conspiracy theorists here who do not believe in the Single-Bullet Theory (which is almost everyone here, of course):
If the SBT is wrong (and particularly in the case of the theories which have JFK hit by TWO separate bullets to replace the one bullet of the SBT), then how can you account for those TWO bullets not hitting any bony structures or the lungs of President Kennedy, and yet STILL those two bullets inexplicably stopped inside JFK's back/neck?
Actually David the bullet not hitting any bony structures in the upper neck area is not so surprising. If you read my work on the SBT you’ll see why a bullet could miss bony structures. What is astonishing is that the bullet did not damage a major vein or artery. As I pointed out in the major post I made today, Perry’s comments about the quantity of blood he noticed in the upper chest area, ten minutes after the assassination, leads to believe that actually major vein(s) were damaged.
With regard to the back wound it was a shallow wound as described by Sibbert and O’Neill. So it is quite possible that, that bullet also did not strike a bone.
James,
You DO accept the autopsy report with respect to the lungs and the pleura cavity and all "bony structures" not being struck directly by any bullet that passed through JFK's upper body....do you not?
David, I put quite a bit of time writing todays post, did you not do me the courtesy of reading it. If you had you would have read my being quite plain that I accept the autopsy report and Humes testimony unless I can offer substantial reasons to doubt it. As I pointed out, Humes description of the SBT, as described in CE 385 is quite clearly a distortion of what happened. In addition I am beginning to doubt Humes statement that no arteries or veins were damaged in the upper chest area.
But at the moment, those are the only two exceptions.
Or do you really think that JFK's lung was hit by a bullet on Nov. 22nd? Did the autopsists lie about that?
You really did not read what I wrote. No, aside from the points above, I have no reasons to distrust the autopsists.
The reason I'm stressing this question again is to get back to this basic fact (whether you believe in the SBT or not):
The bullet (or bullets) that struck JFK in the upper back and neck areas did not produce any significant damage to the areas of the body that conspiracy theorists think would have had to sustain such damage if the SBT is true.
Now you are completely misunderstanding what I am saying. I am clearly on record stating that there will indeed be damage if the SBT were true. The only exception to that is if the entry wound is above Costa IR, as Humes has it in CE 386. Then the lung and bony structures may well not be damaged. Please note I am not saying anything about the rational for a continuing trajectory to John Connally. Also note that if your position for the entry point is, as Humes describes in CE 386, you still need to explain the wound in the upper back. Humes completely ignored that the wound in CE 386 is not the back wound.
If the Entry wound is, as described in CE 903, then there has to be damage and specifically to the lung. Any entry wound for the SBT below Costa IR has to, by definition, cause damage to the lung. There is no way it can be avoided, it is an anatomical necessity.
Which means, of course, that whatever bullets DID go into JFK's back and neck on 11/22 also did not produce any significant damage to Kennedy's lungs or ribs or other bony structures in his body.
Yes, I agree as of now. Later research might make me change my mind. But, as of now, I agree.
Which means that the anti-SBT conspiracists are left with this conundrum (not even factoring in the wounds to Governor Connally):
Two bullet wounds in JFK's body (back and throat)....no bullets in his body to account for either wound....and no significant "bony" or "lung" damage which could possibly account for the stoppage of the bullet(s) that entered the body of John Kennedy.
Fair point. But that does not affect the anatomical restrictions to the viability of the SBT. Just because these bullets were not found, does not make the SBT right as a consequence. The reasons why the SBT is an invalid theory still stand. That has not been changed by the fact these bullets were not found. It is an illogical position to say that just because we could not find these bullets that has to mean that the SBT is the answer.
The SBT can only become a legitimate solution when you can answer the number of criticisms laid against it. So far I have not seen you do that.
Don't conspiracy theorists ever give some serious thought to the "conundrum" I just stated above?
Wow!! is that not a piece of irony.
James.
-
David,
