

Robert Prudhomme
-
Posts
4,105 -
Joined
-
Last visited
Content Type
Profiles
Forums
Events
Store
Posts posted by Robert Prudhomme
-
-
Thanks Bob.
I do recall the icon thing, where there was an extra row of icons along the top of the tie knot that were perfectly aligned with the others on the knot. But some believed that that extra row was actually from the layer of knotting behind the top layer, in a sloppily tied knot. And just sheer coincidence that all the icons were perfectly aligned.
I'm pretty sure that isn't what Tom is talking about.
Anyway thanks for answering. It tells me that I probably wasn't left out of the loop on something important. If what Tom is talking about is important, it's bound to come up again some time in the future
I often wish the discussion would wander back to the tie and the "slits" in the collar. I have this nagging feeling that there is some unfinished business here, and I'm literally itching to get at it again.
Good winter project?
-
Hi Sandy
Well, this is the great thing about theories; they explain a lot of things and everyone can own one. Experience has taught me to try to keep an open mind on this forum, as sometimes what seems crazy one day turns out to be entirely plausible the next day.
I'm sorry to see Tom leave the forum today, and I sincerely hope his absence is temporary. I was not trying to "get on his case" about the finer details of the upper airway; I merely saw a mistake he had made and was trying to point it out to him before it led him even further away from grasping the concept.
I like both you and Tom, and admire both of your abilities to grasp what to many are difficult concepts. I would prefer not to lose contact with either of you, and I hope we can go back to discussing things as we did before.
-
Lance
You have to broaden your thinking here a little. Your vision of a right wing conspiracy operating with clockwork like precision and achieving all of their goals is hardly representative of the coverup that followed.
The coverup that I have been studying all these years is one of the sloppiest messes conceivable, with more loose ends than can be counted. The only thing that has kept the coverup from being exposed is the vast majority of Americans are terrified of their having been a coup d'etat in America, and they will swallow any lie just as long as they don't have to look over the cliff.
Do you really think all the conspirators wanted was JFK dead? Do you really believe their only plan was the Lone Nut plan? What if LHO was only a bit player in the original plan, and no one thought anything of him being on the steps? What if the conspiracy was meant to be discovered, and used as a pretext for invading Cuba, or bombing Russia, and someone got cold feet at the last minute, and a Plan B had already been worked out, where LHO was the Lone Nut? What if no one really believed they needed Plan B until they actually did, explaining why tighter control was not placed on LHO?
-
While we were discussing the nick on the neck tie on Ashton Grey's thread last year, I believe we saw one of the slickest hustles in my recent memory perpetrated on us regarding the nick on the tie, and I'm still not certain who actually pulled it off. It all had to do with the little icons on JFK's tie, and the end result was many of us came away believing the nick was toward the back of the tie, and not on the left side. It's not very fresh in my mind, as I've been working on so many other things but. if someone was to re-start discussion about the "slits" and the nick in the tie, I'm sure it will all come back to me.
-
I found out what was wrong with my PM. As you and Tom guessed, I was up to 100% capacity. I deleted most of it and stand now at 18% capacity.
-
In regards to the speculative theory of a bullet striking the EOP, and continuing in whole or in part on to the vertebrae, and ultimately exiting the throat at a level between the 2nd and 3rd tracheal ring, I would like to add to the discussion.
First, humour me and have a look at this vintage Italian issue 6.5mm Carcano rifle cartridge:


I have explained this cartridge in previous posts but it is worth describing again. Pictured above is a 6.5mm Carcano M37 "Magistri" rifle cartridge, commonly referred to as a "frangible" bullet cartridge. While we nowadays associate frangible bullets with great stopping and killing power in game (and terrorists), frangible bullets were originally designed as "safe" bullets that could be fired in indoor 200 metre ranges. The bullet seen above will disintegrate into powder (except for the jacket) when it strikes something very hard, such as steel, stone or concrete. Because of this, the backstops in these indoor ranges, behind the targets, was simply a concrete wall.
As can be seen, this bullet's jacket is constructed of two pieces that join just below the nose of the bullet. The two sections overlap, although what actually holds them together is unknown to me. They could be soldered together. At the neck of the cartridge can be seen a very deep cannelure groove in the bullet jacket; so deep, in fact, I would venture to guess there was very little bullet jacket left at this point. I would imagine this deep cannelure groove contributed in some way to the easy disintegration of this bullet. Finally, it is possible to see, in the lower photo, that the inner core of the bullet is exposed in the nose of the jacket, possibly another feature contributing to rapid disintegration of this bullet.
Inside this bullet jacket, up in the nose, is a tiny metal pellet made from lead or "maillechort", and this is likely what is visible through the opening in the nose of the bullet jacket. As it is inside the bullet jacket it is, of course, smaller in diameter than 6.8 mm (actual diameter of a 6.5mm Carcano bullet). The jacket walls of a regular 6.5mm Carcano bullet are 1 mm thick, meaning the pellet in the frangible bullet could be 4.8 mm thick, but the jacket of a Carcano frangible bullet may not be quite as thick as a standard jacket, although the very deep cannelure groove seen above certainly suggests a 1 mm thick jacket wall.
Behind the lead/maillechort pellet, in the mid-section of the bullet jacket, is powdered lead. From the mid-section to the base of the bullet the remainder of the jacket is filled with sand. Naturally, this bullet did not weigh as much as a standard 162 grain Carcano bullet, and a reduced amount of gunpowder was loaded into these cartridges to give the frangible bullets a muzzle velocity equal to standard bullets.
There are several differences between these frangible range bullets and modern lethal frangible bullets used to kill game.
