

Robert Prudhomme
-
Posts
4,105 -
Joined
-
Last visited
Content Type
Profiles
Forums
Events
Store
Posts posted by Robert Prudhomme
-
-
Okay so, what did Drs. Carrico and Perry say about their attempts to resuscitate JFK, and how does it relate to my post explaining pneumothoraces of the lung.
The thing that must be kept paramount in our minds about ER doctors and nurses is they are typically presented with patients who must have basic life support established prior to a full and in depth examination of their wounds or ailments is performed. In other words, the patients are often dying (or dead) and there is often mere seconds to read the physical signs of a respiratory condition before attempting to rectify that condition.
In the practice of emergency First Aid, we go with the simple principle of ABC.
Airway
Breathing
Circulation
In JFK's case, all three of these were inadequate, requiring a critical intervention on the part of the doctors to correct them.
Dr. Carrico observed that JFK was "cyanotic". This means that he was, in Dr. Carrico's words, "...ashen, bluish, grey, cyanotic..." from not getting any oxygen to the cells of his body. The first thing Carrico did was to establish an airway and a means of getting positive pressure ventilation into JFK's lungs, utilizing a respirator. The device he chose for this was an "endotracheal tube", pictured below:

And inserted:

As seen, there is an inflatable cuff just up from the inserted tip of the tube. Once in place, this cuff is filled with air from a syringe via the tube marked "B".Once inflated, it makes an airtight seal against the inside of the trachea, and the respirator is able to pass air to and from the lungs. Note that the cuff is below the vocal cords in the larynx, yet the tip of the tube is above the point where the trachea branches into the two bronchi. The most important thing to remember when doing this procedure is to keep the tip of the e. tube above the point where the trachea divides into bronchi.
Some WCR apologists have long debated that Carrico made a mistake inserting the e. tube, and that he accidentally over inserted the e. tube into JFK's left bronchus, thus isolating JFK's right lung. This is simply not true, and it can be proven to be not true, as I will demonstrate shortly. The reason they have argued for over insertion of the e. tube is they are attempting to cover up the most important piece of information Carrico related to the WC. Here it is:
"Mr. SPECTER - You had begun to describe some of the action taken in order to endeavor to revive the President. Will you continue with that description, please?
Dr. CARRICO - I believe we were to where the endotracheal tube had been inserted. After this, the President--his respirations were assisted by the Bennett machine. We again listened to .his chest to attempt to evaluate the respirations. Breath sounds were diminished, especially on the right, despite the fact that the endotracheal tube was in place and the cuff inflated, there continued to be some leakage around the tracheal wound."
So, let's see now, Carrico listened to JFK's chest and observed "Breath sounds were diminished, especially on the right....". If there were no damage to JFK's right lung, what would be the only thing that would make the breath sounds on the right more diminished than on the left? The one and only reason would be the tip of the e. tube would have to be over inserted into the left brochus, cutting off the air supply to the right lung. However, this was impossible, and I will tell you why.
1. The left bronchus is smaller than the right bronchus. Not only that, it is almost a straight shot from the trachea into the right bronchus, while the left bronchus takes off from the trachea at a much sharper angle. As any doctor who inserts e. tubes on a regular basis will tell ou, it is almost impossible to accidentally over insert an e. tube into the left bronchus, but very easy to over insert the e. tube into the right bronchus.
2. Carrico used a laryngoscope to assist in placing the e. tube where he wanted it, and knew precisely where it was once it was inserted.

Laryngoscope
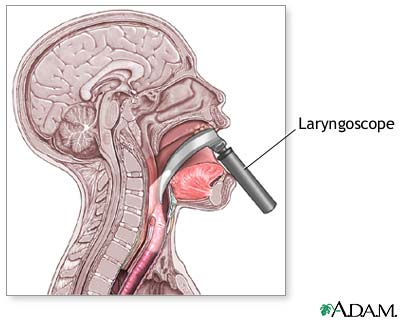
Laryngoscope in use, providing view of trachea.
"No pulse was present, and at that time, because of the inadequate respirations and the apparent airway injury, a cuffed endotracheal tube was introduced, employing a larynzo scope. Through the larynzo scope there seemed to be some hematoma around the larynx and immediately below the larynx was seen the ragged tracheal injury. The endotracheal tube was inserted past this injury, the cuff inflated, and the tube was connected to a respirator to assist the inadequate respiration."
3. The positive pressure ventilation from the respirator was leaking out of the throat wound.
"...despite the fact that the endotracheal tube was in place and the cuff inflated, there continued to be some leakage around the tracheal wound."
In other words, as careful as Carrico was placing the e. tube, he did make a slight mistake. Before the cuff on the e. tube was inflated, sealing the cuff against the trachea, the cuff had to have moved slightly upward; pacing the cuff just above the tracheal wound and allowing respirator air to escape through the tracheal wound and out the throat wound. As can be seen, the distance from the cuff to the tip of the e. tube is so small, the tip could not have been anywhere near the bronchi.
So, why were breath sounds diminished in the right lung, in comparison to the left lung? The only thing that could produce this finding is a tension pneumothorax in the right lung, likely accompanied by a hemothorax (collection of blood in the pleural cavity) in the right lung. I will explain how it likely developed.
The bullet enters JFK's right lung and breaks up, piercing both pleural linings and rupturing several important blood vessels. JFK would now have an open pneumothorax (sucking chest wound) although it is not unheard of for such a small wound to seal itself, elevating the condition to tension pneumothorax.