I am aware that you and I are on “opposite sides of the fence” regarding this case. And I may be on my own on this point, but I have a high respect for your understanding of the position of the Warren Commission. Your ability to cite a wide variety of opinions and views from the Commission is impressive. Your web site is an astonishing piece of work and a major resource to all researchers whatever their opinion of this case. Until I began this study of the SBT, in the spring, I knew nothing about the anatomy of the human body. I had no means to verify whether, what any medical person stated was true or not. It has been a difficult process and I openly admit I have made numerous errors, which fellow members have been kind enough to point out to me. But most important I am learning and I am beginning to be able to see what medical statements are likely to be valid and what cannot be valid. And that is solely down to analysis. I do not take anything anyone says at face value, I check to see whether it is possible and probable. And that something I do not see you doing. You appear to simply cite quotes and state whether they are or are not facts, without any analysis or refection.
As can be seen in your post, which I will reply to below, you simply quote one witness and state that is a fact and by the same token that I am wrong.
Let me go on record here. My position regarding Commander Humes testimony, drawings and autopsy report is that, unless I can establish reasons dispute, I consider them fact. That is not the view of everyone on this forum but it is my view.
And now I will address your post. I will place your quotes in italics. My comments will be in blue.
Point 1:-
The bullet which struck JFK in the upper back on 11/22/63 did not strike any bony structures or lungs inside the President's body. That is an ironclad fact that even one of "your own" -- Cyril Wecht -- agrees with 100%.
And the autopsy report and all three autopsy surgeons (who each signed-off on that autopsy report written by Dr. Humes) confirm the above fact as well.
And whether you believe ONE or TWO (or 22) bullets struck JFK in Dealey Plaza, the above fact will still be true -- no bony structures or lungs in JFK's back and neck regions were struck by any bullets.*
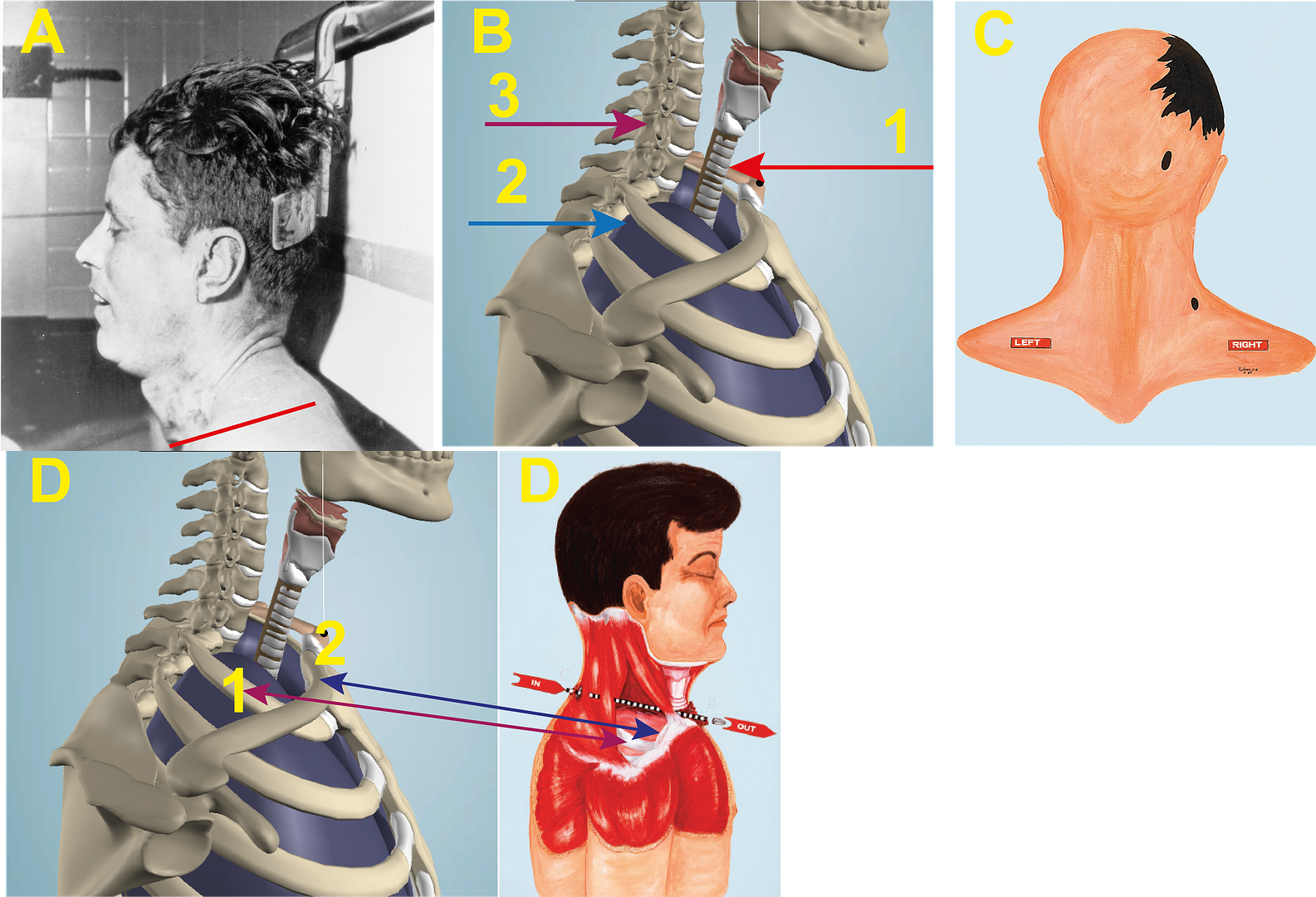
See Image 1 below:-
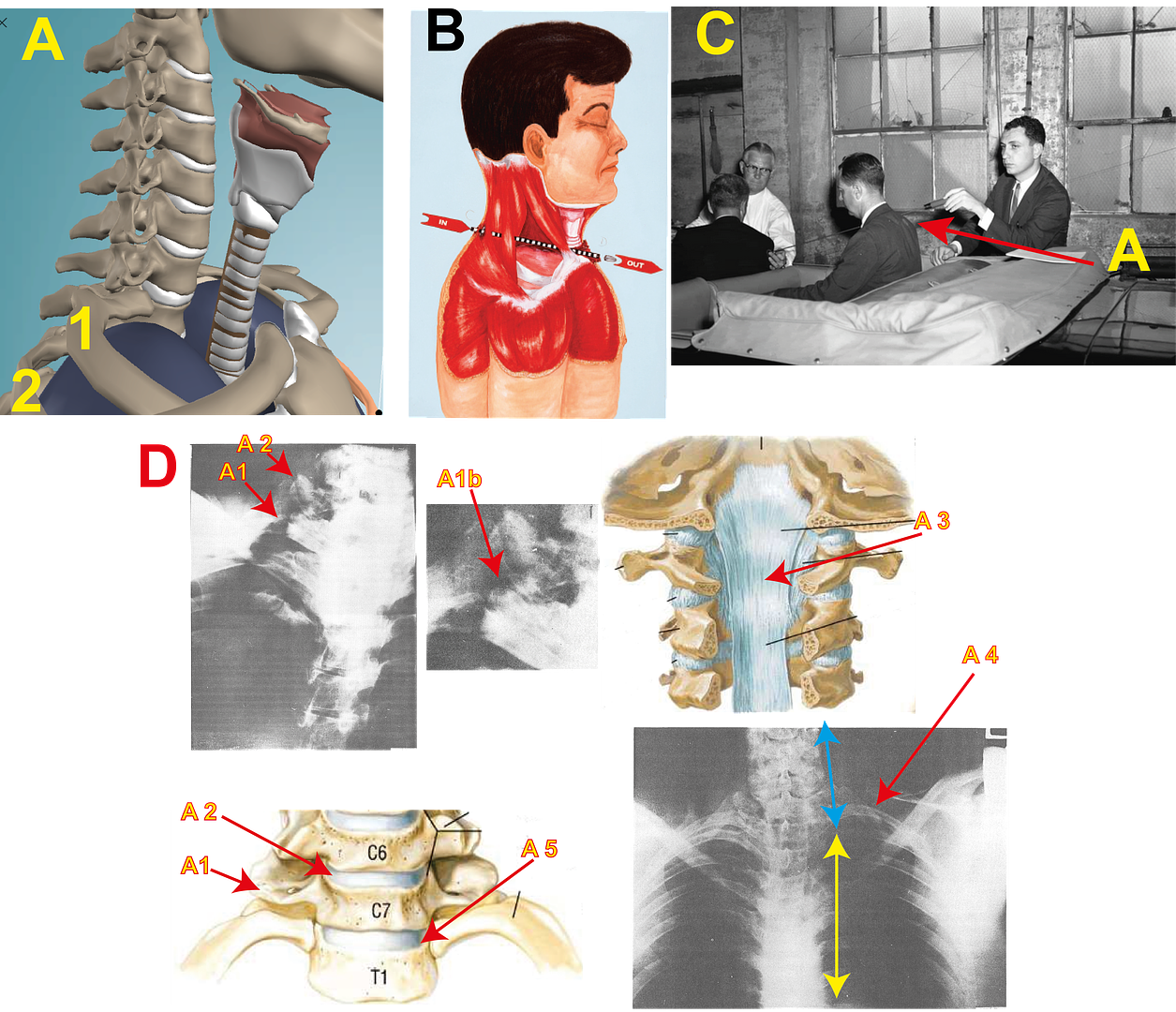
It is here that lack of analysis really lets you down. I do not dispute anything you say there. But by stating these points [ a) No bones were damaged;
 the lung was not damaged ] you restrict your options on where the bullet entry point can be.
the lung was not damaged ] you restrict your options on where the bullet entry point can be.See image A in the image below. If, as we agree, both the lung and bones were not damaged then the only entry point for that bullet would have to be above CostaIR, the bone that is labeled 1. Image B, CE385, the Humes drawing [even though Harold Rydberg drew it] has the bullet placed there. If you place the bullet at 2 [Costa IIR] you then place the bullet between T2 & T1. There are problems with such a position, as I have pointed out to you. One problem you have is that you support CE 903, and that is where it places the entry wound.
See Image C (which I copied from your website) I know it is not CE 903 but a variant but one where you can see the positioning of the bullet wound, which you can see in CE 903. Now, as I understand it you support that image as being a valid description of the bullet’s entry point. Well if you look at image A you can see that position has to be around T2.
The importance about this point is this. If it is your position that CE 903 correctly describes the bullet’s entry position then the only passage for that bullet to get to the throat is through the lung. There is no other option. It is an anatomical impossibility for it to do otherwise.
That is why Commander Humes drew the position of the entry wound in CE 385 + 386 above Costa IR. He knew what you have failed to recognize. He knew that placing it any lower would require the lung to be damaged. Hunt through all the Warren Commission documents and you will not find anywhere where Commander Humes states that CE 903 describes the bullet’s entry point.
Point 2:-
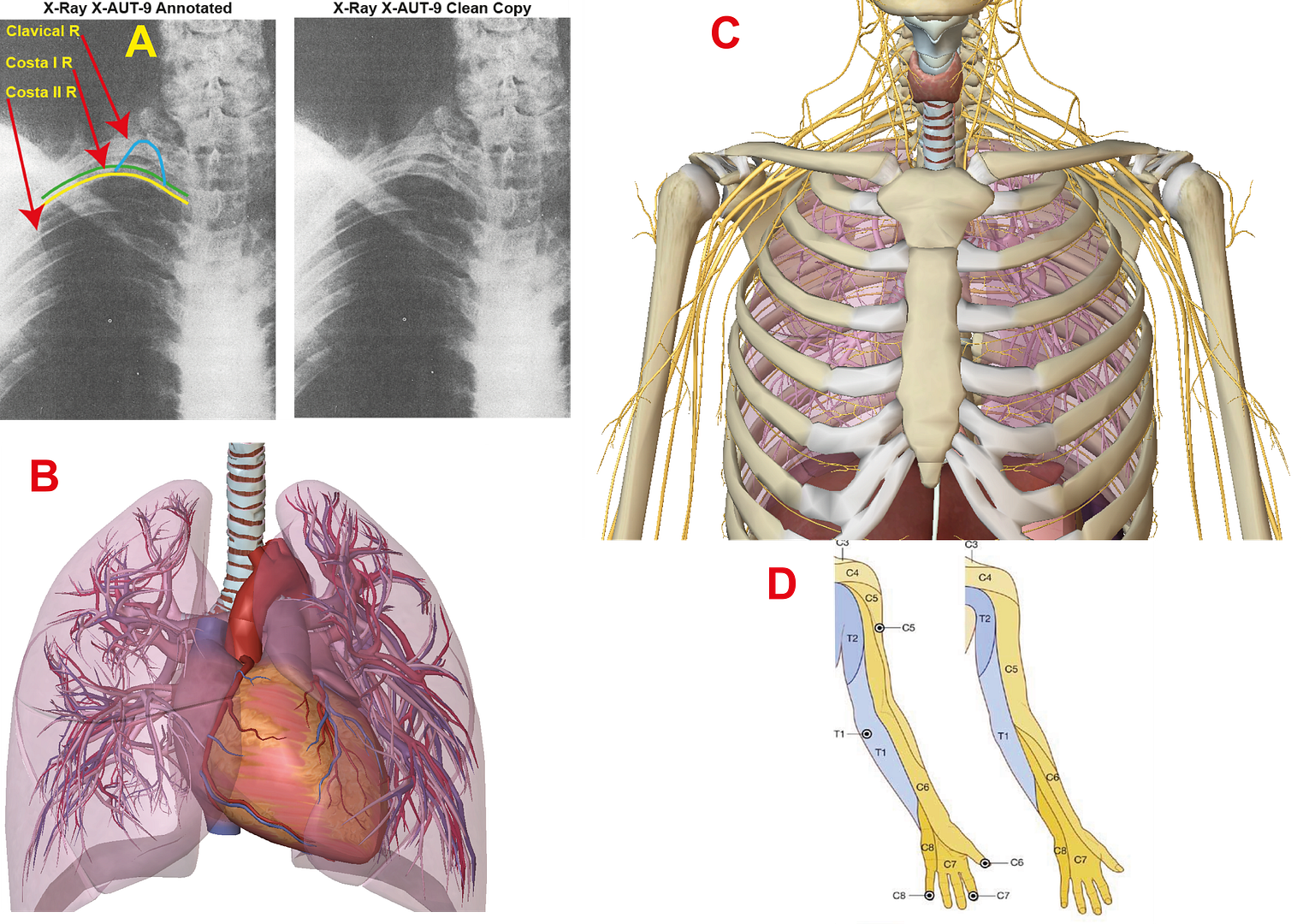
* = And the damaged trachea is obviously not considered a "bony structure". It's a cartilaginous structure. But, amazingly, even Dr. Wecht, in June 2007, insisted that "no cartilaginous structure" was even struck by the bullet that he does think went clean through JFK, exiting the throat. But--somehow--Wecht insists that that bullet missed Governor Connally. ... And the damaged vertebra wasn't actually struck by the bullet either. The HSCA concluded that the passage of the single bullet near the vertebra is what caused the damage to the vertebra.
I am not sure what vertebra you are talking about. If it is T1 there is serious doubt that it was damaged. Between February 27th and August 23rd 1978 the HCSA contacted four doctors. The first two decided that T1 was undamaged. The third was ambivalent, and only the fourth was prepared to state T1 was damaged. This fourth David Davis in his report on X-Rays says “there is evidence of a right T1 transverse process fracture.” P. 225 Addendum D. He can see clearly something nobody else saw, and the very feature, whose absence, determined Professor Chase, the first doctor to be contacted, to declare there was no damage to T1, makes me think that T1 was not damaged.
The process by which the HCSA went about contacting these experts leaves open the interpretation that they wanted someone to agree T1 was damaged, and therefore I suspect had David Davis not agreed the Panel would have contacted a fifth expert.
