

Robert Prudhomme
-
Posts
4,105 -
Joined
-
Last visited
Content Type
Profiles
Forums
Events
Store
Posts posted by Robert Prudhomme
-
-
-
Pat
Did any of the doctors at Parkland report an obstructed airway? Outside of the tracheal wound, what was there to justify a tracheotomy? You do realize how much more complicated and time consuming a tracheotomy is compared to intubation by endotracheal tube, don't you? You're also forgetting Carrico had a laryngoscope at his disposal and would have been able to quickly determine if JFK's airway was obstructed from "his own brain matter or some such thing". The mere fact he had already inserted and inflated the endotracheal tube demonstrated there was an unobstructed airway.
Here is something else to think about. After assisted ventilation was begun and Carrico determined there was leakage of air from the chest through the tracheal wound, after intubating JFK with an endotracheal tube, why did he simply not deflate the cuff of the e. tube, re-insert the e.tube lower to get the cuff below the tracheal wound, and re-inflate the cuff?
-
Sandy,
There is a couple of points I ought to make,
a) the Connally wound was down the outside of his rib. From what I remember the direction of the bullet traveled down the right side of his body in a straight line. The position of Connally - at that moment - as well as the position of the car at Z 230 made that possible.
( b ) Whereas Connally's wound entered just under his arm pit, the Kennedy wound is a few centimetres right of his spine. A missile entering that point from the west window will be moving in a right to left direction. That may have an impact on your calculations.
c) Moving the car up to the position of the Stemmons sign will certainly affect to what degree any shooter could hit that point on Kennedy's back. Down at Z 230 the car is forward of the west window. At Z 220 - or thereabouts - the car is still forward of the East window, but I am not sure what it's location would be with regard to the West window.
Just some thoughts for you.
James.
Thanks James.
Your point ( b ) makes me realize that a shot from the west TSBD window may well have missed the right lung altogether. That is to say, particles from the frangible bullet may have missed. They may have gone into the mediastinum.
I've long doubted that any shots were taken from the "Oswald" window. But that's just a hunch of mine. The shot may have taken place from there. Or from the Dal-Tex building.
Hi Sandy
It is impossible for a shot to the back, at the level we are discussing, to enter to the right of the vertebrae without penetrating the right lung.
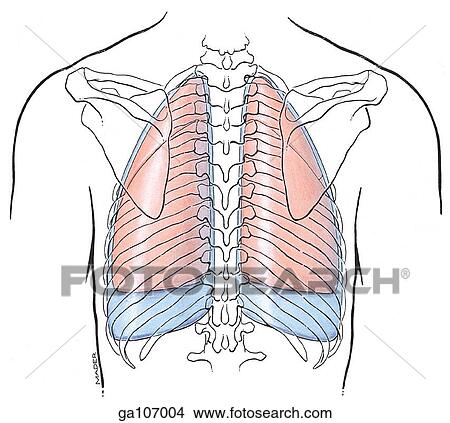
This diagram clearly shows the margin of the right lung up against the vertebrae. To reach the mediastinum, from an entrance wound 1.5-2 inches to the right of the spinal midline, a bullet would have to pass through the right lung.
-
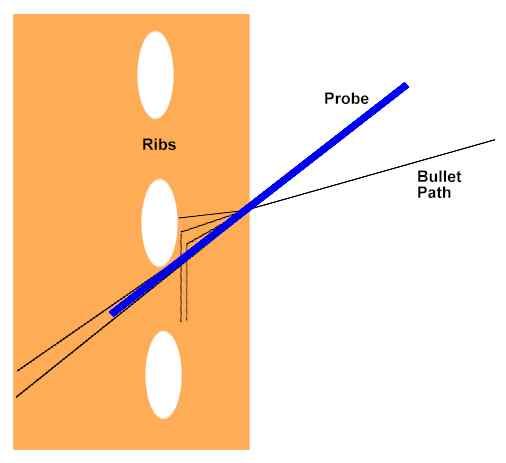
Why Humes Thought the Back Missile Hit at a Sharp Angle -- a Hypothesis
Dr. Humes was reported to have said during the autopsy that the bullet entered JFK's back at a 45 to 60 degree angle. For example, FBI agent Francis O'Neill reported this in his 1978 HSCA affidavit. How could a bullet have entered at such a steep angle?