JFK is laid on his back on a table in Trauma Room One, allowing pooling blood in his lung and the pressure from the table on his back to completely seal the entrance wound, thus guaranteeing a tension pneumothorax. Carrico intubates JFK and connects the e. tube to a respirator which now forces air (oxygen) into JFK's lungs at greater than atmospheric pressure. Air enters JFK's right lung where it passes into the pleural cavity and is trapped. With each breath, the volume of air increases, until a point is reached where virtually no new air will pass into JFK's right lung.
Carrico listens to JFK's chest with a stethoscope and hears greatly diminished breath sounds in JFK's right lung.
Surprise, surprise......
Next up, What did Perry say to the WC?
-
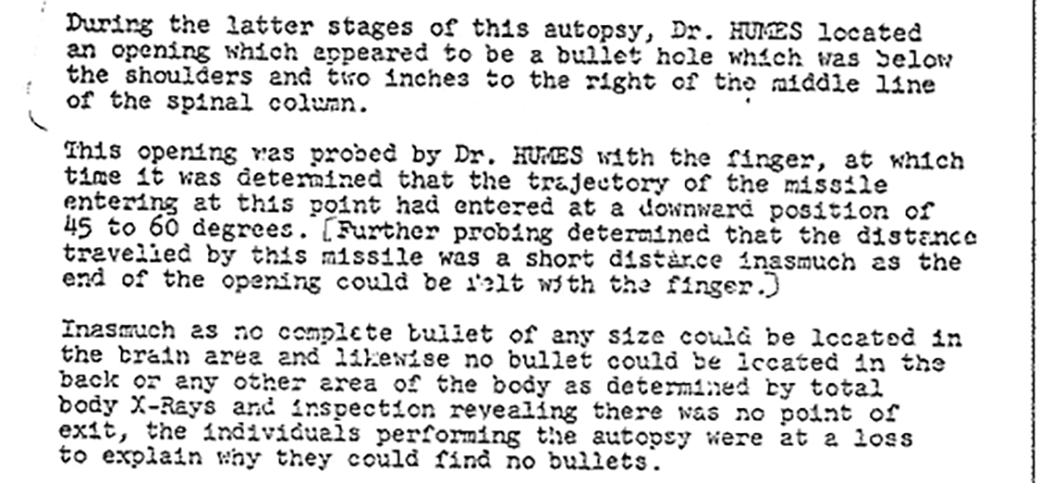
James G. seems to have a good point regarding the Sibert/O'Neil report where they say Humes probed the wound with his finger and said it was shallow. I say that because I've never seen anything that puts doubt on their report.
On the other hand, Humes making that declaration is inconsistent with what happened at the autopsy as reported by Lt. Lipsey. He said that the doctors spent half the autopsy looking for the bullet that had entered the back wound. Well, if Humes noted that the wound was shallow, why was he then looking for the bullet as though the wound weren't shallow?
Is it possible that Humes FIRST did the searching for the bullet, and only after he couldn't find it he pretended to probe the wound so that he could say, ah-hah! we couldn't find the bullet inside the body because, alas, it is a shallow wound!
In fact, wasn't Humes informed during the autopsy that there was a bullet on the stretcher at Parkland? If so, then that could explain why he went from searching for a bullet to later saying it was a shallow wound and that the bullet had fallen out.
In other words, the bullet on the stretcher was planted in order to explain away the bullet Humes couldn't find. And Humes was playing along with the scheme when he did the bullet hole probing with his finger.
Exactly, Sandy! I was beginning to think I was the only person who got this LOL!
Yes, why dissect the chest and abdomen organs looking for a bullet (or fragments) if you probed the wound and found it to terminate an inch in? Better yet, Humes claimed to have looked inside the empty chest cavity and to have seen NO bullet hole in the outer pleural lining. This would also tend to eliminate the possibility of a bullet entering the throat and ranging downward, as Humes claimed the lungs and heart were undamaged, save for slight bruising in the Upper Right Lung.
If the lungs and heart were in pristine condition, this would also mean there would be no bloody wound track ranging down toward the abdomen through these organs. Why look for a bullet in the abdominal organs then?
-
The only problem with shooting JFK in the back, as opposed to shooting him in the head, is being able to tell whether or not you had killed him. He might have been only mildly wounded at z224, but there is no doubt as to what occurred at z313,
Of course, as you surmise, it would require something other than a full metal jacket bullet to do any real damage in a chest shot, as the FMJ bullet would likely go straight through JFK's chest without doing much damage on the way through.
Okay, so it's possible that the assassin was intentionally aiming at the back. And if so, he likely chose that target because it was a guaranteed hit. A frangible bullet was chosen so that maximal damage would be done.
This way, if the later, more difficult head shots missed, Kennedy still had a pretty high probability of dying.
(Just my hypothesis.)
EDIT: One problem with this hypothesis, it seems, is that it risked Kennedy falling down before the head shots could take place. Making the head shots impossible.
This is assuming, of course, that a head shot would even be necessary.
The shot in JFK's back was followed by the head shot(s) within six seconds. How would we know, should the head shot(s) have missed altogether, that JFK would not have expired within the next two or three minutes from massive bleeding into his right lung?
-
Robert,
“How close were Sibert and O'Neil to JFK when Humes supposedly probed the back wound with his finger? Were they standing right beside Humes, looking down, or were they in the gallery many feet away? Where does it actually state Humes used his pinkie finger?” Robert Prudhomme Post 11
Sorry I have not been able to get back to this thread for a few days, I have been very busy.
Siberia and O'Neil were inside the mortuary. They were not in the Gallery. They were under instruction not to leave until the autopsy was complete and report everything they saw and heard. Whether they were watching over Humes shoulder or not I do not know, but you will be aware that the mortuary was a small room. So to get back to the critical point - unless you doubt their veracity - their report makes clear that they did see Humes prod the wound with his pinkie and explain to all in the room that it was a shallow wound.