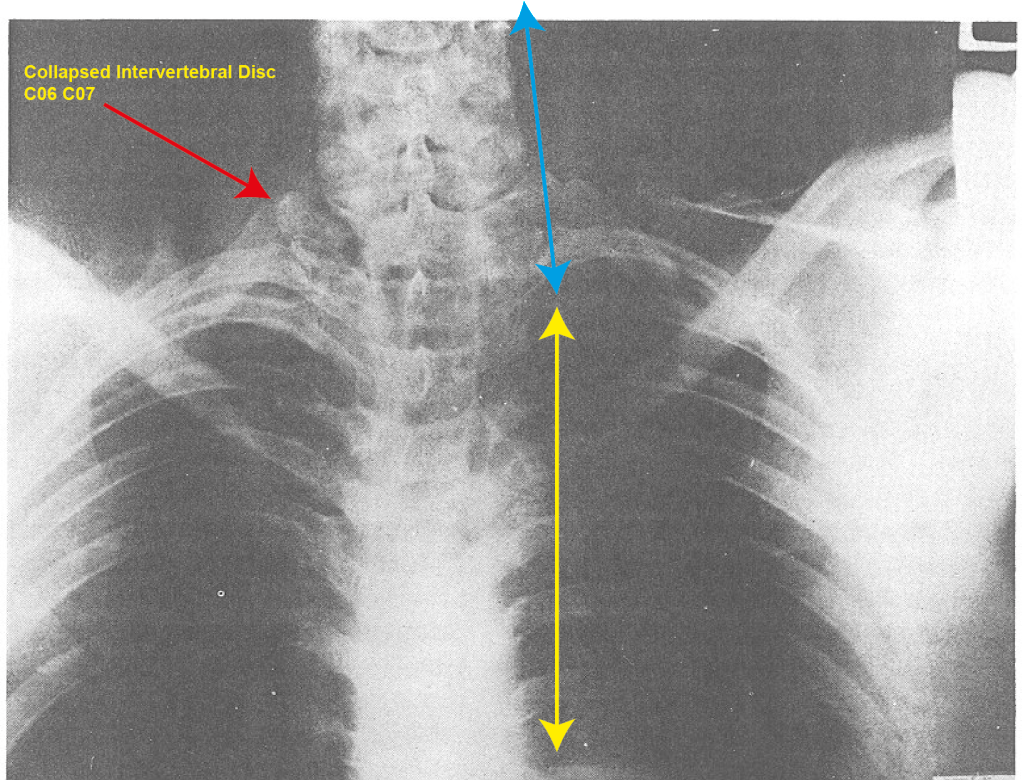
However if you are talking about C7, it was not damaged as far as I can see. However, the support muscle between C7 and C6 appears seriously damage according to X-rays 8 + 9. Indeed in 9 we can see that the neck has moved to the right.
See image D. In the first image A1 is C7. It does not appear damaged. A2 is the support muscle above. It is quite clear that something strange is happening there. Below X-Ray 8 is a drawing showing how these muscles and Cervical vertebras should be. On the bottom right hand side is X-Ray 9. This was taken before the autopsy had begun. It is clear that the neck has shifted to the right. You can also see the damage to C6/C7 muscle. The movement in the neck is exactly where the C6/C7 muscle was. The clear reason is that the C7/C6 muscle has been destroyed and can no longer support the neck and that is why the neck has fallen.
Point 3:-
We know where the bullet entered JFK's back (5.5 in. below the mastoid). We know where the bullet exited (as confirmed by autopsy photos). And this photo proves for all time (IMO) that the HSCA was wrong about the throat wound being anatomically higher than the back wound:
Again you are wrong. Using the mastoid as the reference the position changes according to body position. Lets make it easier. Is the entry wound, according to your understanding, as described by CE 385 or CE 903?
If you agree with CE 903, then the HCSA are indeed correct. The throat wound is indeed higher than the back wound. If you agree with CE 385, then you are right that the back wound is higher, or at least level, with the throat wound.
So which do you agree with?
See Image 2 below:-
With regard to your use of BE 1 [best Evidence 1, I don’t know its Fox number] I have used a better copy of the image to demonstrate. I have placed your line back in exactly. I understand what you are trying to do, but that line is meaningless. There is no way in a 2D image you can recreate a 3D position.
See image A. If you look at JFK you will see his head is bent backwards. JFK’s posture is such that there is no way anyone can judge where the Tracheotomy exactly is on the body. We need a body fully standing up to judge positions better. Now anatomical models vary slightly and everyone’s bone structure is unique: i.e. everyone’s bone structure have slight differences unique to them. However, in general terms, anatomical models accurately display the human body in general terms.
Label 1 points to trachea rings 3&4: the known point of entry.
Image C is CE 386. Looking at the dot, Humes appears to have placed the entry wound around C7 & C6. Being generous lets say the entry would is level with Trachea 3&4
Label 2 points to the point identified by CE 903, which is between T2 & T1.
Label 3 Points to C6, which is the only point that is higher than Trachea rings 3&4.
Now I grant you that anatomical models have slight variations and errors, but not sufficient to invalidate the general point I am making. The point being that when you identify the entry point [trachea rings 3 & 4] you have to be somewhere in the region of C6 to actually be above that point.
Tracing a line like you did (and I understand what you were trying to do) has to create an invalid reference to 3D positions.
So, what I am saying, with your use of BE 1: you have not proved your point at all.
Point 4:-
Therefore, given the above known facts about JFK's wounds and the lack of internal damage, where do conspiracy theorists think they can go with this information to support some murky and unproven theory about multiple gunmen and/or some type of "anti-SBT" theory?
Regardless of whether the SBT is true or not, the above facts I stated about JFK's wounds (and the lack of any substantial damage inside Kennedy's back and neck which could have possibly accounted for the stoppage of any bullet--let alone TWO separate bullets) will still be the facts.
So where do you anti-SBT guys want to go with these facts?
I believe, though you may not agree, that I have shown you that what you have described above as “facts” are indeed not facts. This not because I say so. It is because I have analyzed what was said and pointed out to you where the errors are.
Did Humes lie about pretty much everything?
From what I can see Humes only lied twice. When he created CE 385 he deliberately raised the position of the lung beyond where it should be.
See Image D.
Label 1 points to the position of Costa IR on the model as well as CE 385.
Label 2 points to the position of the Clavical R on the model as well as CE 385.
On the model the position of the lung is around level with Costa IR and below the Clavical. In CE 385 it is well above the Clavical R. I have it on good authority by a senior medical practitioner that had anyone’s lung been in that position in the upper chest area, it would have caused serious medical issues. It is actually encroaching on where the Jugular and the Carotid R arteries are.
Now I understand why he did it…..it was to explain how the bullet when passing through the upper chest area could damage the lung. But when creating this drawing he knew it was a lie. He knew exactly where the lung was positioned.
The second lie is that no arteries were damaged. Malcolm Perry’s testimony I listed earlier today suggests that arteries were indeed damaged.
Is the autopsy report a total fraud?
No.
Are the autopsy photos supposedly "fakes"?
I do not believe so.
Are the X-rays also frauds and forgeries?
I do not believe so.
Was the HSCA a complete sham regarding the SBT? Were the HSCA investigators and FPP members all liars too? Or were they just too stupid to know they were being "misled" about some things (as Pat Speer postulated)?
They were as selective with evidence as was the Warren Commission.
Spell out your theory that replaces the SBT. HOW did it happen? And where was that frontal shooter located that could have possibly accounted for the throat wound being an "entry" wound (as almost all Internet CTers believe)?
First the SBT is invalid. It never happened. What did happen I will show you next year when my model is up and running. And I will look at the SBT, I will show you then why it is an invalid theory.
It would be nice if a CTer could provide at least some solid evidence to back up a valid, workable, and (above all) reasonable "anti-SBT" theory. To date, I've never seen such a theory. And I doubt one will ever be forthcoming.
Have you not read my thread “Dismantling the Single Bullet Theory” Parts 1 – 5? In simple terms I have made two propositions.
1) I have demonstrated that the path of the SBT through JFK’s neck was not possible without seriously damaging the lung as well as arteries.
2) I have, particularly in part 5, suggested how the damage to the upper chest area could have been created by a bullet from the front.
Maybe you should look it over, though I suspect you already have.
And before you start, no I have no idea what happened to the bullet. But having no bullet to show, does not mean it cannot be demonstrated that the shot came from the front.
Most CTers will say, in return: Well, why can't you provide some solid evidence that the SBT is true?
That is not me!!