The first thing to ask is, what made Humes think the bullet entered at that angle. Given that Humes apparently found no missile track other than the wound running through JFK's flesh (skin and shallow muscle), I would think that at some point during the autopsy he probed the wound. Probably not with his finger -- it being too large to fit -- but probably with a metal probe. At which time Humes found the angle of that track to be 45 to 60 degrees... quite a steep angle that cannot easily be explained.
Groundwork
Before presenting my hypothesis, I need to lay a little groundwork. (Please be patient. If you don't want to read the groundwork, jump ahead to the hypothesis.)
Many of you know that I -- having studied Robert Prudhomme's case for a frangible bullet being the explanation for this disappearing bullet -- am quite convinced that a frangible bullet was used on the back shot. Since reading Robert's descriptions of these bullets, I've done some reading about them on my own. Here are a few things I've learned from Robert and elsewhere:
- Due to the fact that frangible bullets break up into numerous particles upon hitting a substance of sufficient hardness and resistance, each particle will contain just a small fraction of the whole bullet's kinetic energy.
- The energy per unit surface area will decrease greatly upon fragmentation. This means the penetration depth will be greatly diminished.
- The finer the powder comprising the bullet, the more diminished the penetration will be, and the broader the spread.
- Frangible bullets can be designed to fragment more or less easily. Even so, there can be great variation from bullet-to-bullet as to what it takes to fragment the bullet.
One thing I set out to find for this presentation was how a bone would react to being hit be an already-fragmented frangible bullet. Unfortunately I couldn't find anything specific to that topic. I did, however find some related materials that I feel confirmed what I already thought about this. It is my contention that a fragmented bullet would be much less likely to shatter a bone than would be a whole bullet of the same mass.
I will give an analogy to demonstrate this.
Suppose we have a pane of glass, and that this represents a bone. A one pound rock represents a whole bullet. A pound of pebbles represents a fragmented frangible bullet. And a pound of sand represents a fragmented ultra-frangible bullet.
First we "shoot the bone" by throwing the rock at the glass with all our might. The glass breaks. Just like a whole bullet would break a bone.
Next we throw the pebbles at the glass. (A new pane of glass.) The glass flexes and gets pitted, but does not break... this time. Maybe it will break next time.
Finally we throw the sand at the window. Very little happens to the glass. The grains of sand merely bounce off. Despite the fact that they carried the same amount of energy as the rock did.
I hope you will now agree with me that a bone will be far less affected by a fragmented frangible bullet than by a whole bullet.
But before leaving this analogy, let's try one more thing. Let's throw the sand at the glass, but this time at a slight angle. What will the sand do? Analyzing this situation can be very daunting, as several factors would need to be taken into account. For example, the fact that early reflected particles could collide with later oncoming ones, depending upon the diameter of the spray. Also, the degree to which each of the many collisions are elastic. ("Elastic" and "inelastic" are technical terms used in physics to classify and describe collisions.) After studying this for some time, I decided that another approach was necessary.
Suppose we dropped a rock on a sidewalk. Would it bounce, or would it stay on the sidwalk upon impact? If the collision were a perfectly elastic one, the rock would bounce up to the same height from which it was dropped. If it were perfectly inelastic, the rock would drop to the ground without bouncing.
I can tell you one thing from experience... a rock won't bounce very high. And it's not just because of gravity. If you've ever played with a Super Ball, you know what a good elastic collision is. And a rock landing on concrete ain't one of them. (Wikipedia describes a Super Ball as "an extremely elastic ball made of Zechron.) But a rock does bounce a little. The reason a rock doesn't bounce high like a Super Ball is because it loses a lot of its kinetic energy when impacting the concrete.
Now, suppose you threw the rock at the concrete at a slight angle. What would it do? It would bounce a little, as before. But this time it would travel in the direction you threw it, till its kinetic energy was depleted. If it were thrown at a smooth surface it would travel quite far. Ever skipped a rock on calm water?
Okay, having gone through that thought experiment, I want to determine what would happen if you threw sand instead of a rock at concrete, again at a small angle. I can't remember every throwing sand at a sidewalk, but I imagine it would behave in a way similar to a single rock. I am confident it wouldn't bounce much at all.... I think even less so than a rock. I'm equally confident that it would move across the surface in the direction thrown, especially if the surface is smooth.
