

Robert Prudhomme
-
Posts
4,105 -
Joined
-
Last visited
Content Type
Profiles
Forums
Events
Store
Posts posted by Robert Prudhomme
-
-
We always assume the long axis of the nick indicates the direction the bullet was travelling but, is this a fair assumption?
If this part of the tie was the tail of the tie, and the part with the nick was folded over as it entered the base of the tie knot, leaving the cease of the fold exposed out to the left, a bullet fragment equal in diameter to the length of the nick could have made the nick.

Could the nick have been on JFK's anatomical right, as seen 3 inches up from where the tie was cut, and the blood really did run down?
-
No matter.
It all depends on what was defined as "up" when this tie was worn, as there seems to be a great difference of opinion about where the nick actually was on the tied tie.
Ever notice there seems to be a bit of blood spattered on the left hand side of this section of tie, also?
-
Here is something to think about. The wound in JFK's throat was described as an almost perfectly round wound of 3-8 mm in diameter. Yet, Perry described the tear in the trachea as not being straight across the trachea. The wound he described was a downward ranging wound that began at the 2nd tracheal ring and left the trachea at the 3rd tracheal ring.
How could a bullet on an obvious downward trajectory make a nice round exit wound?

Skull and cervical vertebrae showing trachea with rings. Rings are counted down from the top.
What, no one has an answer to this question?
-
Cliff
Yes, there was room for a bullet to strike his throat beneath the Adam's apple. However, if you have carefully read my thread about the "shallow" back wound, you will see the undeniable medical evidence that clearly demonstrates the tracheal wound was too far below the laryngeal prominence (Adam's apple) for it to be even close to being above the top of the shirt collar. The location of the tracheal wound is based on Dr. Malcolm Perry's observations. He placed this wound between the 2nd and 3rd tracheal ring. If you prefer, we could go with Commander Humes' observations, which placed the tracheal wound between the 3rd and 4th tracheal ring.
Either way, the tracheal wound was a minimum of one inch below the top of JFK's collar.
P.S.
Before denying this statement, please at least look at the medical arguments I have made.
-
Hi Chris
Which bloodstain are you referring to? There were so many of them.
-
How could a bullet on an obvious downward trajectory make a nice round exit wound?
It was a wound of entrance from a hit circa Z190 as established by ear and eye witnesses Phil Willis and Hugh Betzner.
Betzner said he took his #3 photo (Z186) immediately before a gun shot.
Willis said he took his #5 photo (Z202) in a startle-response to a gun shot.
I agree Cliff.I also agree with your post 327. I feel these are question of a fundamental nature to understanding what happened that day.
James
As I have clearly demonstrated to you that an above the collar throat wound is an impossibility, perhaps you could show me the trajectory of a bullet that could make an entrance wound in JFK's throat by passing under the collar button.
-
-
As the muzzle blast is eliminated by a silencer, the only sound heard by witnesses is the bullet breaking the sound barrier as it passes by them. Once it passes them, every vertical hard surface the bullet passes also reflects this sound as an echo. Therefore, the majority of sound heard by witnesses close to the source of the shot will be echoes returning to them from the target area of the bullet, giving the impression this is where the bullet originated from.
To grasp the above concept, it must be remembered that a projectile does not just make one sonic boom at the point it breaks the sound barrier but, rather, makes one continuous sonic boom all the time it is travelling faster than the speed of sound.
If a silencer was used, this was one of the main reasons, as well as to conceal the source of the shot and give the shooter a chance to escape. It is small wonder there was so much confusion as to the source of the shots.
-
Cliff
Did you ever read the post I posted showing how a silencer (suppressor) can make it seem to listeners that the source of a shot is actually down in the target area?
-
Here is something to think about. The wound in JFK's throat was described as an almost perfectly round wound of 3-8 mm in diameter. Yet, Perry described the tear in the trachea as not being straight across the trachea. The wound he described was a downward ranging wound that began at the 2nd tracheal ring and left the trachea at the 3rd tracheal ring.
How could a bullet on an obvious downward trajectory make a nice round exit wound?
Skull and cervical vertebrae showing trachea with rings. Rings are counted down from the top.