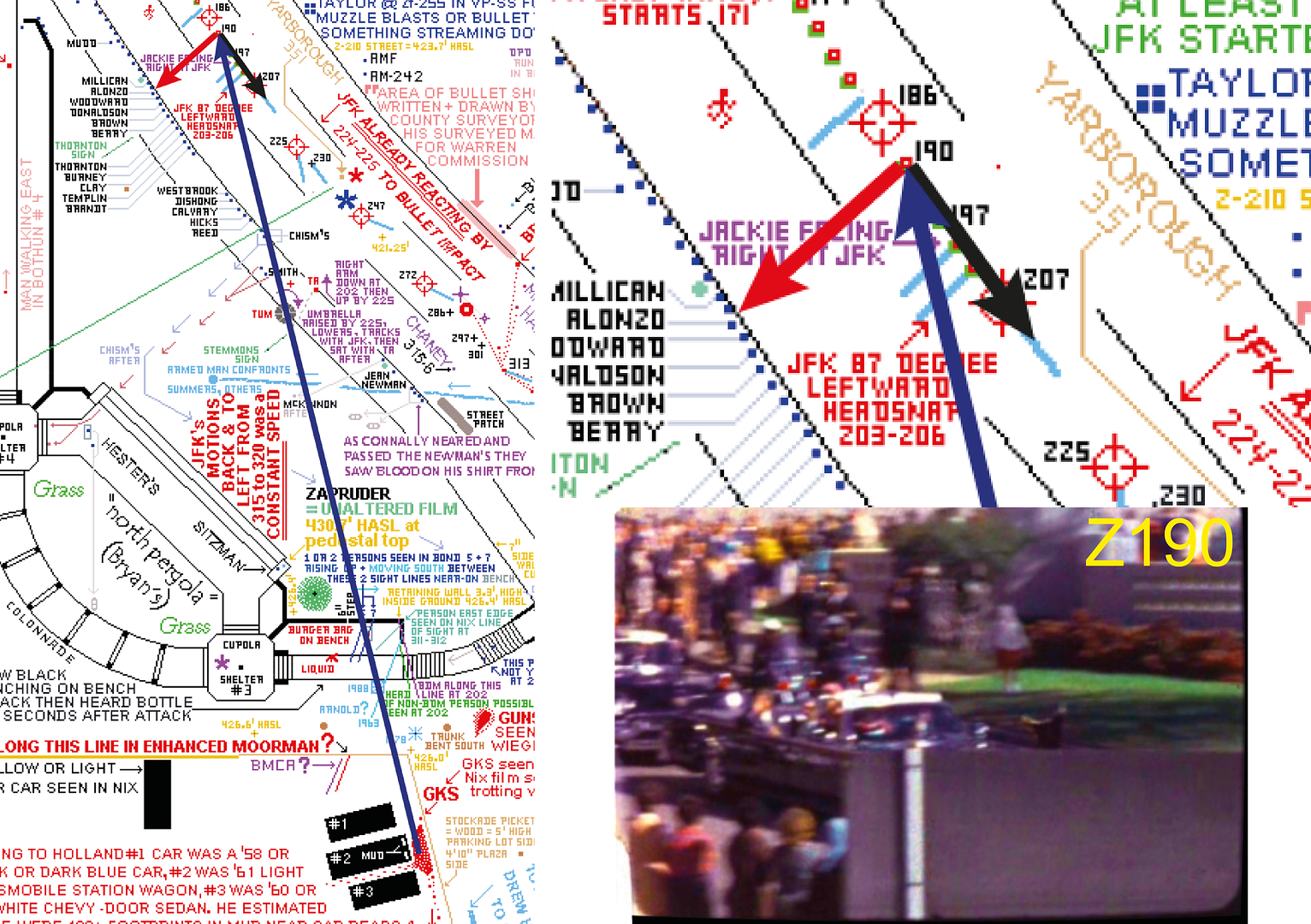
I, however, think that has been done. Many times over, in fact. Starting with the autopsy report, then the WC's re-creation in Dealey on 5/24/64, then Dr. Lattimer's tests which support the general workings of the SBT in the 1970s, then the HSCA's work in the late '70s (although, as mentioned, I do disagree with some points the HSCA & FPP made--like the silly Z190 SBT timeline and the "throat wound is higher" conclusion, but they utilized some common sense in concluding--in general--that ONE BULLET definitely did strike both Kennedy and Connally), and then the FAA simulation, and then Dale Myers' exacting computer work.
Point 5:-
All of the above things provide good, solid underpinnings for the validity of the Single-Bullet Theory. Are they ALL dead wrong? From the WC, to the HSCA, to Lattimer, to FAA, to Myers? If the CTers think they are all wrong, I beg to differ.
Your fault is not that you are not supremely acquainted with the data of the assassination. You are. My criticism is that you have not analyzed any of the information. Your position, appears to me, to be “Well if these bodies and people say “this” or “that” then they must be right. Commander Humes, when explaining the SBT, said “..the missile traversed the neck and slid between these muscles and other vital structures.” H2 P. 363 (my emphasis) Only when you examine the human anatomy of the human neck do you question such an incredible statement. If you look back at some of my work in “Dismantling the Single Bullet Theory” Pt 5 you will see images of the upper neck area with the vein system in place. It is close on to an impossibility for a high velocity bullet to pass through that region and do minimal damage. I always questioned how these arteries and veins were not damaged. It was not until I looked at Malcolm Perry’s comments the amount of blood that I realized they must have been damaged. Now I would not expect you to agree with me, but I had hoped for a higher level of argument than just the recitation of other peoples comments.
Addendum Re: Perry----
And the main reason I posted Dr. Malcolm Perry's "It could have been either" WC testimony was, quite obviously, to counter this wholly inaccurate statement made by James DiEugenio:
"And no one will ever impeach Dr. Perry on this."
Fact is, of course, that Dr. Perry himself pretty much impeached his initial 11/22/63 statement about the throat wound being one of entrance. And he did so by admitting to the Warren Commission that the throat wound could have been "either" an entry or an exit.
Though I do not agree, I understand your point.
James.
-
So how about it, Mr. Von Pein...bone up on your anatomy and physiology, and then explain why Mr. Gordon is wrong in his conclusions. I can hardly wait. [Odds are, Von Pein will instead attack me for suggesting this, and continue to ignore Mr. Gordon's quite logical arguments. But then, I'm a much easier--and most likely larger--target to attack.]
Mark,
That has been my opinion for some time. I had thought David would enter the "Dismantling the Single Bullet" thread. After all that thread is at the heart of David's beliefs on the SBT and I, and others including yourself, were attacking the credibility of the SBT very seriously. I am sure he read the thread, but he refused to enter it.
Like you I had noticed this same point in this thread. I believe one thing this absence does highlight is the weakness of Davis's understanding of the case. He knows the generalities and quotes from the report, but the details of the medical information he has little understanding about.
James.
-
Mr. SPECTER - Based on the appearance of the neck wound alone, could it have been either an entrance or an exit wound?
Dr. PERRY - It could have been either.
David,
If you must insist on being so pedantic please, at least recognise, that Perry does not simply support your position. He is ambiguous in his reply.
Dr. PERRY - It could have been either.
If you insist on taking Malcolm Perry literally then you are admitting that the throat wound could be either an entry wound or an exit wound.
The best you can get from this quote is that we are both right.
It certainly does not confirm your side and deny our side. Basically it is not the best quote you could use. Could you not get a better one???
James.
-
1. In fact, that Z film excerpt is so deceiving as to be useless. Because the HSCA , Speer, myself, Ray Marcus, and anyone with eyes knows that the first shot hit JFK before he went behind the sign. Even Duncan agreed with that when he saw the uncensored film, much to DVP's chagrin.
Jim
I used to believe this, but I don't now. Assuming the shooter was firing from the North Knoll, then the shot had to have been fired either after JFK went behind the Stemmons sign or as he was.
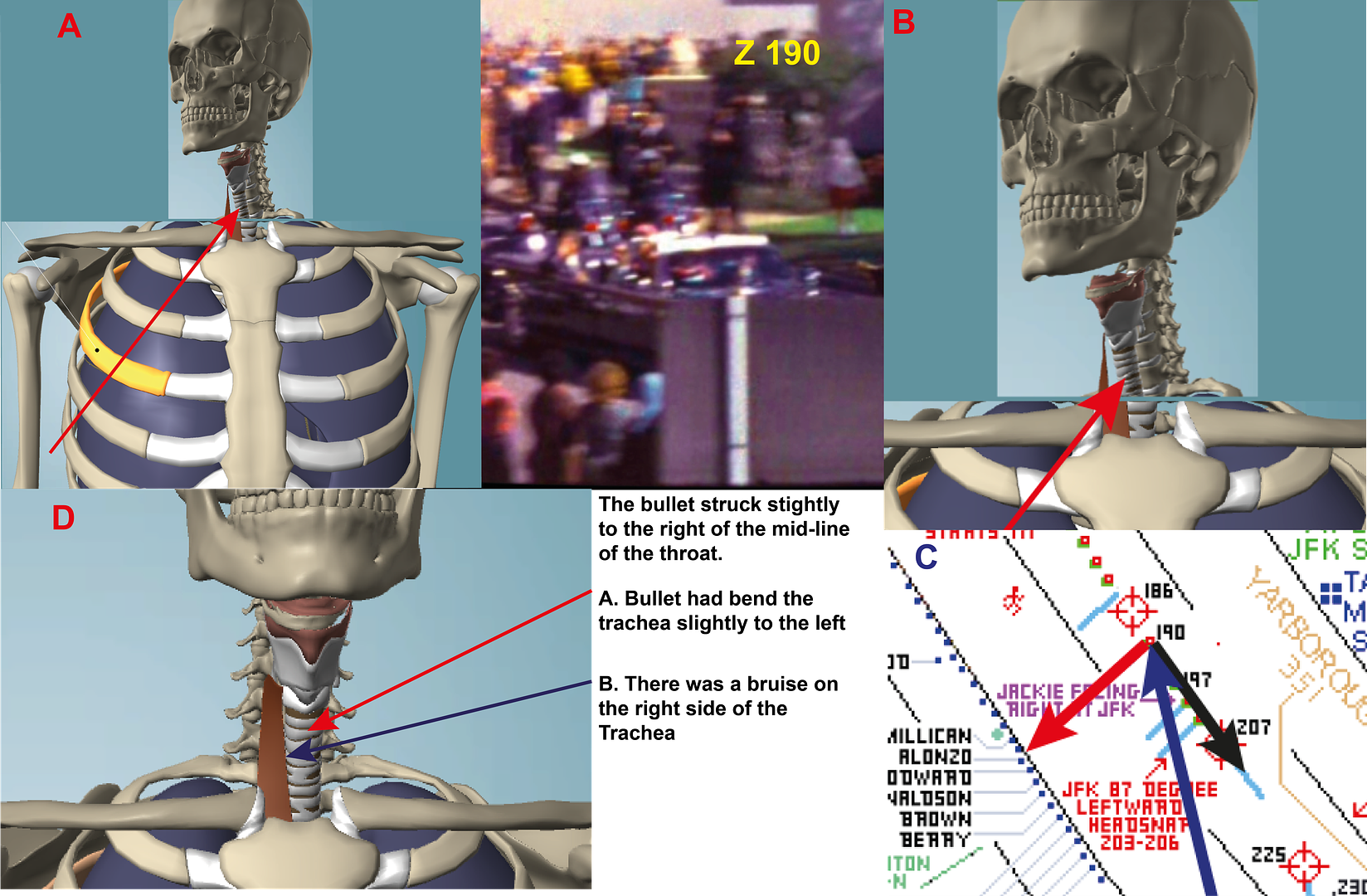
Dr. Carrico stated that the wound was right of centre. I have checked this with Fox 1 and indeed the lower half of the wound is indeed right of centre. Now from Z190 - Z 200 JFK is still turned to his right. Therefore although a gunman could strike the throat left of centre they would have great difficulty striking right of centre. It is not until Z 204 that JFK is fully facing forward allowing a shot to strike him in the throat right of centre. At that point he is either going behind the sign or just begun to travel behind the fence. For me the critical point in determining when that shot was fired is when is JFK facing forward and thereby allowing a gunman to strike him in the throat right of centre, and the only moment I can see when this can be done is from around Z 204 onwards.