Okay, now it's time to translate this back to bullets and bone. One major difference between the two is that bone is more flexible than concrete, is less rigid, and is surrounded by muscle. The effect of these factors is that the bone would absorb a lot more energy than concrete does. So any collision with bone would be a lot less elastic than with concrete. That is to say, the projectile would bounce much less.
I readily admit that I haven't proven what I'm about to say. But I contend that if a fragmented frangible bullet hits a bone at an angle, the particles will tend to skim along the surface of the bone. The particles won't all be in contact with the bone, but will travel near the surface of the bone, perpendicular to its surface.
Hypothesis
Here is what I envision happened:
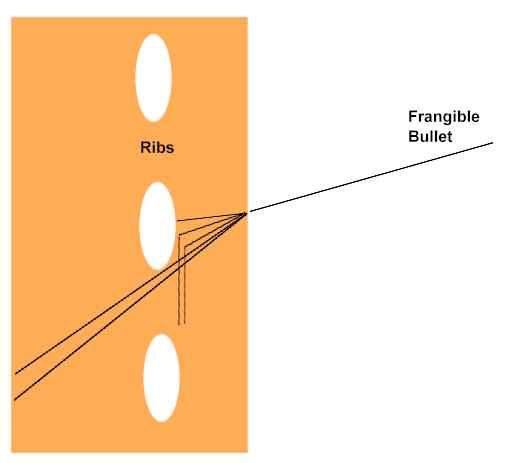
The frangible bullet hit Kennedy's back and began to fragment immediately after hitting the surface of the skin. That it fragmented so near the surface may have been by design, or may have been a fluke.
The angle of the shot was, of course, downward... on the order of 20 degrees. The bulk of the particles hit the bottom portion of a rib and skimmed along its surface toward Kennedy's butt. But the bottom portion of the particle spray passed below the rib and punctured the lung.
The particles that were deflected downward, and those that passed below the rib, created a channel that Humes found with a probe. The angle of the channel was estimated by Humes to be 45 to 60 degrees.
You can see this in the following illustrations.
Related Images
Following are photos, x-rays, and CT scans of a pig's hind leg that has been shot with a frangible bullet. Note that this bullet fragmented immediately after striking the skin. The bullet used was a so-call "hyper-frangible." Due to its small particle size and low velocity (~500 fps), penetration was very shallow.
It would have been useful for this presentation had the bullet been aimed at the bone and been of greater velocity.


This is a CT scan of the leg. It is a cross-sectional view. The white circle is the bone.
(Source for images: Forensic and clinical issues in the use of frangible projectilea.)
Hi Sandy
This is a very interesting post you have written, and it opens up all kinds of possibilities. I'd like to respond to it but I'm a bit pressed for time at the moment. Hopefully I can write something tonight.
-
I don't think any of you quite get it.
Sibert, O'Neill and others at the autopsy discussed a soft point bullet, a plastic or ice dissolving bullet and a bullet that would completely "fragmentize" in a wound.
If Humes opened JFK up and found nothing but pristine untouched chest and abdominal organs, and no bullet hole in the outer pleural lining, how did anyone arrive at any of the above conclusions?
-
In his HSCA testimony, Dr. Ebersole indicated that information regarding the throat wound and tracheotomy was received from Parkland Hospital during the autopsy. Though he couldn't recall how the information was conveyed. (Source) He referred to the throat wound as one of exit, which contradicts what was believed at Parkland. I believe he did that because (according to Lt. Lipsey) the doctors were convinced at the time that the throat wound was one of exit for the EOP entrance wound.
As I said, Humes had to be aware of the throat and trachea wounds at some point during the autopsy. I would wager he had spotted the wounding of the throat and trachea long before receiving a call from Dallas, otherwise he would have questioned why Perry performed a tracheotomy on a pristine neck, when a simple intubation with an endotracheal tube would have achieved the same objective in a fraction of the time. When dealing with a pulseless non-breathing patient, time is not something to waste.
I'm always amused by researchers who believe that Perry was able to completely obliterate the throat and tracheal wounds with a couple of scalpel strokes. That's almost as funny as Superman disguising himself as Clark Kent by donning a pair of glasses.
-
I'll let these images tell my post here.Cliff - Expanding on that right-there-in-the-historical-record Scenario I can buy the first shot to the throat as a paralytic, the shot to the back a toxin. The shot to the throat wasn't a kill shot -- the second hit, to the back, had to be a kill shot. IMO.Really Cliff? Is it possible that you've read one too many spy and cloak and dagger novels?No, I actually read the evidence. Give it a try, sometime.