-
As I stated earlier, it is essential to the Single Bullet Theory that the bullet exited JFK's throat above the tie knot and collar. If the bullet exited JFK's throat below the top of the collar, the SBT is not possible, as the trajectory from JFK's throat to John Connally's right armpit would require the bullet to pass trough the tie knot, and there is no evidence of this happening.
I believe I have proved overwhelmingly that, given the position of JFK's "laryngeal prominence" or Adam's apple in virtually every photo of JFK wearing a shirt and tie, there is no doubt whatsoever the exit wound was below the top of JFK's shirt collar and, coincidentally, in almost perfect alignment with the so called "scalpel slits" below JFK's collar button.
As I believe wholeheartedly that this was a shot from the rear, the next step is to trace a path for the bullet from just below the external occipital protuberance at the base of JFK's rear skull to the left side of the bottom of his tie knot, and to see what evidence there is to support this.
-
The 3rd row of icons below the tie knot is 6 icons wide. Are you able to see this, Sandy? The two rows between this row and the knot show less than 6 icons because the front of the tie is squished in from the sides as it passes through the tie knot.
If the blade (front or widest part) of the tie is 6 icons wide going into the bottom of the tie knot, isn't it likely it is still 6 icons wide going across the front of the tie knot?
"I think it's even more unlikely that a commercially available tie would be made where the tie gets narrower and narrower as you move along it, then widens enough to accommodate an extra icon, and then return to the width it is supposed to be."
What on earth are you talking about, Sandy?

-
Mr. Von Pein, have you ever read Dr Finck's HSCA testimony about the back wound? Finck, as you well know, was chief of wound ballistics pathology for the Armed Forces Institute of Pathology.
Finck claimed that he attempted to use a metal probe in the back wound, but was unable to find the bullet track. He then testified that he ordered x-rays of the chest cavity in order to try to determine where the bullet went.
Yet the x-ray technician who took those x-rays testified that, when he took the x-rays of the chest, they showed an empty cavity because the lungs and other internal organs had already been removed. Now, it would appear to a logical person that if there had been a bullet track within the internal organs, removing the organs would also remove the evidence of a bullet track.
Now...are you also familiar with the Warren Commission testimony of Dr. Marion Jenkins? Dr. Jenkins testified that, because of "the obvious physical characteristics of a pneumothorax," doctors in Trauma Room 1 "put in a closed chest drainage tube."
Do you even know what a pneumothorax is? [THIS is where the copy of Gray's Anatomy would most likely be more beneficial than anything Mr. Bugliosi ever wrote.]
I would suggest you STOP right here and right now, and look up the definition of the term and then look up the primary causes of a pneumothorax. [Hint: Bullets passing between strap muscles in the neck are not listed as a cause for a pneumothorax.]
THIS is why I recommend educating yourself on exactly what the doctors were saying.
Since the most likely cause of a pneumothorax in a gunshot victim would be a bullet or bone fragment puncturing a lung, it would have been nice for the bullet wound pathologist, Dr. Finck, to have had the lungs still in the chest cavity to examine. This might have helped him determine with a better degree of certainty the path of the bullet.
But according to the x-ray technician who took the chest x-rays when Dr. Finck ordered them--and the reason he ordered them, according to Finck's HSCA testimony, was to try to locate a bullet in the chest cavity, if it was still there--the lungs had already been removed at the time of the x-rays.
And there is NO testimony on file that I can find that states that the lungs were thoroughly examined...at least to the degree that a bullet wound pathologist would have examined them. In his testimony before the AARB, Dr. Finck stated that "(t)he brain, the heart, and the lungs had been removed before my arrival."
Notice that in Dr. Finck's testimony, he insists on referring to the wound as one in the upper back, and not a neck wound.
Notice that--if you did your homework and learned what a pneumothorax is--somehow, the right lung had apparently been breached in some way.
Yet there is no mention of an examination of the lungs, or even a mention of when the lungs were removed...except that their removal occurred prior to the arrival of the wound ballistic pathologist [Dr. Finck].
The Warren Commission Report will NOT explain the significance of a pneumothorax to you. Nothing that Bugliosi wrote will explain that to you. But a textbook of anatomy and physiology, in tandem with a good medical dictionary, WILL give you that information. And they are unbiased. They give information, and have no agendas.