And in fact, both Dr. Nichols and Mantik, even with these bad landmarks did the simple geometry. The cervical vertebra would have had to been fractured or broken. They were not. Nichols testified to this at the Shaw trial.
I hate to disagree with such experienced men, but something is wrong with C6-C7 vertebra muscle. AUT X-RAY 8 clearly shown an anomaly there. The shape of it suggests that it has been seriously damaged. AUT X-RAY 9 seems to confirm this in two ways.
a) It agrees that this some sort of anomaly at this point.
This X-RAY also shows that the neck is best at exactly this point. The neck can be clearly seen to have dropped at this point. Now the neck cannot drop its position at this point, unless the support [which this muscle is] has been damaged and there is nothing now to support it.See image of X-Ray 9
There is one error with my image. I say it is the disk. It is not, it is the support muscle above it: the C6-C7 muscle. This X-Ray makes it clear that the neck has moved to the right. Unlike X-Ray 8, which was taken after the autopsy had begun, This one was taken before the autopsy began. There is no reason, as far as I can see for the neck falling unless something has happened to this C6-C7 muscle.
And that is why, even though such highly respected men suggest there is nothing wrong here, I say something is wrong there.
James.
-
David,
Your question was just too tempting not to answer.
“If the SBT isn't correct, then tell us what the most reasonable explanation is to explain the wounds in both JFK & JBC, and the total lack of bullets in the body of President Kennedy?”
I’m sure Pat will answer you and his answer will be thorough.
First, I have no answer to what happened to the bullet. It is a serious question, and hopefully someone will be able to answer it at some point. But the throat wound, as an entry wound, to JFK I believe can be answered.
1.) Dr. Carrico stated that the entry wound was right of center. H6 P. 10
That can be confirmed by drawing a line from the center of JFK in the FOX 1 picture: “The Stare of Death.” That means the shot came from the Grassy Knoll. To strike right of center the shooter had to be to JFK’s right. Why the Grassy Knoll, because the trajectory of the bullet is declining, after entering the body, and hence the shot was taken from above his position. Why declining, because the lung is lower than trachea rings 3&4.
For the bullet to be able to enter right of center in JFK’s throat, he had to be seated facing forward. That places the shot from Z 202 onwards.
2.) Dr. Carrico stated that the trachea was deviated slightly to the left. H6 P. 10
He is saying the trachea was bent slightly to the left. Bending the trachea to its left means the shot impacted to the right of the trachea. Dr. Carrico further confirms that the shot entered right of JFK’s midline by saying that he noticed a small ragged laceration of the trachea on the anterior lateral right side. H3 P. 370
He is stating that as the bullet passed by the trachea, the trachea was also bruised.
3.) Commander Humes states that the right strap muscle was damaged. MD 3 P. 4
A further confirmation that the bullet entered the body right of center. Right of center of the trachea, is exactly where the right strap muscle is.
4.) Now in his testimony Malcolm Perry makes six references to the amount of blood he saw within the upper throat after he had cut the Tracheotomy. H3 P. 371, H3 P. 370, H3 P 381, H3 P. 388, H3 P. 832 and H6 P. 11.
What is striking about these comments is that Commander Humes stated that no major vessels and arteries were damaged. H2 P. 363 If you know anything about the anatomy of the upper chest area of the human body, that is an astonishing feat for any missile to achieve in that area of the body. The most interesting of Perry’s comments is the last one where he said “There was there was so much blood that the tissues were discolored.” Within 10 minutes of the assassination, which would be about the time Perry cut the trachea, there was so much blood in the upper chest area, not only could Perry not see details of organs and muscles ( in the other references ) the tissues of the body were discolored. There had to be substantial blood in that area to disclour tissues within 10 minutes. That suggests that as the bullet moved forward it did infact damage major veins and/or arteries. The route the bullet was taking, takes it right towards the major arteries and veins in the upper neck area.
5) Because of the bending of the Trachea and bruising of it, that makes clear that the bullet’s path will take it over the Apex of the lung. The Apex of the lung is very close to the position of the Trachea. Commander Humes describes the bruise H2 P. 367/8.
As Pat Speer has described to you this bruise was shaped as an inverted pyramid that was positioned on top of the Apex and was attached to the lung. Pat has suggested that bone could have caused that damage. I don’t like to disagree with Pat, but Humes is clear that no bones were damaged. H2 P. 361 + 364 I suspect the bruise might have been the pressures and forces created by the bullet that caused this damage.
6.) In his autopsy Commander Humes laid down certain criteria that this bullet had to undertake. It had to do the following:-
a) Damage the right strap muscle.
Damage the Trachea.c) Damage the lung.
The above account describes all three.
So you might then say, “but what about the bullet? Where was the bullet that did all this?” O.k. I do not know the answer to that, but because no bullet was found, does not mean that the injuries had to be caused by the SBT.
Dr’s Perry and Carrico as well as Fox 1 make it clear that the bullet entered, or exited in your case, right of center. That is as close to an established fact as we can get. Unless you intend to dispute Fox 1, the entry point is clearly right of center which does not help you.
The SBT requires the bullet to exit in the center of the neck. As Fox 1 shows the entry point is reasonable significantly right of center. Exiting right of center is going to throw out your trajectory both to the back wound as well as onwards to Connally. The SBT is based on the bullet exiting in the center of the throat.
So just because I can’t explain what happened to the bullet, does not mean the only answer is the SBT. And don’t forget, you have a far bigger problem than mine of no bullet. You support CE 903 as the definition of where the bullet entered. As I have pointed out any trajectory from there has got to pierce the lung. No bullet is able to say “hang on a minute, I’ll have to go left here…and I’d better go right here” If CE 903 is your position there is no way the lung would not be pierced. Just on its own that would invalidate the SBT.
As I said to you before. The injuries to John Connally are irrelevant if the injuries to JFK do not sustain the SBT. Only, if the injuries to JFK support the SBT can we then consider the injuries to Connally. And it is clear the injuries to JFK do not support the SBT.
James.
-
"Rankin hired a stand in to pose as the stenographer". Jim/Glenn, from an unashamedly self admitted amateur, would you tell me where this info came from? To think that they would do this to a U.S. Senator of Russell's stature is extremely sad. So, understanding that I am nit picking here, It's just that I would like to read further about this action. It seems that I do remember a promise of a statement required by Russel that there should be some parts of the findings (primarily, the single bullet theory), which was never done.
Terry,
You will certainly find the info on the change in findings in "Breach of Trust" by Gerald McKnight on P. 298 but I seem to remember others. Although I can't find a reference to it you might also find a reference to the stenographer also in the book.
James
-
David,
The problem with your series of six “facts”, is that they make no attempt to deal with the reality of the human body.
I accept point 1. “1.) The upper lobe of JFK's right lung was bruised by the passage of a bullet. That's a concrete fact. But the lung was not penetrated. Nor was the pleura cavity. It was only bruised by the passage of the missile as well.”
From the work I have been doing on this issue, the bruising was probably caused the pressures and force of the bullet passing near by.
However, although I quoted CE 385 in my previous post, CE 385 is a distorted document that hides the reality of the position of the lung in the body. The real position is as shown below. I have no intention of skewing this thread with all my points of view. If you want to see why I state CE 385 is a distorted document you will see my evidence the “Dismantling the Single Bullet Theory Pt5.”
What you see above is the actual position of the human lung in the body, as opposed to where Commander Humes placed it in CE 385.
Now where CE 385 is relevant is that it shows the only position as where the entry point must be. And why, because any lower would cause damage to the lung and as you state it was not damaged.
And here is where your problem is, as well those who support the SBT, a point any lower in the body such as, CE 903, places the entry wound lower than CE 385. And why is that important? It places the wound below Costa IR [ whereas CE 385 places the entry above it ] and therefore requires the bullet to pass through the lung. In the image below the yellow dot is roughly where CE 903 places the wound and as you can see that now requires the bullet to pass through the lung.
This is the difference between “theory” and “reality”.
I have no dispute about points 2 – 4. I agree they are issues.
Another problem you, and other SBT supporters, is to confuse the wounds of JFK and JBC. For the wounds of JBC to be relevant to the SBT theory then first and foremost the wounds on JFK must first and foremost support the criteria of the SBT. It is only when the wound to JFK support the SBT that the wounds to JBC are relevant.
And your problem is that the wounds to JFK do not support the SBT. Yes, you can fix, as Dale Myers has done, a trajectory from the TSBD to the back of JFK. You can also create a trajectory, as Dale Myers has also done, between the back wound and the throat wound. But what he, and all other have done and I suspect you are also doing, is to ignore what happens when the bullet had to pass through JFK’s upper chest area.
Between the TSBD and JFK’s back there are no obstacles. Inside the upper chest area is a veritable minefield of obstacles.
If your position is that the entry point is as described in CE 903, then you have placed the bullet roughly where that yellow dot is. In doing that the lung has got to be pierced, there is no other trajectory the bullet can take. Only CE 385 escapes that, but then it leaves open where did the back wound come from. Everything looks fine as explained by Dale Myers, but he, and it also appears, to me, that you are also not dealing with the reality of what would have had to happen if such a bullet entered the body, as described by CE 903.