1. Instead of the nose of the bullet being exposed through the jacket, as in the M37, modern frangible bullets have a cavity opening in the nose referred to as a "hollow point". This allows the modern frangible bullet to penetrate bone, such as skull. Inside the body, liquid and semi-liquid matter (ie. brain) quickly fills this hollow point and begins to build a tremendous hydraulic pressure. This pressure exerts tremendous stress on the core of the frangible bullet and causes it to disintegrate; often within a couple of inches of the point of penetration, into a lethal cloud of metal dust that creates a wound cavity up to 4 inches in diameter.
2. The cores of modern frangible bullets are not made from powdered lead and sand. Rather, they are made from metal powder (not always lead) that has been compressed or sintered into a solid before insertion into the bullet jacket.
3. Not all frangible bullets, especially handgun bullets, are jacketed bullets meaning that, upon disintegration, nothing is left but powder. These bullets are so safe, it is actually possible to fire a 9 mm frangible bullet at concrete between one's feet without fear of injury from ricochet.
So, what is the point of my story? Well, it seems everyone has forgotten that no one at Parkland ever actually measured the throat wound, and it was described by Parkland staff as being from 3-8 mm in diameter.
I have no idea of the penetrating power of the M37 bullet in flesh or skull bone but, knowing that modern frangible hunting bullets also disintegrate when they impact steel, stone or concrete, I imagine the M37 had no trouble penetrating a skull bone or flesh. What would happen to it after that is anyone's guess.
However, as the lead/maillechort pellet occupies a good portion of the nose of this bullet, how difficult would it be to drill a small hollow point through the nose of this bullet into the pellet beneath, stopping just before the drill bit went into the powdered lead?
Now, with the modified nose, we might actually have something capable of doing some damage. If the M37 made it through the skull bone, it should perform in an identical fashion as any other hollow point frangible bullet; filling the nose with liquid until the hydraulic pressure caused complete disintegration of the bullet.
As I have said before, this would have been a crude adaptation, and the results might not even have been acceptable by today's standards, and a frangible bullet from 1963 might have had limited effect on a bony structure such as the vertebrae. If the bullet struck the base of JFK's skull, just below the EOP, and continued on until it struck the vertebrae in the region of C3/C4, it may very well be that most of this bullet broke up by hitting the vertebrae without doing a great deal of damage, leaving only the lead/maillechort pellet to carry on and exit the throat. As you should be able to see, this type of bulet is most effective when travelling through semi-liquid matter such as the brain or organs.

Counting the dorsals up from C7 vertebra, seen at the bottom of the neck in this diagram, C4 vertebra can be found right in the middle of the cervical stack of vertebrae. Now, take a straightedge and connect the EOP at the base of the back of the skull with the tracheal membrane between the 2nd and 3rd tracheal rings. C3 and C4 vertebrae will be on this line, just as Jerrol Custer suggested to the HSCA, when he told them the x-rays he recalled taking of JFK's neck showed "many fragments" in the vicinity of C3/C4.
As the Parkland doctors only reported one large wound in the back of JFK's head, presumably a wound of exit, it has sometimes puzzled me how a bullet could enter the base of the rear of the skull, just to the right of the EOP, and not either exit JFK's face or take part of his face off. Could Humes' report of a skull entry wound to the right of the EOP be just another "slight" modification of an actual wound, such as the back wound that became a neck wound? Could a frangible bullet have grazed and followed the base of the skull, only to break up when it struck the vertebrae at C3/C4?
-
Something we all should consider is that while we seem to be in agreement that the "slits" below the collar band were not made by a scalpel, they certainly had to be made by something, and I find it highly coincidental they are roughly in alignment with a nick in the tie that is adjacent to what appears to be a bloodstain.
-
Not only has it never been located with any degree of certainty, but what is traditionally referred to as the "nick" is much more likely to be the piece of cloth removed by the FBI Lab for testing. So where is this "nick" on the tie? There are a large number of white areas on the HIGHLY overexposed photo of the tie. Are they ALL nicks that penetrated the exterior cloth but not the lining?I do not believe it was ever adequately demonstrated where the nick in JFK's tie actually was when the tie was knotted
I presume this is not directed at me, but if so, I have made the above statement many times along with the fact that Carrico demonstrated using scissors and Head Nurse if the TR Audrey Bell STATED that she used scissors. And yes the fact that "Blunt-nosed" scissors are used to remove clothing has been stated here on this forum, long before you, me or Mr. Larsen mentioned this fact.I do not believe for one second the "slits" in the shirt collar were made with a scalpel, and that anyone could put that large of a slit in a shirt collar, with a scalpel, without cutting the tissue beneath it.
There is only one nick on the tie that has what appears to be a bloodstain directly adjacent to it. Such a coincidence. Perhaps one of the FBI technicians cut his finger while obtaining a sample of the tie material?
-
"...through his shirt collar..." Semantics?If the tracheal wound was between the 2nd and 3rd tracheal rings, and the top of JFK's shirt collar was against the bottom of his thyroid cartilage (Adam's apple), I really do not have a problem seeing a projectile either entering or exiting JFK's throat, passing through his shirt collar and nicking his tie on the way by.
There is no hole through his shirt collar. The slits are below it. Are you saying the slit is located at the same level as the throat wound?
The word "collar" is deceiving. You're right, the slits are just below the narrow collar band, but well above the actual bottom of the collar itself.