That suggests any thought that - whatever caused this wound - was able to pass intthe rib cage let alone into the lung is simply not possible. Whatever this wound was it was not a deep or penetrating wound.
James.
If I was a respected physician and I stuck the tip of my finger into an entrance wound and told you I could feel the bottom of the wound, would you have any reason to doubt me, James? Humes is the same doctor who reported only shallow incisions in JFK's chest, when it seems to be universally believed at Parkland that chest tubes were not only fully inserted, they were also connected to drainage. Someone was lying in that matter, too, and who had the greater motive?
As for doubting their veracity, I'm sorry but, most of the problems with this case stem from a total lack of veracity on the part of the FBI when it came to supplying evidence.
I'm sorry to disagree with you James but, I simply cannot accept that Humes was able to probe a 1/4 inch diameter entrance wound with a finger that was likely almost three times that diameter at the first knuckle, and increasing in diameter as it went up the finger. As I stated earlier, I have attempted this unsuccessfully on entrance wounds in deer made by larger calibre rifles.
-
The only problem with shooting JFK in the back, as opposed to shooting him in the head, is being able to tell whether or not you had killed him. He might have been only mildly wounded at z224, but there is no doubt as to what occurred at z313,
Of course, as you surmise, it would require something other than a full metal jacket bullet to do any real damage in a chest shot, as the FMJ bullet would likely go straight through JFK's chest without doing much damage on the way through.
-
Hi Sandy
It is taking me a long time to write a post that ties together my earlier explanations of pneumothoraces with the testimonies of Drs. Carrico and Perry. It is a very complex topic and I am finding it difficult to present but I will keep plodding on.
In response to your question, a lung shot is one of the most popular ways of shooting a deer, and also one of the most effective. The reason for this is that the simple piercing of the pleural cavity with a bullet is enough to create an open pneumothorax (sucking chest wound) that will severely impair the breathing process. Rupturing the lung will also prevent that lung from properly inflating, and further impair the breathing process. The lungs also contain the pulmonary arteries and veins, and rupturing these can quickly cause an animal to bleed out into the chest cavity. Lastly, there is the heart, and a shot through the heart will bring almost instantaneous death.
On long difficult shots, many hunters will aim at the chest, just behind the front legs, simply because it offers such a large and easy to hit target. I have seen a deer shot through the lower portion of the lungs with a soft point .243 bullet take four steps and fall down dead.
Ribs are quite fragile, and offer little protection from a bullet to the lungs beneath them. If anything, striking a rib will only increase the severity of the wound, as was the case with John Connally, where the shattered shards of his 5th rib became "secondary missiles" that went on to create large amounts of damage to his right lung; despite the fact the bullet never entered John Connally's right lung.
As strange as it may seem, the wound in JFK's back could have easily been fatal by itself, without the head wound.
-
Also, the only x-rays that somehow ended up with "dirt" on them that "look like metal, but are only dirt" are the x-rays of the chest.
How coincidental.
I don't think I ever dug into the other x-rays, but if I did I don't recall any artifacts due to dirt on the non-missing x-rays. Have you verified this? If so, that is Mighty Interesting!
Of course I can't remember who said it, but it was published in Doug Horne's 5 volume set, and the comment by one of the techs who worked there 11-22-1962 was that he 'couldn't imagine' how dirt could get into a film cassette, and it that ever happened someone(s) would have caught pure holy for it, but has no memory of that. Apparently Humes et al thought it happened every day because they never challenged the fact that it was dirt.
Although as a former member I recall seeing MANY "dirty films" in the USN, I can't say one way or another about "dirty film."
It is just possible that Humes had no idea what he was actually dealing with, and the possibility of a bullet disintegrating into dust after going through nothing but soft tissue simply was a non-starter with him. He may have truly thought (with a likely bit of suggestion from an unnamed source) that he was looking at dirt on the chest x-rays that just happened to look like metal.
-
Also, the only x-rays that somehow ended up with "dirt" on them that "look like metal, but are only dirt" are the x-rays of the chest.
How coincidental.
-
*sigh*
I was defending the fact that you were right to declare an "OT."
But you're right, it's time to let that go, and move on with the thread...
Thank you.

-
Bob,
What do you think of the conflict between Parkland and Bethesda regarding the insertion of chest tubes? Parkland says they inserted chest tubes and set up sealed drainage, Bethesda says the two incisions only penetrated flesh and did not violate the pleura.
Due to Bethesda's many exposed lies regarding JFK's body, I would expect Parkland to be telling the truth. More or less speculation, but IMO Humes was ordered to declare the pleura as unviolated. I believe that the right lung was peppered with the bits of a bullet that was designed to fragment. Only low resolution x-rays were taken of the lung and they were looking for a bullet or large bullet fragments, but the 'dust-like' constellation of fragments present in the skull x-rays would have told them to look for tiny fragments as well. They DID remove the right lung which could have been carried upstairs to a high-resolution x-ray but chose not to do so. Additionally, IIRC a notation about the lung x-ray states that many artifacts that 'look like metal' are 'actually dirt.' Kind of a stretch for me to believe a military hospital allowed that much dirt into a film cassette, and that they didn't redo these xrays until they found some 'clean' film. I mean this was an x-ray of their Commander-in-Chief who had been murdered.
There is a definite contradiction between Parkland and Bethesda on the matter of chest tubes. It is almost ludicrous to read Humes' description of the "shallow" incisions that did not fully penetrate into the pleural cavity, when one considers the difference between a shallow incision and full penetration only amounts to a few millimeters.