You ask:
“Given the above facts, tell me again how the SBT is an impossibility.”
It is an impossibility for a variety of reasons, but the most compelling for me is that had a bullet entered as described by CE 903, then not only would the lung be damaged but on the bullet’s travel towards the throat it would have been bound to pierce the jugular vein which is in the bullet’s direct route towards Trachea rings 3&4.
That is the difference between theory and the reality of the position of organs in the upper chest area of the human body.
James.
-
David,
You said:
“Something that conspiracy zealots like DiEugenio always totally ignore when discussing the issue of the Single-Bullet Theory is Warren Commission Exhibit 903, which is a photo that proves for all time that the Warren Commission (including Mr. Ford) did not need JFK's upper-back wound to be "moved" up into the neck of the President.”
Well there is another side to that argument and it is this. Something that supporters of the Single-Bullet Theory always totally ignore is what would happen had this “bullet” actually traversed the area of the upper back and chest area as described by the placing of your entry and exit points.
Are you aware that CE 903, is not what Commander Humes stated the trajectory of this bullet was. CE 386 describes his trajectory. The difference (and the reason for that difference) is the avoidance of major damage to the arteries, veins but most of all, the Lung.
In CE 386 the entry point is above Costa IR, and thereby well above the position of the lung. In CE 903 the entry point is somewhere between Vertebrae 3 and 2 and directly behind the upper third of the lung.
The importance of that is that the only trajectory this bullet could take to get to the neck exit point is through the lung. Not only would the lung have collapsed, it would have also been severely damaged.
Understandably, and quite rightly, JFK researchers have seriously criticized Humes for these three drawings. But Humes had a reason for each of them. The reason for CE 386 was that he knew what would happen had he placed the entry point where CE 903 has it placed. CE 386 was the only entry point where Humes could argue that the SBT would not cause significant damage to JFK’s upper chest area.
Of course that raises all sorts of other problems, but that is not the issue here.
The issue here is very simple. If it is your position that the entry point is, as described by CE 903, then the damage caused to JFK at that point [Z224 – Z225] might well have endangered his life there and then….even before the head shot.
The Achilles heel of the SBT is not the arguments about where the entry and exit points are on the bodies of JFK and JBC (that you seem so preoccupied with) it is the ignoring of the inevitable damage that had to be caused as a consequence of the required internal trajectory through JFK’s neck consequent on where you have placed the external trajectory points.
James.
-
Patrick,
Are you confusing the Greer door opening on Houston Street, with the LBJ follow up car which did have a door open?
James.
-
Cliff,
When I made that last posting, I was just casually thinking about where the bullet could have come from and decided to post this concern. Soon after I began to regret I had made such a statement. However, since then, I have not been able to get the thought out of my mind. If the shot came from the North Knoll, which is certainly what I would have considered to be the natural home for such a shot, the more I keep asking why was the right side of JFK injured and not the left side.
Since that posting I have done some reading about what this injury looked like when Kennedy arrived at Parkland. I was wanting to see if the information could help explain why the right side was damaged. However as a result of the reading I am now changing my position regarding damage to arteries and blood vessels. I now agree with you that indeed they were damaged.
My reasons are as follows:-
Here is what Malcolm Perry said amount of blood in the upper chest area:-
1. “As I noted, I did not see any underlying injury of the pleura, the coverings of the lungs, or the lungs themselves. But in the presence of this large amount of blood in this area, one would be unable to detect small injuries to the underlying structures.” H3 P. 371
First, he makes it clear that the amount of blood in this area makes it very difficult to see the smaller injuries.
2. “I noticed there was free air and blood in the mediastinum and although I could not see any evidence, myself any evidence, of it in the pleura of the lung the presence of this blood in this area could be indicative of the underlying condition.” H3 P. 370
Second, the middle section of the chest, the “mediastinum”, was full of blood.
3. “There was there was so much blood that the tissues were discolored.” H 6 P. 11
Third, and this is the critical evidence for me, within around 10 minutes there was so much blood in the area it had actually discolored body tissues.
4. “This bruising, as you describe, would have been obscured by the fact that there was a large amount of blood, hematoma, present in the neck and the mediastinum and hence all the blood tissues were covered by this blood.” H3 P. 381
Specter asks Perry whether he saw any bruising of the neck muscles. Perry replies that there was so much blood it was impossible to see whether they had been bruised.
5. “Mr. SPECTER. Was there blood in that area which tended to obscure your view?
Dr. PERRY. It was exuding blood during that procedure and thus I did not examine it very closely.” H3 P. 388
Perry says that the blood that was flowing made it difficult to see and he did not examine further.
6. “There was no evidence of a hemothorax or a pneumothorax through my examination; only it is sufficient this could (not) have been observed because of the free blood in the mediastinum.” H3 P. 832
There is a typo error here. It is clear that Perry must have said “not”, without the word his sentence makes no sense. So what he says is that his examination of the upper chest area was inhibited by the amount of blood.
Taken together, it is clear to me that a vast amount of blood was in the area, and enough to discolor body tissues within around the 10 minutes between the assassination and when Perry did the tracheotomy. That makes it clear to me that arteries had to have been damaged. Humes had to have both observed it as well known that and therefore was aware he was lying when he declared in both testimony and in the autopsy protocol that they had not been damaged. It is true that Malcolm Perry, in his testimony also said they had not been damaged, but that may be because he was severely lent on. His testimony, as described above, is strong evidence that they were damaged.
2. Returning to the problem of where the shot came from, the first thing I did was look for evidence of what the shot and damage looked like in Parkland.
Where the shot struck:-
Dr. Carrico:-
This was probably a 4-7 mm. wound, almost in the midline, maybe a little to the right of the midline, and below the thyroid cartilage. H6 P. 3
I am taking this to mean Right as looking towards the body and not the body’s right. If it is the body’s right then that is not facing any gunman at Z 190. The turn at Z 190 has hidden that side of the neck. That part of the neck is not facing any gunman until after Z 225
What damage was done by the bullet:-
Dr. Perry:-
a. There was an injury to the right lateral aspect of the trachea at the level of the external wound. H6 P. 10
b. The trachea was deviated slightly to the left. H6 P. 10
c. I noticed a small ragged laceration of the trachea on the anterior lateral right side. H3 P. 370
d. I could not see any evidence, myself any evidence, of it in the pleura of the lung the presence of this blood in this area could be indicative of the underlying condition. H3 P. 370
Now I am well aware that the images below are in 2D and not 3D. I accept that 3D with, first access to the Y axis as well as viewing of all 3 axis’ together, gives a far better understanding. I therefore accept that what I have below is limited.
However I do feel, even though it is in 2D, I feel this does raise questions – the biggest one being why given the trajectory of the bullet and the way Kennedy was facing at the time did the bullet damage the right side and not the left side.
It is not my position that Z 190 was the moment, I just feel it had to be around that area and I have used Z190 as my example. Although JFK’s head moves towards the left from Z190 – Z200, his body position is still the same.
The turning of the head to the right is a serious problem, because Dr. Carrico states the impact was to the right of center. Any head movement to the left makes that much more difficult.
See image below:-
What the image shows:-
Image a shows the model with the head turned to the right similar to Z190.
Image b is a close up of that image.
Image c is a crop of Don Roberdeau’s map with a line drawn from the Grassy Knoll shooter’s position. Don suggests JFK’s head is fully turned to the right, hence the red arrow. In Z190 I am not sure his head is turned so far to the right.
Image d highlights the damage on the model.
My problem is this:-
1. The bullet will have struck the flesh on the neck before it gets to the trachea. Why does the bullet not carry on its leftward trajectory. There is no bones etc to stop it at this point. The head, at that point is turned to the right thereby offering the left side as a path and avenue.
2. In order for it to bend the trachea to the left, as Perry stated, the bullet has to have impacted to the left of the midline, and by quite some distance. Thereby allowing the bullet to damage the trachea in that manner. Carrico was clear that the bullet struck to the right of the midline. That makes perfect sense given how Kennedy’s head was turned at this point.
3. The bruise of the right side of the trachea, that Perry testifies to, makes it very clear that the bullet travelled on the RHS of the trachea. I don’t see how it could do that.
The kernel of my problem is this. It is best seen on Don’s map. In order for the bullet, being fired from this position and impacting as described by Carrico and Perry, the bullet would have to make a very significant change in direction after impact in order to do so. It has to be something in the order of 40-50º and I cannot see a reason why it would do so. Now I know bullets will do strange things when traveling through a body and changing direction is very common. But this change is not just very significant but had to take place immediately on impact if it is to damage the areas described.
You mentioned, Cliff, the Badgeman/Blackdogman as a source for the shot. That would not help. A shot from that source would make the angle more obtuse and compound the problems.
I have been wresting with this problem over the last few days and there are only two sources that would allow a shot to impact the right side of Kennedy.
a) The South Knoll. I am reluctant to seriously consider this. Although Gary Mack’s study about “Inside the Car” was flawed with regard to the gunman’s position, he was studying Z 312 and not Z190. However even at Z190 I am not sure how much of Kennedy would be exposed for such a shot.
The Storm Drain area at the west of Railroad Car Park. From what I can see that would give a perfect line of fire to both strike the neck right of the midline and also travel left of the trachea and be able to do the damage as described. Even Gary Mack’s gunman suggested this was a possibility.I do not have any solutions, I just don’t have an answer as to how the bullet could strike where it did and not damage the left side of Kennedy.
James.
-
Sounds like Flechette, to me...
Cliff,
I agree there is a logic to the Flechette idea. But from where could it be fired from?
At a rough guess the angle of decline within JFK's body will be something like 15-20º. So that suggests the gunman has to be on a higher plane than street level.
If your position is the North Knoll, I am not sure that the area damaged would be JFK's right side. There is the turn of the road at say Z190 as well as the position of Kennedy in the car at that moment. All would suggest that logical area to be damaged would be the left side as opposed to the right.