-
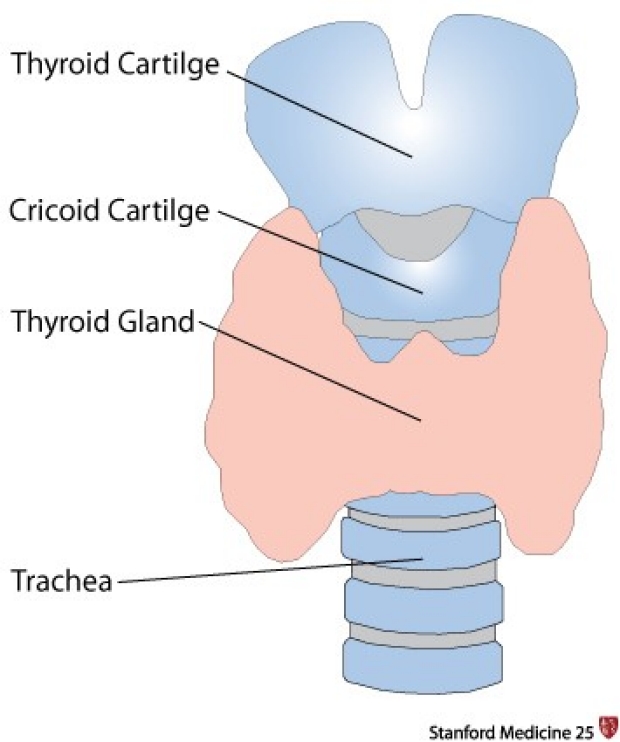
In actuality, Tom, this is not quite how it is. The term "tracheal cartilage" is actually another term for "tracheal ring". During the performance of a tracheotomy, the only thing necessary to retract, in order to access the tracheal rings, is the thyroid gland itself which, in many cases, overlies the upper trachea.[/font][/color]
Bob,
I don't believe I ever said the tracheal cartilage had to be retracted. I was speaking of the Adam's Apple and used the word "cartilage" referring to the cartilage immediately below the Adam's Apple. This is what has to be retracted. I pointed this out myself not too far back.
If I DID say the tracheal cartilage had to be retracted, please point it out to me and I'll correct the statement. I DO know the difference between the two.
""The first one you can feel - possibly. In most tracheostomy procedures the tracheal cartilage must be retracted to allow access to the upper tracheal rings. How can anyone feel them through this cartilage?"
The cartilage immediately below the thyroid cartilage (Adam's apple) is the cricoid cartilage, and it does not need to be retracted to perform a tracheotomy, as the tracheal rings start below the cricoid cartilage. Were you possibly thinking of the thyroid gland, which in many cases must be cut and retracted to expose the space between the 2nd and 3rd tracheal rings?
-
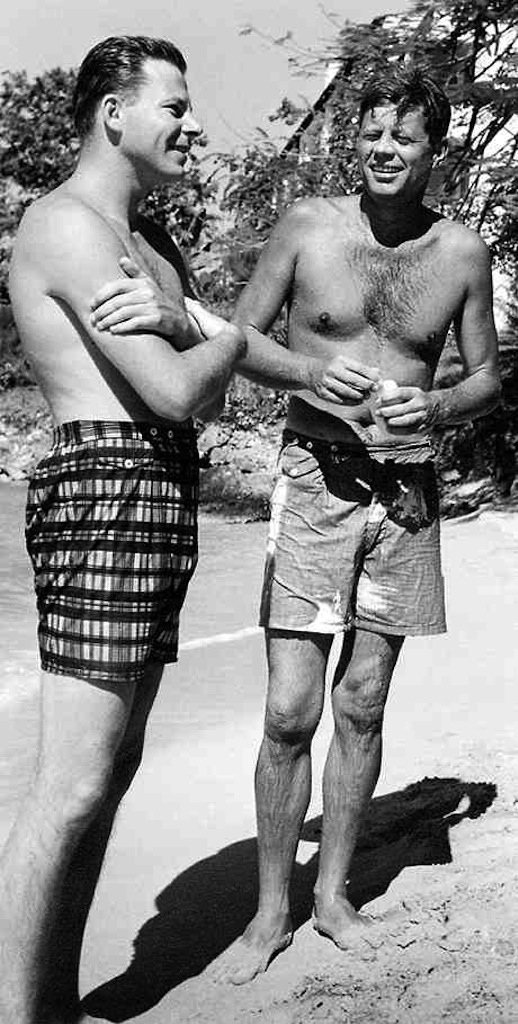
It is rather odd, isn't it. As I pointed out on your thread a few minutes ago, I thought at first it was an alteration of the chest x-ray, or the x-ray was taken from a perspective way above JFK's head. However, after looking at photos of a shirtless JFK, it appears his clavicles really did descend rather steeply, and that he did have a very low suprasternal notch. He must have been the very opposite of you!
I wonder if this anatomical oddity contributed to JFK's perpetual slouch; the one grossly exaggerated by Dale Myers in his Dealey Plaza cartoon.
-
If the tracheal wound was between the 2nd and 3rd tracheal rings, and the top of JFK's shirt collar was against the bottom of his thyroid cartilage (Adam's apple), I really do not have a problem seeing a projectile either entering or exiting JFK's throat, passing through his shirt collar and nicking his tie on the way by.
I do not believe it was ever adequately demonstrated where the nick in JFK's tie actually was when the tie was knotted, and I still believe it was on the anatomical left side of the knot, and was nicked by a projectile as it passed the outside of the tie knot. I also do not believe for one second the "slits" in the shirt collar were made with a scalpel, and that anyone could put that large of a slit in a shirt collar, with a scalpel, without cutting the tissue beneath it. As Sandy pointed out, blunt nosed scissors are the tool of choice in ER's for removing ties and clothing.
-
Tom Neal said:
"The first one you can feel - possibly. In most tracheostomy procedures the tracheal cartilage must be retracted to allow access to the upper tracheal rings. How can anyone feel them through this cartilage?
The trachea begins at the base of the Adam's apple. Therefore you are saying your Adam's Apple is located at or below the sternal notch. ???!!!
Where is your evidence that JFK's 2nd tracheal ring was substernal? The stare of death photo clearly depicts the trach incision AND the upper half of the circular bullet wound in the margin of the incision which is located at the 2nd tracheal ring. It is located quite close to the base of the Adam's Apple despite the EXTREME retraction of the lower margin of the incision. The substernal notch is also visible, many inches BELOW the wound.