The hundreds of dust like particles of metal seen in the x-ray of the skull is a dead giveaway as well. Lead bullets will break up into fragments but, seldom will they turn to dust. Lead is malleable, not brittle. The only lead bullet that will turn to dust is one that was made from compressed lead dust to begin with; ie. a frangible bullet. This is assuming the particles in the x-ray actually were lead. I don't believe this was actually ever proven.
-
-
I exceeded the limit of diagrams in my previous post. Here is the diagram of the cross section of the right lung hilum:

-
Well, here goes nothing.
I am going to attempt to show, using the medical reports and WC testimonies of the surgeons attending to JFK in Trauma Room One, that JFK was suffering from a respiratory emergency known as a "tension pneumothorax". It likely began as an "open pneumothorax (sucking chest wound)" but, once JFK was laid on his back on a gurney in Trauma Room One, effectively sealing his back wound, and positive pressure ventilation was applied, the open pneumothorax likely developed into a tension pneumothorax rather quickly.
So, what is a pneumothorax? To explain this, it is necessary to understand the basics of how the lungs draw air in and expel it roughly 16-24 times per minute for us. The basic physical description of a lung is an airtight rubber bag inside of a plastic bag that is also sealed. When we increase the volume of this plastic bag, by moving our diaphragm muscle downward, we create a partial vacuum outside of the rubber bag (lung). Naturally, as air pressure equalizes, air rushes in through our nose and mouth, filling the rubber bag (lung) and occupying the vacuum in the plastic bag (pleural cavity).Exhalation is just the opposite; the diaphragm muscle moves upward, decreasing the volume in the pleural cavity and raising the air pressure in the pleural cavity. to compensate, and equalize the air pressure, air rushes out of the lung and through the nose and mouth.
If you look at this diagram, you will see that each lung has its own pleural lining that envelops each lung individually like a sack.
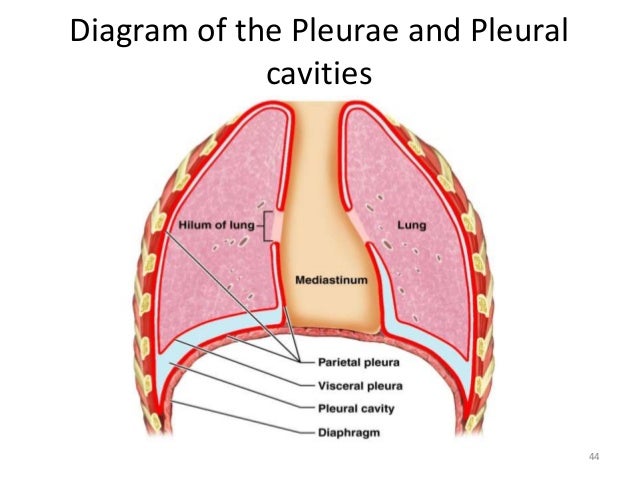
When the diaphragm (labelled) moves downward, the pleural cavity (labelled) increases in volume. It is important to note that each lung is enveloped in its own "visceral pleura" and those are contained in two separate "parietal pleura". The lungs are separated by an area called the "mediastinum", which contains the heart and major blood vessels leading to and from the heart.
The reason I am making a point of demonstrating the two lungs are each in their own separate sack is because it is possible to have an injury in one lung that shows no signs, initially, in the other lung.
An "open pneumothorax" (sucking chest wound) is a puncture or tear in the parietal (outer) pleural lining that allows outside air access to the pleural cavity between the two pleura. If such a tear or puncture occurs, outside air will enter through this opening when the diaphragm moves downward; equalizing air pressure with the outside air. Of course, if air enters through this opening, the lung does not inflate in the normal fashion, and the patient is said to have a "collapsed lung". This is a very serious respiratory condition and, unless addressed, can kill the patient within a short time.
The quickest method of dealing with an open pneumothorax, on scene, is simply to seal the opening with a rubber gloved hand, until an occlusive dressing can be fashioned. Once sealed, the lung, if not compromised also, should inflate in a normal fashion.
The occlusive dressing for sealing an open pneumothorax must be designed carefully, and the dressing NOT to be applied is one that is sealed all around. Below is a diagram of the traditional three sided dressing to be used in this situation:
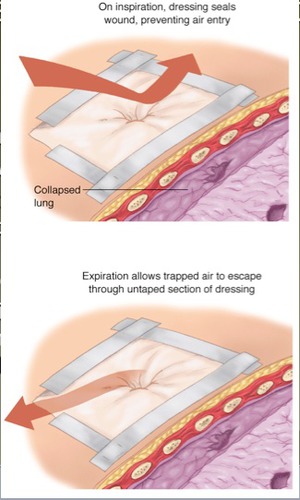
Note that one corner of the plastic is not taped down. As the diagram explains, upon inhalation, the plastic gets sucked against the skin and seals the hole in the chest, allowing the lung to fill. On exhalation, the plastic moves away from the skin, and air in the pleural cavity escapes through the wound and passes out the gap in the tape.
Where is the air in the pleural cavity coming from? The same mechanism of injury that put a hole in the parietal (outer) pleural lining often will put a hole in the visceral pleural lining and the lung itself. When this compromised lung inflates, a portion of the air in this lung will escape into the pleural cavity outside the lung. On exhalation, the damaged part of the lung may flatten somewhat; acting as a one-way valve and trapping the air in the pleural cavity. With each breath, this trapped volume of air will grow, especially if the patient is on positive pressure ventilation (ie. respirator machine) that is forcing air into his lungs at greater than atmospheric pressure. The reason for the open edge in the three sided dressing becomes obvious.