To give some idea what I mean I have drawn a graphic on Don Roberdeau's map. The red arrow represents the direction JFK's head is turned. the black arrow the direction of the car and by implication the direction JFK is seated. His body is not turned, it is just his head. The blue arrow is a line drawn from the GKS. As can be seen were a shot taken from here the damage should be to JFK's left side and not his right, which was damaged. If Badgemman were used the angle would be worse. See below
That brings up back to the South Knoll, and who would use a Flechette from the South Knoll?
James.
-
Pat,
Thanks for the article. It is exactly the kind of information I was looking for.
Although your focus is proving how illogical the idea of the SBT is, you still raise very important questions for the throat wound.
Question 1:- Your references on the kind of damage, that even the Oswald rifle could achieve and it was not the most high powered rifle, is it your position that it was not that kind of rifle that created the throat wound? I have been grappling with the question of how such a bullet flying at such speed first did not go right through the throat and second did not create much more damage. I discount Humes comment about “slid between”. I agree it was an outrageous comment but it was because Humes knew there had been no such wound and he also knew the kind of damage such a bullet would incur had it really inflicted such a wound.
Although Malcolm Perry, when talking to the HCSA, suggests that although he certainly did not examine the throat area he did see sufficient to have the impression that major damage had not be inflicted in the throat.
If he is right, and I am not saying he is, there is a real dilemma. The kind of damage you describe ought to have taken place, yet appears not to have happen. Yet, at the same time, experienced doctors, first impressions ( and yes I agree there was nothing more than that ) were that the wound they were looking at was a bullet wound.
Do you have any thoughts on this.
Question 2:- I had noted Perry’s comment about the laceration to the right side of the trachea as well as Carrico’s comment. Taken together it suggests that something had to have passed in that direction. You may have noted the reference I gave from Perry who suggested that it appeared to him that there had been no damage to the main arteries. So whatever did pass in that direction appears not to have created the kind of damage you so excellently describe.
I have read suggestions that it could be a low powered velocity shot. In one way that makes sense, but then I am forced to ask why anyone would want to bring a low powered gun when intending to assassinate the President of the United States?
Do you have any thoughts on this?
Question 3:- Finally there is the directional issue. It is clear from all the evidence that the right side of Kennedy was injured. I.e. the right lung, the right strap muscle, the right side of the trachea.
If the shot was coming from the North Knoll, that position is left of Kennedy’s position. Therefore the natural area to be damaged by such a shot ought to be the left side. But it is Kennedy's right side.
Now there are two moments: one around Z 160 and the other around Z 190 when Kennedy’s neck is turned to his right. However his body is still facing forward and I am not sure any shot, no matter how far Kennedy's neck is turned, would have a bullet travel down the right side. I am wondering if, even in that situation, the bullet would not still progress down the left side.
The ideal position in order to damage the right organs in Kennedy would be the South knoll. But I can’t get my head around the idea that anyone would be positioned over there.
Do you have any ideas on this?
Thanks for the article. I’ll follow up your references as well as the full chapter on your site.
James.
-
John,
I am beginning to understand that. I am much more aware of the power of the forces a bullet creates as it passes through a body.
When I started this thread, I was mainly focused on physical contact. I did not give much attention to the forces created by a bullet as it passes through an object. Now I am.
Your suggestion is one I will take on board. An area that I am about to start reading about is balstics. I don't, as yet, have a clear idea what happens when a bullet passes through an object like a body.
Thank you for your observation.
James.
-
Cliff,
To make the argument clearer to follow I have extracted the main points of your post and addressed them separately.
a) What were the experts conclusions on the Air Pocket?
Professor G.M. McDonnel:- “In the pre-autopsy radiograph ( that is X-Ray 9 ) of the chest shows air in the soft tissues of the right supraclavicular area of soft tissues.” That is around the C7 area. Addendum C P. 219
Professor David O Davis:- “In the pre-autopsy film shows that there is some subcutaneous or interstitial air overlapping the right C7 T1 transverse processes.” Addendum D P. 224
Professor Norman Chase:- “Air was noted in the subcutaneous tissue in this same region caused by the passage of a missile and/or air entering the region due to the tracheostomy incision.” Addendum I P. 228
Professor William Seaman:- “He said the transverse process appears abnormal with air present (possibly by-pro of tracheotomy) calling it "* * * highly suspicious compared with the other side.” Addendum 1 P. 322
The airpocket overlying T1 and C7So to sum up. All four agree that there was air in this area of the upper chest. One, Professor Davis, observes that this air pocket overlapped the C7 T1 area. Two of the doctors, Chase and Seaman, suggested that the air pocket originated from the wound to the throat.
c) The position of Commander Humes in the argument
This is a point we are just going to have to disagree upon. You appear to consider that everything Humes says is a lie. From what I can see you have no foundation for saying that. Humes certainly was less than truthful with CE 385, the SBT chart, but how can you prove he lied about everything else. Unless I can demonstrate that Humes lied on an issue I have chosen to believe him.
However it would be helpful, in furthering the conversation, rather than you saying Humes is a xxxx all the time, that you provide the evidence that makes you want to contradict Humes statement.
That way we ought to be able to widen and deepen the quality of the conversation. It is difficult to find an appropriate response to Humes is a xxxx.
Supporting image:-
 The Hematoma is damaged blood vessels
The Hematoma is damaged blood vesselsHumes said this about the damage to the top of the lung:-
“As depicted in figure CE 385, in the apex of the right pleural cavity there was a bruise or contusion or ecomymosis of the parietal pleura as well as a bruise of the upper portion, the most apical portion of the right lung.
It, therefore, was our opinion that the missile while not penetrating physically the pleural cavity, as it passed that point bruised either the missile itself, or the force of its passage through the tissues, bruised both the parietal and the visceral pleura.
The area of discoloration on the apical portion--of the right upper lung measured five centimeters in greatest diameter, and was wedge shaped in configuration, with its base toward the top of the chest and its apes down towards the substance of the lung.”
See Image A
Humes point is that this bruise was around 5 in diameter and was pyramid in shape. As you can see X-Ray 9 shows this shape. So I assume we agree there was a shape on top of the lung similar to what Humes describes. The clear version of the image allows you to inspect whether I have drawn my Cyan line correctly.
Now your point, as I understand it, is that this damage is the consequence of one of the blood vessels in the upper chest are being damaged.
That makes no sense. This shape we are talking about is attached to the lung: it is described as being part of the lung. The X-Ray appears to agree.
I concur that it is a blood vessel that caused this damage, however the vessel responsible was inside the lung, not outside. It was the damage to this vessel that created the swelling within the lung and thereby created the swelling we see outside the lung. As Image B shows there are blood vessels close to the Apex of the lung.
Maybe you can explain how an artery, that is some distance from the lung, when punctured then creates an object that attaches itself onto the top of the lung? I don’t see that.
e) JFK coughing up the projectile
My argument has nothing to do with whether JFK was, or was not, attempting to cough up the projectile.
As image D shows the cervical nerves control the movement of the arms.
JFK may well have been attempting to cough up the projectile, I have no idea whether he was or was not, that is not a concern of mine. What I had suggested is that the movement of his arms were an involuntary action triggered by the damage to his nervous system.
If you look at image C and you will see all the nerve strands the emanate from cervical spine. These nerves all connect with the areas in the arm. You will see them listed in image ??. My point is that the bullet damaged these nerves and the movement in JFK’s arms was involuntary. It was the damage to the nerves that caused the arms to move in the way they did.
f) The speed of the air pocket being created
One of your arguments is that the air pocket around C7 and maybe even T1 had an impact on the missile.
My argument is that the bullet was moving at such speeds it was impossible for the air pocket to be created in the upper chest area.
In Gerald Posner’s paperback version of “Case Closed” Appendix A P. 6 is a diagram purporting to describe the path of the bullet, but more important indicating the speed of the bullet as it struck JFK. It is his view that when the bullet struck it was moving at a speed of 1,750 feet per second. Now I have no idea what gun was being used that fired the bullet that struck him in the throat. Nor have I any idea what speed the bullet was moving.
However, for the sake of argument lets assume it was moving at 1,750 feet per second. For a person of 6 foot it is argued that the circumference of the neck is 12 inches making the diameter 3.819 inches. I feel JFK’s neck was larger so, for the sake of argument, lets assume the circumference was 15 inches. That means the diameter would be 4.774 inches.
Now if the bullet was traveling at 1,750 feet per second it would pass through the throat in 0.0002273 seconds.
I suggest that there is no way the air pocket could be created faster than that.
g) The possibility that arteries were damaged
I understand that the average pressure in the arteries is 80 mm Hg. I have no idea what that means. However having seen images of artery damage on films it is a common sight to see spurts of blood as a consequence. We all know that fluid will always find the easiest route and that would be out of the hole created by the bullet.
It is true that once the head shot took place the pressure of the blood would rapidly decrease. However between the point of the throat shot and the head shot there was 10.75 seconds. That was more than sufficient time for the escaping blood to find its escape route. That would certainly have been visible on the Zapruder film.
Perry was questioned by the HCSA and one question he was asked was whether there was any sign of artery damage in the upper chest area. He replied: “there was no evidence of a major arterial injury. And the artery, the course that's closely applied to the trachea is the common carotid artery at that level But it was not injured” Addendum I P. 304
Taken together, I would argue that there is no evidence that any of the arteries were damaged.
James.
-
James
My position is that any damage to T1 is incidental to the salient fact that an air-pocket overlaid the right C7 and T1 transverse processes. The angle of that air-pocket -- from T1 to C7 -- points back in the general area of the nicked trachea. A path above C7/T1 would account for the damage you see in that area, right?
James, the highest back wound you can justify is T2. That's too low to have created the air-pocket. The air-pocket was the result of a round that entered the throat and stopped in the vicinity of T1. The round did not exit; and no no round was recovered at the autopsy.