JFK's 2nd tracheal ring is just below his Adam's Apple. Given the size of tracheal rings, the wound is at most 3/8" below his Adam's Apple - not the cartilage below it. The shirt slits are well below the collar button (supply your own measurements if you like) and therefore below the lower edge of the necktie knot.
The photo I have posted and referenced many times of JFK speaking at a podium on 11-22-1963 wearing the *SAME* shirt and tie that he was wearing when shot clearly shows his entire Adam's Apple and cartilage is above the top of his collar. Verify this with the skin folds in his neck, here, and in the SOD photo. The shirt slits however are below the knot in his tie.
My estimate is the shirt slits are 1 1/2" lower than the throat wound, and if true these slits could not have been created by any missile departing the throat wound."In actuality, Tom, this is not quite how it is. The term "tracheal cartilage" is actually another term for "tracheal ring". During the performance of a tracheotomy, the only thing necessary to retract, in order to access the tracheal rings, is the thyroid gland itself which, in many cases, overlies the upper trachea.
However, should the patient be suffering from a tension pneumothorax, and the trachea is shifted or deviated away from the affected lung, it is often necessary to sever strap muscles on the side of the trachea away from the affected lung, in order to access the trachea. This was the case with JFK, and explains why Perry severed the left strap muscles in order to perform a tracheotomy.
The trachea is separated from the larynx (contained within the thyroid cartilage or Adam's apple as seen above) by the cricoid cartilage. As the diagram above clearly shows, if JFK's tracheostomy site was between the 2nd and 3rd tracheal rings, it would have to be substantially more than 3/8" below his Adam's apple.
It is interesting to note another way to access the trachea surgically in an emergency, should the upper airway be blocked. At the junction of the thyroid and cricoid cartilages can be seen a notch where resides the "cricothyroid membrane". Below is a diagram portraying the procedure for intubating a patient via this membrane, the procedure being known as a "cricothyroidotomy".
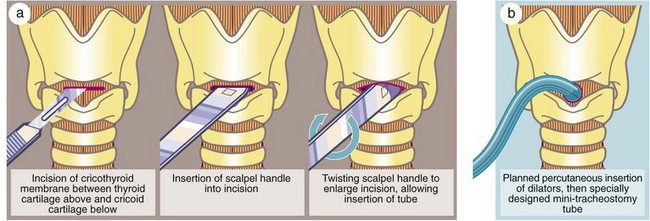
We had a patient we medevacced out to a larger centre who had an emergency cricothyroidotomy crudely performed on him by a doctor who just happened to be the first person at the scene of the MVA he had been involved in. The impact had broken/dislocated his lower jaw; forcing it upward and inward and completely sealing off his mouth and nose. Needless to say, he was a mess, and now is a quadriplegic.
Judging from the x-ray of JFK's chest, I would say he had an almost freakishly low suprasternal notch, and almost the entirety of his trachea must have been above it. Most people have clavicles that are more or less horizontal but JFK's descend downward at a severe angle. I thought at first it was either an alteration of the x-ray, or an x-ray taken from a perspective somewhere above the top of JFK's head, but perusal of photos of JFK without a shirt on indicate his clavicles may very well have been out of the ordinary.
-
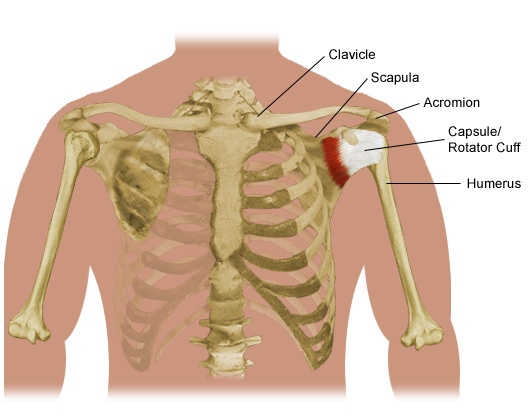
I would like to know from what perspective this x-ray was taken.

Do you see how the clavicles (collarbones) descend dramatically from the shoulders to the middle of the chest?
-
Assuming there were indeed tiny particles of metal bullet pieces in JFK's chest....
The reason we can't see them in the chest x-ray image is because that x-ray doesn't show a lot of things that it should. Like large sections of rib bones. Like the heart.