Which is why I recommended you consult an unbiased source upon occasion. NO film clip from a fake trial of Oswald will tell you how a pneumothorax occurs...or none that I'm aware of.
Mr. Knight has well expressed the true nature of JFK's back wound, and the ensuing respiratory condition and medical emergency referred to as a "tension pneumothorax".
While somewhat difficult for the layman to understand, a tension pneumothorax is actually quite simple to explain.
In JFK's case, a fragmenting or a frangible bullet would have entered his back at about the level of the thoracic vertebra T3. Entering at this point, it would have gone directly into the top of his right lung, come apart and stopped midway through his right lung.
When JFK was laid on his back in Trauma Room One, it is likely the wound made by the bullet into the back of his chest cavity would have been sealed by his flesh pressing against the table.
JFK was intubated by Dr. Carrico, who inserted an endotracheal tube down JFK's trachea to a point where the tip of this tube would have been well above the two bronchi leading to the lungs.
Dr. Carrico inflated the cuff of the endotracheal tube in order to seal the tube against the inside of the trachea. Carrico misjudged the insertion, despite using a laryngoscope to guide him during intubation, and the inflatable cuff was placed slightly above the tracheal wound, and a perfect seal was not made against the inside of the trachea.
Following intubation, JFK was connected to a respirator, and positive pressure ventilation was occurring in his lungs. It was this higher than atmospheric pressure ventilation that brought about the tension pneumothorax.
With the tearing of lung tissue, the right lung would have lost its airtight qualities and would have collapsed. With each inspiration from the respirator, higher pressure air would attempt to inflate the right lung, and air would escape from the lung into the right pleural cavity. On exhalation, the lung would collapse again, preventing air in the pleural cavity from escaping. Within the space of a minute, enough air would build in the right pleural cavity to prevent any air from entering the right lung at all. The left lung, being in its own pleural cavity, would still inflate but, eventually, enough pressure would build on the right side to impair the left lung, as it exerted pressure laterally to the left, and JFK would asphyxiate.
Following intubation and connection to a respirator, Dr. Carrico listened to JFK's chest for breath sounds. He found the breath sounds to be diminished, due to some respirator air escaping through the tracheal wound, but he also observed the breath sounds in the right lung to be greatly diminished, in comparison to breath sounds in the left lung.
Dr. Carrico's observation of reduced breath sounds in the right lung would be universally interpreted in the medical world as being caused by one thing, and one thing only; a tension pneumothorax building air pressure in the right pleural cavity preventing additional air from entering either the right lung or the right pleural cavity.
There are other signs, observed by Drs. Perry and Carrico, that are unmistakeable signs of a tension pneumothorax, but I will save them until DVP has had a good chance to rant at my post first.
-
LOL Well, that sure stopped everyone in their tracks.
This is so typical of JFK assassination research. There are so many things that everyone just "knows" are true, such as JFK's back wound being a "shallow" wound, and the nick in the tie just having to be in the tie knot itself.
As I said, think for yourselves. The answers are all there if we just apply a little of the old grey matter.
For starters, if the wraps in the tie knot are made up of the "front" or wide part of the tie, what else is in the knot that is not part of the "front" or wide part of the tie? And might only be five icons wide?

-
Rotated or perspective adjusted; who cares? Either way, once the posts and gate are lined up and plumb, Oswald is leaning so far to his right he could never stand like that.
-
Ashton
How do you know the nick was in the tie knot?
-
"Oswald's" lean is even more pronounced when the perspective is corrected.
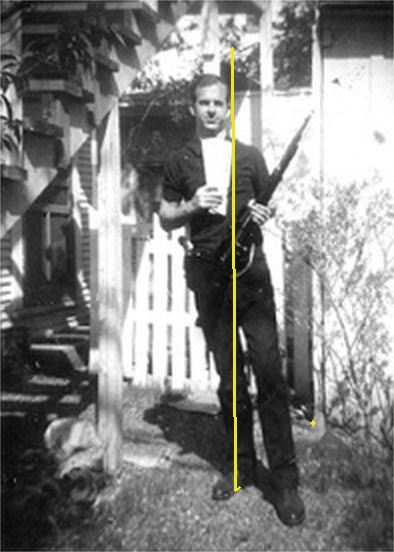
This is one of the few sensible posts in this entire thread. Good show, Ray! After all the scientific double talk, Ray simply rotates the photo to make everything plumb, and shows us why the photo has to be a fake. Oswald going down!