If the trapped air is not released, the ensuing respiratory condition is known as a "tension pneumothorax" and it is even more dangerous than the open pneumothorax. As the air pressure builds in the pleural cavity, the affected lung is able to inflate less and less with each breath, until the lung is no longer able to inflate at all. As the condition progresses, pressure begins to be exerted on the mediastinum, preventing normal beating of the heart found there and normal return of blood to the heart through the major veins (superior and inferior vena cava). It will eventually get so bad that the other lung will begin to have difficulty inflating and, at this point, death is imminent.
The classic cause of a tension pneumothorax, just as an example, is a broken rib (or two or three) caused by a blow to the chest from a blunt object. While there is often no opening to the pleural cavity from the outside, the sharp end of a broken rib will often tear the visceral pleural lining and tear a hole in the lung itself. As demonstrated above, this will fill the pleural cavity with each breath and lead to a tension pneumothorax.
The accepted method of treating a tension pneumothorax is the insertion of a large bore needle or "tube" in the intercostal space between the 2nd and 3rd ribs, at about the "midclavicular line".

The mere insertion of this tube will provide instantaneous relief to a patient, as the impairment is removed from his heart and lung. In a hospital setting, this tube will now be connected to what is called "underwater sealed drainage". Think of a device similar to a hookah water pipe that will allow air and blood to escape through the chest tube, but not return. In the field, we now use the "Asherman Chest Seal", pictured below:

This is an extremely sticky dressing that is applied over a hole in the patient's chest, taking the place of the old three sided dressing, and can be used in conjunction with a chest tube. Upon inhalation, the rubber tube projecting up from the dressing seals it self flat, preventing air from entering the pleural cavity. On exhalation, outgoing air opens the rubber tube and escapes.
That pretty much covers the lungs and the two types of pneumothoraces. I would also like to refer again to the diagram of the lungs.
Note that, on the inside border of each lung, there is an opening referred to as the "hilum of the lung". This is the only opening in the lung, and through this portal must pass the bronchus and pulmonary arteries and veins (see below). The brochi (plural for bronchus) are the two airways that the trachea (windpipe) separates into once the trachea enters the chest.
(diagram of cross section of right lung hilum shown in next post)
As you can imagine, with all of the things entering the visceral pleural cavity through the hilum, sealing the hilum is difficult. When a tension pneumothorax is present, with air pressures above anything normally seen in the pleural cavity, some air leakage (as well as blood) through the hilum is inevitable, and this leakage of air and blood will be observed in the mediastinum.
That's all I'm going to write for today, other than to say that when a patient's breathing is listened to with a stethoscope, there will be severely reduced, often absent, breath sounds in the lung suffering a tension pneumothorax. Also, as the built up air pressure in the affected lung tends to push the mediastinum contents toward the other lung, a classic and universally observed sign of a tension pneumothorax is that the patient's trachea (observed on his lower neck) will be deviated away from the side of his chest that has the tension pneumothorax.
Please go back and read the selections from the Warren Commission testimony of Drs. Carrico and Perry that I posted earlier. If you keep in mind what I have typed in this post, I believe you will be able to see that these gentlemen did not believe they were addressing a simple through and through bullet wound of the lower neck.
-
There, I've given the topic its own thread, in the hopes the debate will migrate here and stop hijacking other threads.
-
Sorry for the delay in my analysis of the medical evidence. I know I said I would deliver it a couple of days ago but, since then, I've been busier than a one legged man in a butt kicking contest. Hopefully I can start on it tonight.
-
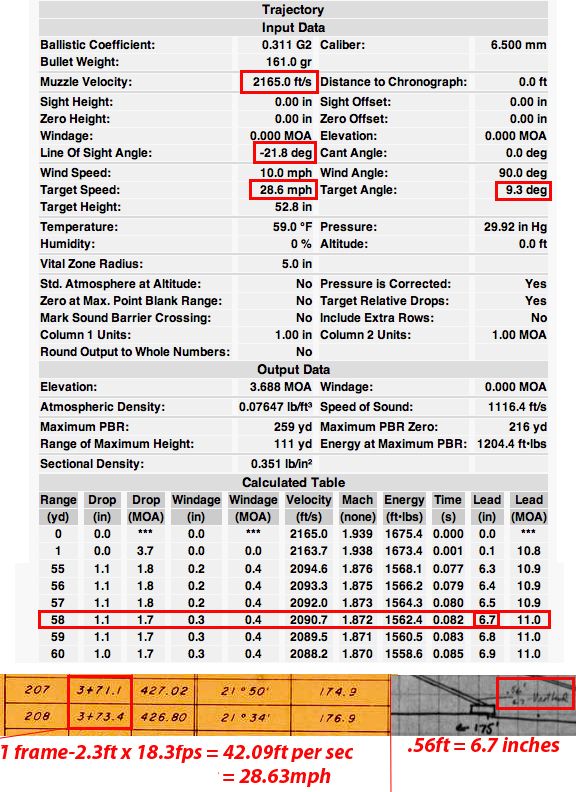
A quick refresher into the reality of ballistics.
Obviously didn't come from the 6th floor snipers nest.
Hi Chris
I see the ballistic coefficient for the 6.5mm Carcano bullet is given as .311. Was this, plus the rest of the info here, supplied by the FBI?
The reason I ask is that I have calculated a BC for this bullet as high as .521.
-
Yes, gentlemen, I'm sure it could have been a rocket propelled flechette, or even a laser fired from a passing UFO.
Whatever the case, on this particular thread, I am assuming the entrance wound in JFK's back was caused by a bullet, and I really don't feel like getting into another long drawn out flechette vs. bullet debate; at least not on this thread anyways.