Compare JFK's x-ray with a normal chest x-ray:
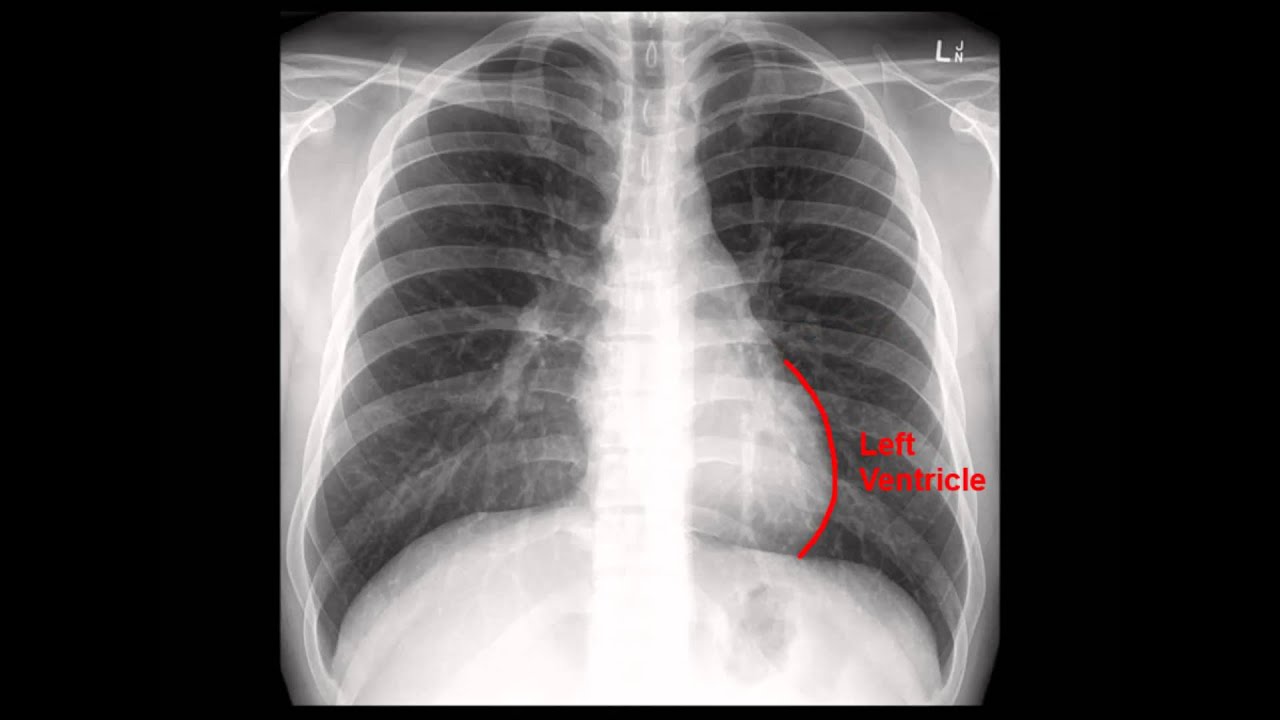
So why is it that we don't see much of the rib bones and heart in Kennedy's x-ray?
An over-exposure of x-rays will do this. Here is an overexposed chest x-ray:

However, it doesn't seem likely that Kennedy's x-ray was over-exposed given that it was taken with a weak, portable x-ray machine.
Another possibility is that the hard copy we see isn't a good copy. Maybe the bones and heart can be seen in the original x-ray.
Another possibility, of course, is that the extant x-ray was intentionally altered to hide something.
Or, the x-ray of JFK's chest was exposed after the heart and lungs were removed.
-
We also know that Humes reported, in the autopsy report (Appendix IX of the WC Report), that the tear in JFK's trachea was between the 3rd and 4th tracheal ring, just below the larynx.
According to Perry and Baxter the tracheal tear was at the 2nd tracheal ring and between the 2nd and 3rd. Apparently it wasn't quite parallel to the rings and cut across the trachea at a very slight angle. So what is Humes motive for moving the tear downward 3/8" or so?
The Parkland doctors, who unlike Humes, were qualified to analyze a gunshot wound, had reported this as an entrance wound. Lowering the wound:
- Assures the wound is comfortably below the top of the shirt collar and therefore not an entry wound.
- It is now closer to an alignment with the back wound that they raised to create a compatible entry-exit path for a shot from behind.
- It is now closer (but still too high) to align with the slits in the shirt located below the tie knot that allegedly were caused by an exiting bullet.
Good point, Tom. In fact, an excellent point. I was so busy looking at other aspects, I completely forgot Perry and Baxter placed the wound between the 2nd and 3rd tracheal rings. Just another one of Humes' "minor" disagreements with the doctors in Dallas, I guess? It would be interesting to know how many degrees equals a "very slight" angle, as the angle the Magic Bullet traversed the side of Connally's ribcage was anything but "very slight" at 23°.
If the wound was above the 3rd tracheal ring, and Carrico erroneously placed the endotracheal tube's inflatable cuff above this wound, there is no way Carrico could have placed the tip of the endotracheal tube into one of the two bronchi. Breath sounds, although diminished, should have been equal on both sides.
This proves a bullet went into JFK's right lung and caused a tension pneumothorax and, with this bullet arresting in JFK's right lung, another bullet (or two) had to be responsible for wounding Connally.
Too many bullets for one shooter = conspiracy
-
I have demonstrated several observations made by Drs. Carrico and Perry, in Trauma Room One of Parkland Memorial Hospital, regarding the state of JFK's respiratory system; in particular, his right lung. These observations point to very obvious clinical signs of a tension pneumothorax in JFK's right lung, a direct result of a bullet entering his upper right lung via the back entrance wound.
1. Dr. Carrico observed, while listening to JFK's chest with a stethoscope (following intubation and assisted breathing with a respirator), that breath sounds in JFK's chest were diminished, especially on the right side. While some WC apologists have argued this was a direct result of Carrico clumsily over-inserting the endotracheal tube into the left bronchus of JFK's left lung, and thus denying air to the right lung, there is simply too much evidence this was not the case.
The mere fact that breath sounds were diminished overall indicates the only mistake Carrico made was to under insert the endotracheal tube, leaving the inflatable cuff of the endotracheal tube above the tear in the trachea, and thus not making an airtight seal inside the trachea. This lack of a seal would allow positive pressure ventilation to escape the trachea, resulting in diminished breath sounds. Why would they be more diminished in the right lung? Quite simple. The right lung was collapsed, and building pressure in the tension pneumothorax (from the respirator) was preventing the lung from inflating.
We also know that Humes reported, in the autopsy report (Appendix IX of the WC Report), that the tear in JFK's trachea was between the 3rd and 4th tracheal ring, just below the larynx. Pictured below is a tracheostomy performed between the 3rd and 4th tracheal rings.

Note how close this is to the larynx (Adam's apple). Now look at this typical endotracheal tube, inserted into the trachea with its inflatable cuff just below the larynx.
https://upload.wikimedia.org/wikipedia/commons/5/5d/Endotracheal_tube_colored.png
Although difficult to see, in this diagram the inflatable cuff is just above where the tracheal tear would have been between JFK's 3rd and 4th tracheal rings. The tip of the endotracheal tube is even further above the point where the trachea divides into the two bronchi.