-
The farthest post to our right is 8° off of vertical. Your computers are full of baloney.
Regardless if it is 1.9, 5 or 8 degrees, you straighten that picture out by any of these amounts and Mr. Oswald has too much weight out the right side of his body, and he will fall over.
-
"There are none so blind as those who will not see."
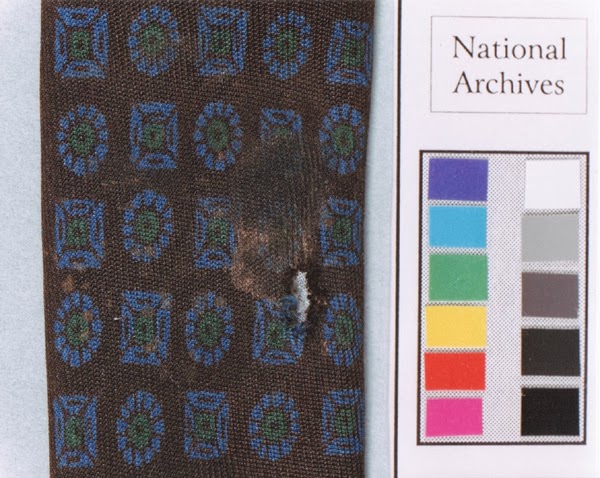
Just to refresh everyone's memory, here is a sample of the tie, and the reason Ashton and Sandy are completely out to lunch about the tie knot:
There is no escaping what I am about to tell you. As seen, the icons on the tie are rectangular and ovoid, and they are longer going lengthwise on the tie than they are crosswise.
Five icons also take up more space on the tie lengthwise than crosswise. Measured above, five icons measured:
Lengthwise = 117 millimeters
Crosswise = 77 millimeters
A difference of 40 mm or 33%.
If what Ashton and Sandy are telling you is true, the top two icons would be part of a section of tie going down behind the face of the tie knot. It would be a bizarre coincidence to have these two icons even come close to aligning with the rows below them and, even if they did, these two top icons would be 33% closer to each other than the icons below them, which they are most definitely not.
Sandy's only explanation for this is that it is a "coincidence". I guess that's what you say when you run out of logical arguments.
Ashton doesn't even attempt to explain the problem but, rather, carries on like a little girl.
Do not be taken in. Think for yourselves, people.
-
Sandy, you won't have to bother trying to post a zoomed in closeup of that low-res, pixelated image. The image I originally posted of JFK at Love Field is high enough resolution and has all the information needed for those who have eyes to see and even a modest modicum of intelligence—and who aren't blinded by their own biases. Below is that image blown up to 800 percent. It has not been retouched in any way. The levels have been adjusted simply to make features more prominent and easily visible.
There clearly, inarguably, OBVIOUSLY is a curved horizontal EDGE OF THE TIE KNOT AT THE TOP, which I have indicated by making an animated GIF with a white line, so that perhaps even those who have gone stone cold blind from living in a fantasy "theory" for too long might be able to find with both hands. Here it is:

It should be obvious even to the most prejudiced and obtuse (but I repeat myself) that the two icons ABOVE that obvious line of separation CANNOT POSSIBLY be a continuation of either vertical line of five icons BELOW that separation. They are nowhere near the same size, nor aligned with those below, nor even GOING IN THE SAME DIRECTION!
Those with a disinformation agenda can whine about it and twist the facts all they want, and throw as many tantrums as they want. Those who want the truth merely have to LOOK.
Ashton
Outside of possessing a big mouth that likes to throw out baseless insults, what do you have going for you, Ashton?
All of the icons in the two rows of five icons below your "line" are either rectangular or ovoid, and their long axes are horizontal across the tie knot. The two icons above these two rows are also aligned with their long axes going across the tie knot and, despite your childish rantings, they are the same size as the icons below them PLUS they are precisely in line with the rows below them.
"Those with a disinformation agenda...."????? Boy oh boy, is the pot ever calling the kettle black!