If you wish to discuss the poisoned flechettes, please show me the courtesy of doing so on another thread, and perhaps I will drop in and offer my opinion on the matter. The medical information I will be conveying on this thread is so complex, it will be difficult for anyone to comprehend if they have to sort through distracting off-topic posts to get at it.
-
I haven’t studied the medical evidence to any great degree but I’ve always found it curious that there was a back wound that barely penetrated and, if you believe the throat defect was an entry wound, a throat shot that never exited.
Could supressors/silencers take that much velocity off a bullet? Just speculation. I find those two underpowered shots to be an interesting coincidence.
No, suppressors do not reduce the velocity of a bullet; not by 80% anyways. Any reduction in velocity would be miniscule.
The real question you should be asking is how a bullet travelling at an 80% reduction in velocity actually made it to the target without dropping to the earth far short of its target.
-
First off, I must establish that I do not believe the back wound was connected in any way to the throat wound. Nor do I believe it was a through and through wound that exited the front of JFK's chest.
Humes was correct in searching through all of JFK's chest and abdominal organs, looking for a bullet or fragments of a bullet. In all fairness to Humes, he may have been genuinely unaware of the exotic type of bullet employed, and he may also have been sincerely puzzled at his inability to find a bullet or fragments of a bullet.
Here is something to think about, though. If an intact bullet, or fragment of a bullet, did range downward through his chest and lodge in an abdominal organ, where Lipsey stated Humes was searching for a bullet or bullet fragment, that bullet or fragment would leave an unmistakable path through the organs it traversed, showing tissue damage and haemorrhaging. In other words, Humes would not continue his search downward into the abdiminal organs without seeing obvious proof of passage of a bullet or fragment. Also, the diaphragm, separating the pleural cavity from the abdominal cavity, is one great unbroken expanse of tissue stretching from one side to another of the bottom of the pleural cavity. If a bullet or fragment passed from the pleural cavity to the abdominal cavity, it had to go through the diaphragm and it would have left a very obvious hole doing so.
Unless Humes was a complete idiot, why would he be searching abdominal organs for a bullet or fragment of a bullet if his initial exploration revealed an intact diaphragm?
-
Robert,
The Sibert O'Neil report is quite specific. They witnessed Humes making this probe. The report reads that they witnessed Humes probing this wound. The idea that Humes fooled them does not seem realistic or probable. We know both had been instructed to witness everything and report back. Just because you could not do so, is not proof that Humes was also unable to do so?
I take it from your expression "it is time to let the shallow wound go" that you feel this may be a through wound. If I am right I will be interested how you can establish that.
James.
James
How close were Sibert and O'Neil to JFK when Humes supposedly probed the back wound with his finger? Were they standing right beside Humes, looking down, or were they in the gallery many feet away? Where does it actually state Humes used his pinkie finger?
Has it ever occurred to anyone that Humes was so inept, he thought he had found the bottom of the wound, simply because he could not work his fat finger any further into the 1/4 inch diameter entrance wound?
I'm sorry but, if the only evidence of a shallow back wound is two FBI agents, untrained in medical procedures, watching an autopsist from halfway across an autopsy theatre, there really is not much of a case for a shallow back wound.
Once again, if Lt. Lipsey correctly reported to the HSCA the autopsists spending such a great deal of time dissecting the chest and abdominal organs in search of bullet fragments, doesn't this tend to contradict Humes' first finding of a shallow back wound, especially if Humes believed the bullet that caused this back wound had entered JFK's back at a downward angle of 45° to 60°? Does not Humes' estimation of a 45° to 60° downward angle call into question his ability as an autopsist, or is it possible JFK was shot from a helicopter?
-
Robert,
I do not have all my notes with me at the present, however I recollect that Sibert and O’Neil stated that Humes did indeed probe the wound with his pinkie. An that he concluded that it was a shallow wound.
I agree that the lung was damaged, but not anywhere near where T3 is located. Humes in testimony describes a wound - which he refers to as a bruise - was at the top of the lung.
Commander HUMES. “The bruise here, photographs are far superior to my humble verbal description, but if I let my hand in cup shaped fashion represent the apical parietal pleura, it was an area approximately 5 cm. in greatest diameter of purplish blue discoloration of the parietal pleura. Corresponding exactly with it, with the lung sitting below it, was a roughly pyramid-shaped bruise with its base toward the surface of the upper portion of the lung, and the apex down into the lung tissue, and the whole thing measured about 5 cm., which is a little - 2 inches in extent, sir.” H2 369
The ammunition that you describe in post 4, had that kind of ammunition penetrated JFK’s body it would have created damage that could never have been concealed.
You are right to raise the issue of the back wound. It is indeed a problematic wound. If the wound did not enter the body - as I believe - then what caused that damage and where is the object that created that wound.?
I hope you do not intend to link the back wound with the throat wound. Such a link is impossible.
I will follow this thread with interest and reflect on your thinking on this subject.
James.
James
I realize Sibert and O'Neil claimed to have witnessed Humes attempt to probe the back wound with his pinkie finger. As I have repeatedly stated, the Carcano bullet is roughly 1/4 inch in diameter, and I have measured the diameter of my pinkie finger at the first knuckle and found it to be roughly 3/4 inch. Is it not possible that Sibert and O'Neil were taken in by Humes, and that Humes simply could not put his pinkie finger into such a small hole? As I pointed out, I have tried this with larger .30 calibre (.308 inch) entrance wounds in deer, and my finger simply will NOT go into the hole.
The shallow back wound myth was attractive, for the simple fact it contradicted the Single Bullet Theory. However, there are so many other ways to disprove the SBT, it is time to let the shallow back wound go.