If you have a fact based argument to challenge the above, I'd like to hear it, James.
Cliff,
When we discussed during this thread, it was my impression that damage to T1 was a fact in your opinion. It certainly was something you often pointed to. As I understood it, creating that image with the ABC trajectory line was important to you since it created a direct path from the Trachea to T1. Are you suggesting now that damage to T1 is not an essential issue.
Having studied HCSA Volume 7, as well as the appendixes, it is clear to me that T1 was not damaged. Even though on P. 99 the Panel state that it was damaged.
I am also less certain that the bullet travelled close to the Trachea. I was always astonished that traveling on that route the bullet did not damage the main arteries, including the jugular, that lie in that area. If you remember there was only one route I could find that would avoid these arteries.
When Humes was being interviewed by the HCSA medical panel he said this about the route the bullet took. "It had to have passed medial to the right carotid bundle." Vol 7 Addendum I P. 256 It made perfect sense. The route had to be to the right of the arteries, or in the case of the model below, to the left of the arteries. Of course he was talking about the SBT. And that is why in CE 386 we see his bullet entry point on the extreme RHS and miles away from the actual position of the back wound. Although Humes never mentions it during the Warren Commission, the reason he places the entry point there is because if it were vertically anywhere near the position of back wound the bullet's trajectory would be bound to damage one or more than one of these arteries. And that is why when Hume created his path for the bullet, it was "to the right carotid bundle." But by the same token, it now means that the bullet that entered the throat from the front must also be "to the right carotid bundle." Otherwise it also would have damaged the major arteries.
Dale Myers and the others who use the position of the actual back wound for their entry point are oblivious to the fact that their trajectory places the bullet going right through the "carotid bundle." Even if their trajectory for the SBT avoids going through the lung, it cannot avoid hitting one, or more, artery. This is an area I am going to be returning to.
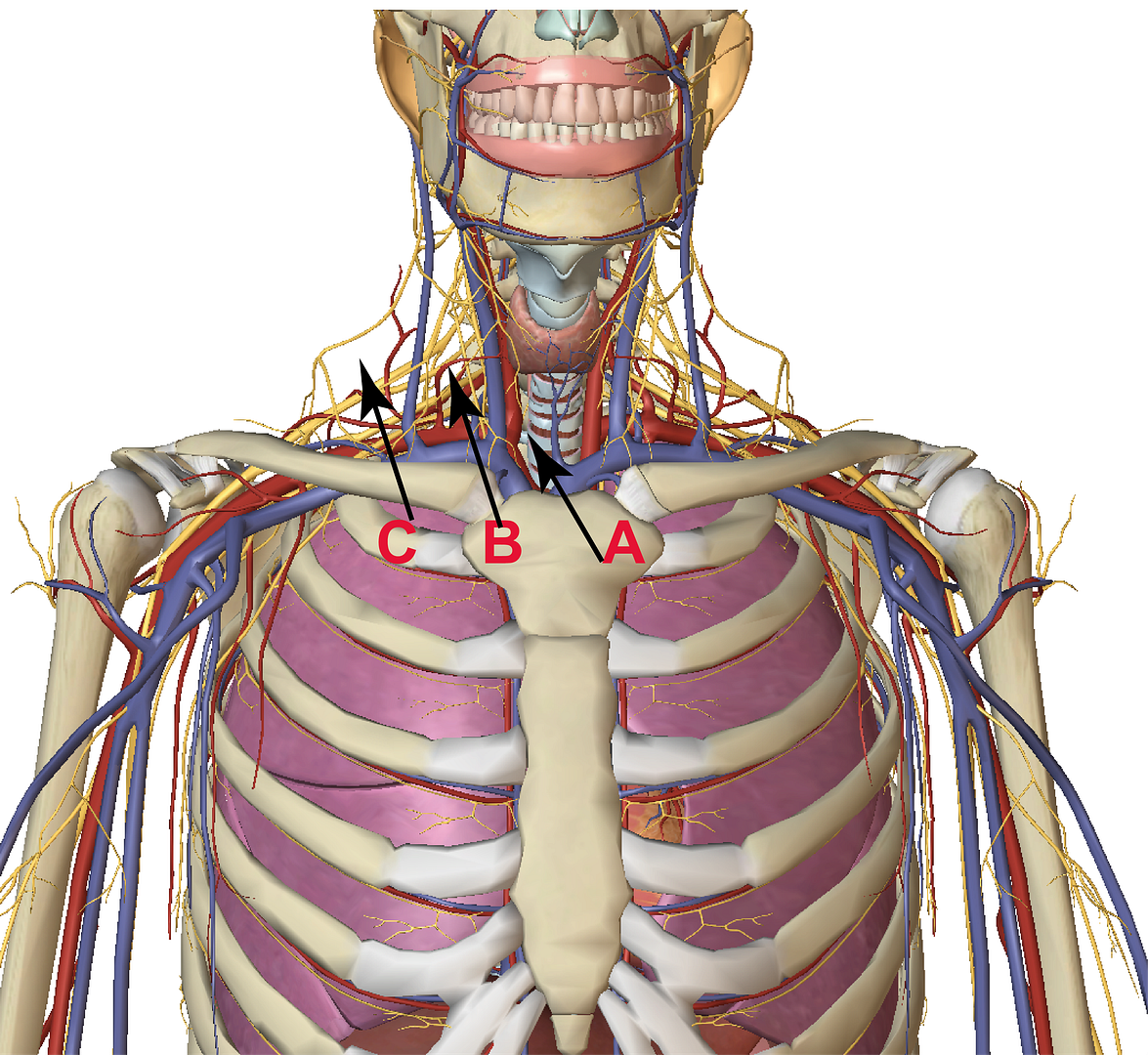
Initially my position had been for the bullet to travel through the path indicated by A. That said I could never understand how traveling on this path the bullet did not damage an artery. That is why I now consider path A to be no longer a viable path. It is just too dangerous a path.
Humes' point is that the path had to be B or C. I suspect B would be the preferable one. It still takes the bullet close to the arteries, but nowhere near to them that path A does.
So taking up your point about the path for C7 T1, my revised position is that the bullet did not travel anywhere near C7 or T1.
The other interesting point about these new trajectory paths is, that having included the nervous system ( they are the yellow lines ), the damage to the nerves was caused by the bullet. In that trajectory it is bound to have struck some of these nerves. This is important because the raising of JFK's arms is an involuntary action by him that is caused by damaged nerves. I did post earlier an image showing the areas on the arms that were controlled by specific nerves. The damage to the C6 C7 muscle may well have damaged the nerves, but I suspect that the bullet cut nerves, shown above, on its route. It is these nerves that force JFK's arms upwards.
With regard to the air pocket, the various experts who looked at the X-rays all agreed to their being an air pocket. They all were of the opinion that it was created by the damage to the trachea. In that case the air pocket is irrelevant to any discussion. It would not have been created and positioned itself until long after the bullet had completed journey. The bullet was going to fast for any air pocket to have a chance of forming and then impacting on the route and trajectory of the bullet. The air pocket was not there prior to the bullet entering the body. It was created as a consequence of the bullet entering the body and was not in position until after the bullet had completed its journey. That is why it played no part on the path and trajectory of the bullet.
The back wound, be it at T3 or T2, had no impact on the creation of the air pocket. The HCSA experts are unanimous that it was the trachea wound that was responsible for the air pocket.
Cliff, you say that the bullet “stopped in the vicinity of T1”. No it did not. As I have pointed out above, the path for the bullet took it nowhere near T1. Yes, I used to think it did travel near T1, but I no longer do. A path such as that, i.e. path A, takes the bullet far too close to the arteries. The bullet would have been bound to damage one or more arteries had it been on that path.
James
-
James R Gordon said,"My conclusion from all this is that the T1 Transverse Process was not damaged."
On the whole,after following this debate,I am inclined to agree with you James.Its just better done with the 3D Images,a picture paints a thousand words,so as to speak.
Malcolm,
Thank you for your support.
I agree images would have helped and since the argument revolved around the X-Rays 8 + 9, maybe I should have used them.
After the main series of postings I felt I should delve in more detail into the HSCA exhibits and reports. Up until then I had mainly used the WC as my evidence support.
In the case of this posting I was curious what the evidential foundation Cliff had to constantly to state that T1 had been damaged. I knew it came through the HSCA, and so I read Vol 7, along with submitted reports. Cliff's confidence had always been a worry to me, I did see where the evidence was to give Cliff such confidence. Having thoroughly read Vol 7 and the relevant appendixes I now see there is no basis for his position. Although I have greatly enjoyed reading the material, when you delve into the appendix evidence you see that the HSCA were just as selective with their evidence as were the Warren Commission. Having commissioned these experts, they then ignored half of then and were selective with one of them. The one they did fully use appears to be quite an interesting character in himself.
Although I had initially been looking for the basis for the the idea that T1 had been damaged, what was central in my mind was the damage to the C6-C7 cervical muscle. This is an issue I am very interested in. I was deeply interested in what these experts had to say about C6_C7. It was really illuminating. They are all over the place. At the moment I am not sure if it is because they have no idea what they are seeing, or whether they do, and therefore understand the difficulty it places them. This is the subject of a future posting.
I found a superb comment by Commander Humes that has really clarified his thinking on the SBT and in doing so has also clarified mine. In my earlier postings on the SBT I was really adrift as to what path this bullet could have taken. By that I mean the essential paths that both the Single Bullet, itself, as well as the bullet that entered through the throat had to have taken. Humes comment is so clear and so logical that I am shocked I did not see the point before. This will also be the subject of a future posting.
In the follow-up posts I will use images and movies to support my text. I understand, as well as agree, they make the understanding of my argument much clearer.
Again thank you for your support.
James.

Logical implications of nearly simultaneous heads shots
in JFK Assassination Debate
Posted
Mark,
Sorry to correct, but I believe it was actually 2.4 seconds to reload the gun. It was the equivalent of 42 Zapruder frames.
James