-
Sorry, Sandy, the icons still measure longer, in a group of 5, lengthwise than they do crosswise, and the top of the tie knot is an impossibility, and you know it is.
I know no such thing.
If you would like to prove me wrong, by all means, do a physical demonstration using the sample photos of this tie.
Look... five icons, and no slip-down of the knot face. (You need to zoom way in.)

Is that the best you can do, Sandy? You still have not explained why the top two icons are rectangular and ovoid in the same direction as all of the other icons in the rows below them.
-
I don't have the means to zoom in on that photo. Why not post a zoomed in closeup of this photo for us?
-
Sorry, Sandy, the icons still measure longer, in a group of 5, lengthwise than they do crosswise, and the top of the tie knot is an impossibility, and you know it is.
If you would like to prove me wrong, by all means, do a physical demonstration using the sample photos of this tie.
-
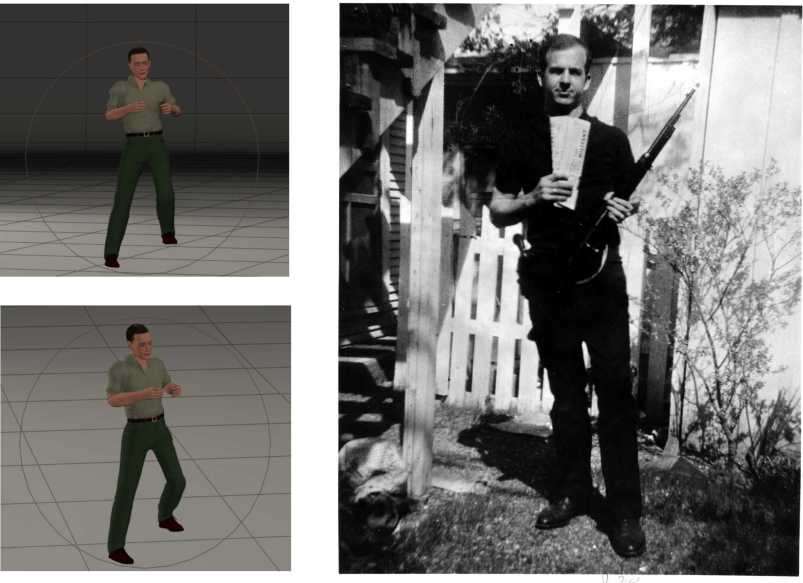
I am posting again the reconstruction of Prayer Man' s figure which also appeared in Prayer Man thread. The man's posture fits well with Prayer Man' in Darnell; I would like to show this part of work when complete, which entails realistic clothing and face, and fitting all the doorway occupants there.
I'm getting seasick studying the BYP tilted so far to the right. What's you flavour-of-the-week explanation today for everything tilting to the right, Andrej? C'mon, dazzle me with some scientific jargon.
Robert:
the comparison of Prayer Man's stance with that of the man in backyard photograph did not require any big science. The fact that the backyard picture is tilted by 1.9 degree does not prevent seeing that the hands are in very similar positions in both men, and that the right foot holds the body weight. I posted this one only to have all cases in which Oswald showed this peculiar habit on one place. As Paul wrote in a previous post, many people use to stand like this. So, it is not much, however, it aroused my interest, and it seems that quite a number of people are interested in the man's stance for various reasons. Let us see where it will lead.
Where did you get the figure of 1.9° Andrej? My simple plastic protractor tells me the gate and posts are leaning to the right by almost 10°.
You're not trying to minimize the problem now, are you?

JFK's "SHALLOW" BACK WOUND REVISITED (FOR THE UMPTEENTH TIME)
in JFK Assassination Debate
Posted
Hi Chris
I don't think you see what I mean. Look again at this photo:
In the photo at right, look at the left side of this section of tie, on the opposite side from the nick. See the tiny drops of blood? The main patch of them is directly opposite the nick, with a few more to our upper left and none of them below a line drawn straight across the tie from the nick.
If we turn this photo 180° and place the nick on the right, could this be the spray pattern from a bullet on a downward trajectory? Did the bullet carry this blood from the wound with it, leaving the largest deposit at the nick where it ran down the tie slightly? Did this coating of blood prevent the bullet from leaving metal deposits on the shirt material?