It is interesting to read the HSCA interview of Lt. Richard Lipsey, an officer with no medical experience who witnessed most of the autopsy and who likely overheard a great deal of the conversation between Humes, Finck and Boswell. According to Lipsey, the majority of the autopsy was spent dissecting the organs of the chest and abdomen looking for bullet fragments or a bullet. If the back wound did not penetrate the pleural lining of the chest, what would have been the point of dissecting these organs in search of bullet fragments?
-
Below are excerpts from, first, the Warren Commission testimony of Dr. Charles Carrico, followed by selected excerpts from the Warren Commission testimony of Dr. Malcolm Perry. I am posting these excepts in this order because Carrico arrived in Trauma Room One before Perry, and was the first doctor to attempt to establish a patent airway in JFK. When Carrico's endotracheal tube proved ineffective, Perry elected to perform a tracheotomy.
Mr. SPECTER - What did you observe as to the President's condition upon his arrival?
Dr. CARRICO - He was lying on a carriage, his respirations were slow, spasmodic, described as agonal.
Mr. SPECTER - What do you mean by "agonal" if I may interrupt you for just a moment there, Doctor?
Dr. CARRICO - These are respirations seen in one who has lost the normal coordinated central control of respiration. These are spasmodic and usually reflect a terminal patient.
Mr. SPECTER - Would you continue to describe your observations of the President?
Dr. CARRICO - His-- the President's color--I don't believe I said--he was an ashen, bluish, grey, cyanotic, he was making no spontaneous movements, I mean, no voluntary movements at all. We opened his shirt and coat and tie and observed a small wound in the anterior lower third of the neck, listened very briefly, heard a few cardiac beats, felt the President's back, and detected no large or sucking chest wounds, and then proceeded to the examination of his head. The large skull and scalp wound had been previously observed and was inspected a little more closely. There seemed to be a 4-5 cm. area of avulsion of the scalp and the skull was fragmented and bleeding cerebral and cerebellar tissue. The pupils were inspected and seemed to be bilaterally dilated and fixed. No pulse was present, and at that time, because of the inadequate respirations and the apparent airway injury, a cuffed endotracheal tube was introduced, employing a larynzo scope. Through the larynzo scope there seemed to be some hematoma around the larynx and immediately below the larynx was seen the ragged tracheal injury. The endotracheal tube was inserted past this injury, the cuff inflated, and the tube was connected to a respirator to assist the inadequate respiration. At about this point the nurse reported that no blood pressure was obtained. ""Mr. SPECTER - You had begun to describe some of the action taken in order to endeavor to revive the President. Will you continue with that description, please?
Dr. CARRICO - I believe we were to where the endotracheal tube had been inserted. After this, the President--his respirations were assisted by the Bennett machine. We again listened to .his chest to attempt to evaluate the respirations. Breath sounds were diminished, especially on the right, despite the fact that the endotracheal tube was in place and the cuff inflated, there continued to be some leakage around the tracheal wound. For this reason Dr. Perry elected to perform a tracheotomy, and instructed some of the other physicians in the room to insert chest tubes, thoracotomy tubes. "
"Mr. SPECTER - Upon your arrival in the room, where President Kennedy was situated, what did you observe as to his condition?
Dr. PERRY - At the time I entered the door, Dr. Carrico was attending him. He was attaching the Bennett apparatus to an endotracheal tube in place to assist his respiration.
The President was lying supine on the carriage, underneath the overhead lamp. His shirt, coat, had been removed. There was a sheet over his lower extremities and the lower portion of his trunk. He was unresponsive. There was no evidence of voluntary motion. His eyes were open, deviated up and outward, and the pupils were dilated and fixed.
I did not detect a heart beat and was told there was no blood pressure obtainable.
He was, however, having ineffective spasmodic respiratory efforts.
There was blood on the carriage. ""Mr. SPECTER - Would you continue to describe the resuscitative efforts that were undertaken at that time?
Dr. PERRY - At the beginning I had removed my coat and watch as I entered the room and dropped it off in the corner, and as I was talking to Dr. Carrico in regard to the neck wound, I glanced cursorily at the head wound and noted its severe character, and then proceeded with the tracheotomy after donning a pair of gloves. I asked that someone call Dr. Kemp Clark, of neurosurgery, Dr. Robert McClelland, Dr. Charles Baxter, assistant professors of surgery, to come and assist. There were several other people in the room by this time, none of which I can identify. I then began the tracheotomy making a transverse incision right through the wound in the neck.
Mr. SPECTER - Why did you elect to make the tracheotomy incision through the wound in the neck, Dr. Perry?
Dr. PERRY - The area of the wound, as pointed out to you in the lower third of the neck anteriorly is customarily the spot one would electively perform the tracheotomy.
This is one of the safest and easiest spots to reach the trachea. In addition the presence of the wound indicated to me there was possibly an underlaying wound to the neck muscles in the neck, the carotid artery or the jugular vein. If you are going to control these it is necessary that the incision be as low, that is toward the heart or lungs as the wound if you are going to obtain adequate control.
Therefore, for expediency's sake I went directly to that level to obtain control of the airway.
Mr. SPECTER - Would you describe, in a general way and in lay terms, the purpose for the tracheotomy at that time?
Dr. PERRY - Dr. Carrico had very judicially placed an endotracheal but unfortunately due to the injury to the trachea, the cuff which is an inflatable balloon on the endotracheal tube was not below the tracheal injury and thus he could not secure the adequate airway that you would require to maintain respiration.
(At this point, Mr. McCloy entered the hearing room.)
Mr. SPECTER - Dr. Perry, you mentioned an injury to the trachea.
Will you describe that as precisely as you can, please?