What all of this means is that the mere fact the cuff was not sealing JFK's trachea, allowing air to escape through the tracheal wound, makes a l.i.a.r. out of any WC apologist who tries to tell us Carrico over inserted the endotracheal tube. The tip of this device simply isn't long enough to allow this.
2. While surgically performing the tracheotomy on JFK, Dr. Perry observed several things. First, he observed the inflatable cuff of Carrico's endotracheal tube above the tracheal wound between the 3rd and 4th tracheal rings, thus confirming everything I stated in Point 1.
He next observed the trachea was deviated to JFK's left; so much so, it was necessary to sever the strap muscles on the left side of JFK's trachea, in order to gain access to the trachea. I have always found this sentence from Perry's Warren Commission testimony to be odd and somewhat contradictory, and I often wonder if it is not an example of "editing" done to Perry's WC testimony.
"At that point the trachea was noted to be deviated slightly to the left and I found it necessary to sever the exterior strap muscles on the other side to reach the trachea."
The use of the word "slightly" is what puzzles me. I have discussed this matter with several ER doctors, accustomed to dealing with tension pneumothoraces and performing tracheotomies, and they are quite unanimous in stating that a trachea deviated far enough to one side to require the severing of strap muscles to gain access to it can hardly be said to have a "slight" deviation. Was the word "slightly" added to Perry's testimony to downplay the possibility of a pneumothorax?
To be continued....
-
Hey Bob,
I tried to PM you with this, but I got a response that you are "unable to receive PMs." So...
Any chance I can get you to comment on my post:
http://educationforum.ipbhost.com/index.php?showtopic=22979&page=6#entry332273
TIA,
Tom
Hi Tom
Sorry I didn't answer your post. Things have been a bit hectic around here lately.
I find it quite odd that I am "unable to receive PM's". I don't recall ever trying to block anyone from sending me Private Messages.
"Thanks, Bob!
Question fer ya - your earlier comments re expert v. amateur and my thoughts as to WHY your 'scientific explanation' and mine on this topic are not accepted by many members. IMO, the instant the statements begin to sound like science or even worse, physics, many readers immediately reject any info that follows as pompous BS.
I have noticed that when I and others make a statement, a too frequent response is 'all you need is "common sense" to know that is not true.' Hopefully not true in Canada, but here in the USA a STRONG anti-science bias exists. IMO, this is due to the the repercussions of "Climate Change." Eliminating or severely reducing carbon emissions for example would reduce the typical "record profits" of oil companies.
Again IMO, this anti-science bias began in earnest with NASA's study which was immediately classified 'because it would panic the public with information that wasn't true.' This expanded quickly into a 'you can't trust scientists' attitude, and the opinion of experts possessing a higher education is superseded by alleged "common sense" that completely contradicts science. Again IMO, this bias is the result of a carefully orchestrated and politically supported plan.
To my knowledge this corporate/political campaign is not in effect in Canada. And at last the question I have been leading up to: Do you find the same anti-science bias there as in the USA?
Although I refuse to 'dumb down' the science to a point that it interferes with the necessary comprehension and can even create a false understanding, I don't supply any math, science or physics credentials for two reasons.
1. It has been my experience that when I counter 'common sense' opinions with science it is not accepted and is actually counter-productive to communicating.
2. Far too many people think you MUST be lying regarding credentials because 'simple common sense' proves you wrong.
None of the above applies to 'Science sites' where I spend MUCH more time than I do at this site.
Tom
PS If the 'Thread-Starter' believes this post is OT, LMK and I'll remove it. My personal opinion is that EVERY thread-starter has the right to make this decision him or herself."
Unfortunately, Tom, the same holds true in Canada as does in the USA. Climate change acceptance here is directly relative to how closely your sustenance is tied to the Oil Sands in Alberta.
-
It's a myth in your mind only, Bob. Humes said it was shallow and handled the body. The report and witnesses said that "the end of the opening could be felt with the finger."
Sorry Bob but I have to go with what they said vs. your fantasy myth, just like I'm going to go with Oswald himself saying he was innocent compared to your fantasy about a mystery agent getting a message to Oswald about keeping quiet all weekend.
That's fine if you want to go with the shallow wound report, Mike. But if you go with that, you need to explain how such a wound could have been created. A standard bullet shot from a rifle could not have made such a shallow wound because it is far too powerful. The wound also could not have been caused by a defective (lower speed) bullet shot from a rifle because it would have missed the target.
On the other hand, the shallow wound could have been caused by a small caliber subsonic (i.e. low speed) bullet, such as those reviewed in this article. In this review, a variety of .22 caliber subsonic bullets were shot into a gelatin blocks. (Ballistic gelatin is designed to simulate muscle tissue, and is used to demonstrate penetration depth of bullets.) Here are the results of the test:

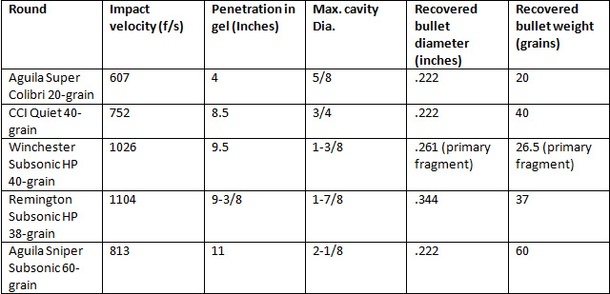
The Aguila Super Colibri bullet, having a velocity of only 607 fps, penetrated the gel by only four inches. It is conceivable that this bullet, or one like it, could have made the shallow wound described by Humes. It is one of the three bullet to have remained in like-new condition upon recovery:

Above: The recovered .22 LR subsonic bullets. From left are the Aguila Super Colibri, CCI Quiet, Winchester Subsonic HP, Remington Subsonic HP, and Aguila Sniper Subsonic.