Dr. PERRY - Yes. Once the transverse incision through the skin and subcutaneous tissues was made, it was necessary to separate the strap muscles covering the anterior muscles of the windpipe and thyroid. At that point the trachea was noted to be deviated slightly to the left and I found it necessary to sever the exterior strap muscles on the other side to reach the trachea.
I noticed a small ragged laceration of the trachea on the anterior lateral right side. I could see the endotracheal tube which had been placed by Dr. Carrico in the wound, but there was evidence of air and blood around the tube because I noted the cuff was just above the injury to the trachea.
Mr. SPECTER - Will you now proceed to describe what efforts you made to save the President's life?
Dr. PERRY - At this point, I had entered the neck, and Dr. Baxter and Dr. McClelland arrived shortly thereafter. I cannot describe with accuracy their exact arrival. I only know I looked up and saw Dr. Baxter as I began the tracheotomy and he took a pair of gloves to assist me.
Dr. McClelland's presence was known to me at the time he picked up an instrument and said, "Here, I will hand it to you."
At that point I was down in the trachea. Once the trachea had been exposed I took the knife and incised the windpipe at the point of the bullet injury. And asked that the endotracheal tube previously placed by Dr. Carrico be withdrawn slightly so I could insert a tracheotomy tube at this level. This was effected and attached to an anesthesia machine which had been brought down by Dr. Jenkins and Dr. Giesecke for better control of circulation.
I noticed there was free air and blood in the right mediastinum and although I could not see any evidence, myself any evidence, of it in the pleura of the lung the presence of this blood in this area could be indicative of the underlying condition.
I asked someone to put in a chest tube to allow sealed drainage of any blood or air which might be accumulated in the right hemothorax.
This occurred while I was doing the tracheotomy. I did not know at the time when I inserted the tube but I was informed subsequently that Dr. Paul Peters, assistant professor of urology, and Dr. Charles Baxter, previously noted in this record, inserted the chest tube and attached it to underwater seal or drainage of the right pneumothorax. "Everything you need to know about an injury to JFK's right upper lung and the conditions and signs it produced can be found in these four excepts from these two doctors.
Examine them and, tomorrow, I will analyze precisely what it was they were attempting to relate to Specter and the Warren Commission.
-
So, if the bullet did penetrate JFK's Right Upper Lung, why did it not exit the front of his chest? The most reliable medical information we have access to are the Parkland surgeons' first day medical reports, and not one of these mentions an exit wound in the front of JFK's chest. Therefore, if I am correct about the "short shot" myth, one of two things happened:
1) JFK was shot in the back with a rapidly expanding bullet (ie. hollow point) that came to a stop partway through his chest cavity. This would necessitate removal of this bullet prior to autopsy or the removal of this bullet at the autopsy and concealing its discovery and removal from any witnesses present.
2) JFK was shot in the back with a type of hollow point bullet made entirely from compressed metal powder, known as a "frangible" bullet. This bullet would be under great hydraulic stress travelling through the soft tissue of the right lung, and would completely disintegrate into a cloud of metal powder, capable of great destruction, partway through the lung.
I should point out that both a hollow point and a frangible bullet will make a tiny entrance wound in soft tissue and they will both perform to the full capacity of their destructiveness without coming in contact with any bony structure. In fact, both of these bullets perform far better only travelling through soft tissue. This is not to say, though, that they are incapable of penetrating skull bone. They will penetrate skull bone, leaving only a small entrance wound, and then wreak utter devastation travelling through brain matter.
-
Quite frankly, I don't believe such a slow bullet could have ever made it to JFK's back, making the shallow back wound a myth; at least in my eyes anyways.
So what are you saying happened, Bob? Humes probed the back wound and it terminated not very deeply. You can see the wound on the autopsy photo. You can see the bullet hit Kennedy in the Z film right after he throws his hands up - he lurches forward and his head bobs backward and then forward from the force of the bullet.
I'm genuinely curious what your alternative theory to the back wound myth is.
Well, think about this for a minute, Michael. A 6.5mm Carcano bullet, which actually measures 6.8 mm in diameter, equates to just a shade over 1/4 inch in diameter (.2677 "). I measured my pinkie finger at the first knuckle and found my finger to be roughly 3/4 inch in diameter.
Unless Humes had fingers like a 4 year old girl, how was he able to probe the entrance wound with his finger? Do you believe skin and muscle is elastic enough to stretch the entrance wound to three times its diameter?
This is why research in this case progresses to a certain point and then stalls. There are so many "facts" in this case that everyone seems to blindly accept. The key is to question everything.
In the next few posts, I will examine the medical evidence (specifically the Warren Commission testimonies of Dr. Charles Carrico and Dr. Malcolm Perry) to see if the surgeons at Parkland gave us any indication of JFK's right lung being wounded. I believe you will be surprised at the evidence that has been right out in front of us for over 50 years.
P.S.
Just for comparison, I have attempted, in the past, to probe .30 calibre (.308") entrance wounds in a deer, and have been unable to insert my finger into one of these slightly larger entrance wounds.

JFK's "SHALLOW" BACK WOUND REVISITED (FOR THE UMPTEENTH TIME)
in JFK Assassination Debate
Posted
This is how simple Humes' job was. Make the "Y" incision, remove the abdominal and chest organs, look inside JFK's rib cage to see if there is a very obvious 1/4 inch hole into the rib cage from JFK's back. If no hole is found in the back of the rib cage, or anywhere else on the interior of the rib cage, do not waste time and effort dissecting all of the organs for bullets or fragments.
Humes was either hiding something or he was the most assbackwards S.O.B. to ever conduct an autopsy. (excuse my French)