The Aguila Super Colibri is the one on the left. Notice how much less massive this bullet is than a typical .22 caliber bullet. (The table shows that its mass is 20 grains, compared to the others which range from 38 to 60 grains.) This no doubt explains why its penetration was so much less than the other bullets.
So we learn from this test that a very slow 600 fps, lightweight, small caliber bullet is capable of causing a shallow wound. But if such a bullet were used on JFK, a number of complications need explaining.
First, it must be admitted that the bullet was either lost or hidden for some reason. CE399 was certainly not it.
Second, the effective range of this bullet is only 100 feet or so. Beyond that it will likely miss the target. Where could this bullet have been shot from?
Third, it must be explained why an assassin would choose such a wimpy bullet to kill the President. Perhaps if it carried a poison?
BTW, in order to make this bullet that penetrates only 4 inches into flesh, the manufacturer had to remove ALL the gun powder from the shell. The only thing that powers this bullet is the primer!
Also, Sandy, the rifle would have to be sighted in for a bullet travelling 600 fps. As Michael would say, this would require quite a bit of "loft" just to get the bullet to its target.
The problem with bullets that are slow moving and have high trajectories or "lofts" is that they are not what we would call "flat shooting".
For example, the 6.5mm Carcano, shooting a 162 grain bullet at a muzzle velocity of 2200 fps, is actually quite flat shooting at ranges within 100-200 yards. If sighted in at 100 yards, the high point of this bullets trajectory, at 50 yards, is only .72 inches above the line of sight.
OTOH, the 20 grain .22 LR bullet, travelling at only 600 fps, has a much higher trajectory. If sighted in and fired at 100 yards, the high point of its trajectory, at 50 yards, works out to 13.29 inches above the line of sight. Hitting a target at anything but its sighted in range requires aiming much higher or lower than the target.
Put another way, if this .22 LR bullet travelling with an initial velocity of 600 fps will drop 53.26 inches in 100 yards.
As you say, Sandy, who in their right mind would attempt to kill the President with something so ridiculous, even if it was poison tipped?
P.S.
I was rather impressed to learn this 20 grain .22 LR bullet had a muzzle velocity of 600 fps, with no gunpowder and only the rimfire primer as a propellant.
-
Robert,
There are two issues that bother me. First is the damage to the Lung. The second is the damage to the spine.
Xray taken before the autopsy:-
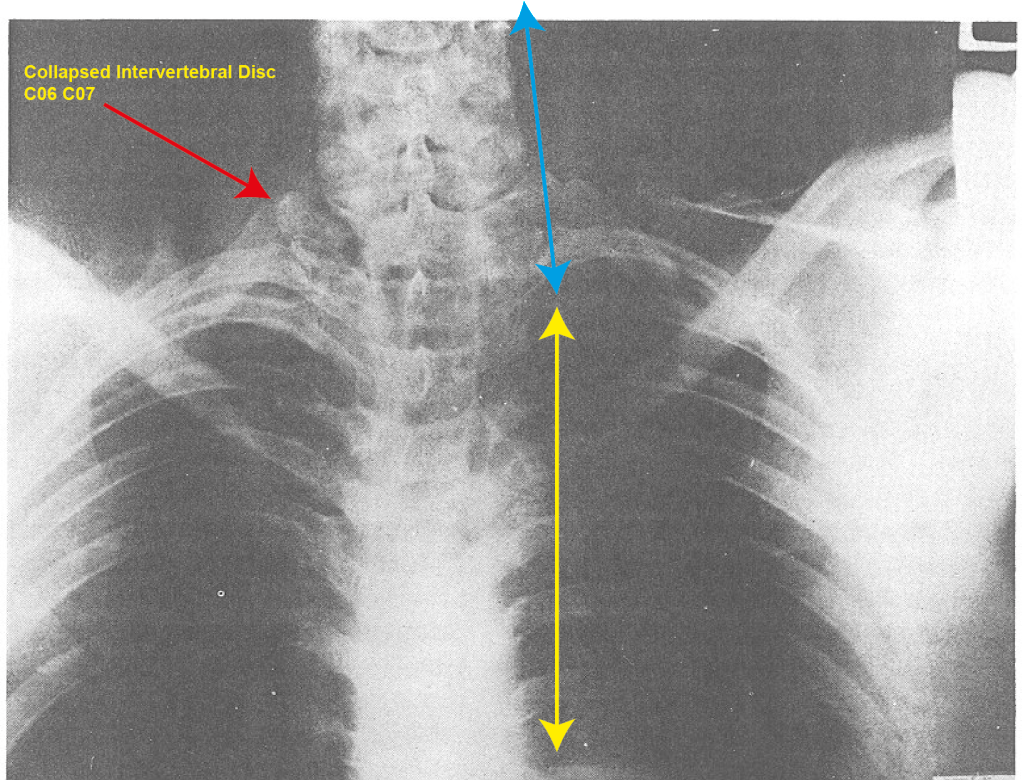 I have added lines to show the clear slope of the neck. Clearly there has been damage to the spine. This image and close up taken around 8:30pm and after the organs have been removed makes clear something has been damaged. the position of the damage is around C7.
I have added lines to show the clear slope of the neck. Clearly there has been damage to the spine. This image and close up taken around 8:30pm and after the organs have been removed makes clear something has been damaged. the position of the damage is around C7.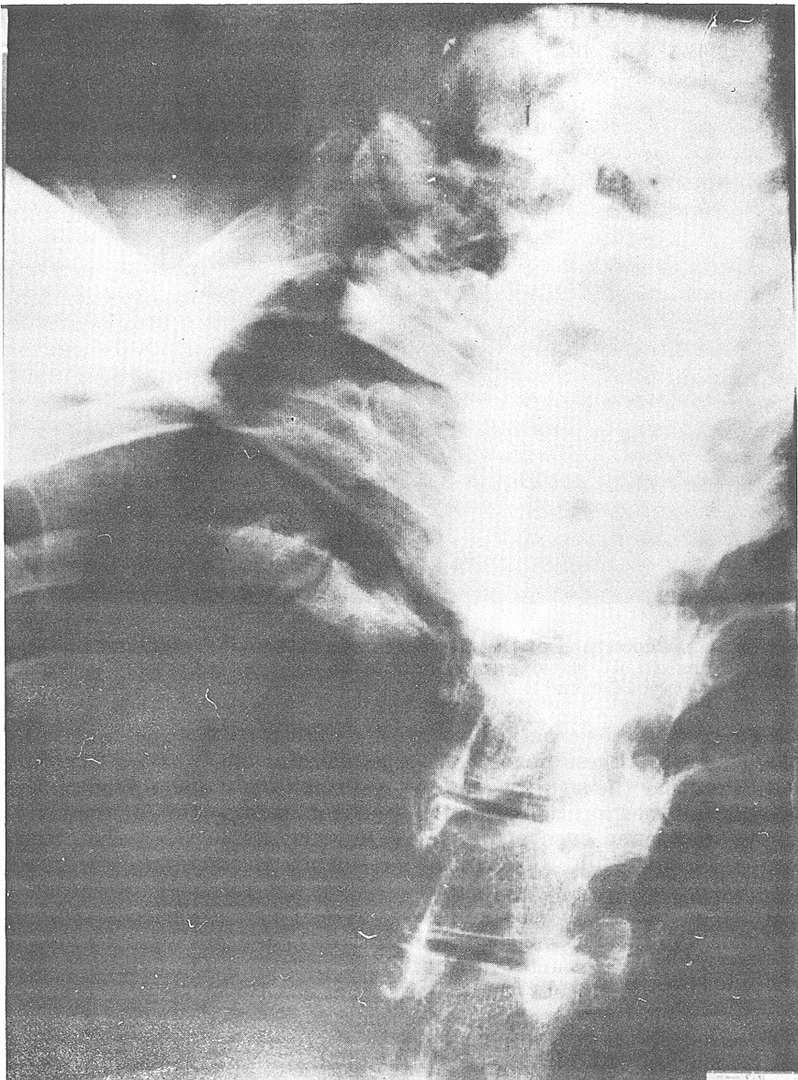 The question is this. Did a bullet enter through the throat hit and damage the spine around C7 and land on the lung thereby creating the damage to the lung? Something caused that damage to the spine. The kind of damage needs explaining. And the only explanation I have is that the spine was damaged by a bullet entering through the throat. I wonder whether this same bullet did not also cause the damage to the lung.
The question is this. Did a bullet enter through the throat hit and damage the spine around C7 and land on the lung thereby creating the damage to the lung? Something caused that damage to the spine. The kind of damage needs explaining. And the only explanation I have is that the spine was damaged by a bullet entering through the throat. I wonder whether this same bullet did not also cause the damage to the lung.Just out of curiosity, James, is it your opinion there is serious damage at C7, or have you had these x-rays examined by a radiologist?
-
In the conversations I have had with Gary Murr, he was quite adamant that the 6.5mm Carcano ammunition, found in Oswald's rifle, was manufactured in 1954 by the Western Cartridge Company of the USA, despite my protestations that this ammo was made by the WCC prior to 1944.
Either way, this makes the WCC 6.5mm ammo either nine or nineteen years old in 1963; hardly what could be called "aged" ammunition, if the ammo was well manufactured and the cartridges were well sealed.
Regardless, though, of claims of cartridge deterioration, it must be understood the degree to which a cartridge, normally capable of propelling a bullet at 2200 fps, would have to deteriorate to propel a bullet at a low enough velocity (<300 fps) in order to make only a shallow flesh wound at a range of 50 yards. This is an astonishingly low velocity for this rifle, and a bullet leaving this rifle at this velocity would likely be so unstable it would be tumbling end over end on its way to JFK's back, and would make an oblong entrance wound in JFK's back instead of a round wound. Tumbling bullets are also more prone to air drag, and if this bullet were tumbling it would be slowed down much quicker.
As I have been pointing out in another thread, a shooter would not be expecting such a defective cartridge, and would be aiming in a normal fashion. If he did so, the bullet would land far short of the target, as this graph below illustrates:

Trajectories of a projectile with air drag and varying initial velocities
-
Might surprise you but, JFK might have forever been remembered as the man who brought us the Viet Nam War. I have analyzed the matter quite carefully, and I am far from convinced, as many are, that JFK intended there to be a total troop withdrawal from Southeast Asia.
-
Humes also said there was no large gaping wound in the back of JFK's head. Humes also agreed with Specter that the bullet entered the back of JFK's neck and exited his throat.
Does that make these things true as well?
-
BTW, Michael, not only have I likely forgotten more about the JFK assassination than you will ever know, I also am able to understand, technically and medically, why some things in this case are possible and others are not; something I am beginning to notice you are totally incapable of.


{kind=link}
PRAYER PERSON - PRAYER MAN OR PRAYER WOMAN? RESEARCH THREAD
in JFK Research
Posted · Edited by Robert Prudhomme
And welcome back to you Thomas.
Use your imagination. Try to think how many patsies were set up for that day (or several days) with rifles and backyard photos, or other bits of incriminating "evidence". The problem with all of us is we all tend to think in small terms, and none of us have the ability to grasp what we are up against.
No idea what LHO's role might have been. Lookout, perhaps?
Not everyone can predict the future. This was 1963 and no one had cell phones. Maybe the conspirators didn't really expect two films to show up with one of their boys in them.