From autopsy-attendee FBI SA Francis O'Neill's sworn affidavit for the HSCA:
<quote on>
Some discussion did occur concerning the disintegration of the bullet. A general
feeling existed that a soft-nosed bullet struck JFK. There was discussion concerning
the back wound that the bullet could have been a "plastic" type or an "Ice" [sic]
bullet, one which dissolves after contact.
<quote off>
From autopsy-attendee FBI SA James Sibert's sworn affidavit for the HSCAt:
<quote on>
The doctors also discussed a possible deflection of the bullet in the body caused
by striking bone. Consideration was also given to a type of bullet which fragments
completely....Following discussion among the doctors relating to the back injury, I
left the autopsy room to call the FBI Laboratory and spoke with Agent Chuch [sic]
Killion. I asked if he could furnish any information regarding a type of bullet that
would almost completely fragmentize (sic).
<quote off>
It never fails to amaze me why the research community always seems to suspect poison darts, stun bullets, and the like.It never fails to amaze me how Pet Theorists disregard the historical record.It was the autopsists who thought JFK may have been hit with a high tech weapon.It was the FBI men who took the scenario seriously.Who gives a quad-x what you think?There was simply no need to go through such an elaborate and possibly faulty spy weapons when some simple bullets would do the job.Not if the first shot resulted in a non-fatal wounding, or a miss, allowing the target to duck down.First-shot-kill-shot was not a 100% guarantee.Hi Cliff
Going over the words you quoted from Sibert and O'Neill, I began to look at them in a new light.
Why would the bullet that struck JFK's back be viewed as everything from a soft point bullet to one that would "fragmentize" completely, if a great deal of corresponding internal damage was not discovered in JFK's thoracic cavity?
And then there was the autopsists' theory that the bullet was deflected in the body after striking bone. Would they be discussing this if they opened JFK's chest, and found his right lung in pristine condition? I have seen many animals shot through the lung(s) and there is NO mistaking whether or not a bullet has passed through the lung(s).
-
According to Dr. Humes and the WCR, Humes did not know about the throat wound till the morning after the autopsy. This is not true.
The truth is that he learned of it long before Kennedy's body had even arrived in Maryland.
How do we know that?
First we have the testimony of Dr. Robert Livingston, who at the time was Science Director of the National Institutes of Health. He had heard news reports regarding the throat wound and felt it necessary to pass this information on to whomever would be performing the autopsy. He called Bethesda Naval Hospital and spoke with Dr. Humes about the throat wound at around 3:30 or 4:00 PM eastern time. (Kennedy's body didn't arrive at the hospital till 6:35 PM ET.)
Dr. Livingston has related this story a number of times. One time was when he testified in Dr. Crenshaw's defamation lawsuit against the American Medical Association. (Dr. Livingston's testimony here.)
Testimony given by Lt. Richard Lipsey also indicates that Humes knew about the throat wound on the day of the autopsy. He testified that the autopsy doctors were convinced that the throat wound was the exit for the entrance wound located near the external occipital protuberance (EOP), which is near the hairline on the back of the head. Of course, for them to form that conclusion, they had to have known about the throat wound. [Need to find Lipsey's testimony.]
I'm posting this for the benefit of anybody who is unaware of this particular WCR L.I.E.
James is right. Regardless of whether or not Humes knew about the throat wound, Livingston's claim he called Humes is clearly bogus. He never came forward until the 90's, when he contacted Lifton. Lifton failed to buy into it, so Livingston then contacted Livingstone. The bottom line is that Livingston claimed the small size of the throat wound was discussed by a nurse on the radio, and that this led him to call Humes. The problem is that those studying the news footage and broadcasts have found no record of such an interview. There's also this. Livingston claimed he was friends with the journalist Richard Dudman, and that Dudman could vouch for him. Well, I contacted Dudman and he verified that he'd known Livingston for decades, and that Livingston had talked to him more than once about the Kennedy assassination. But, get this, he had no recollection of Livingston ever claiming he'd talked to Humes, or some such thing. Now, Dudman was quite an old man at this time, so I chose to not come forward with this for fear Fetzer and others would proceed to attack him. (Fetzer is the main proponent of Livingston's credibility on this issue.) In any event, I never felt the need for confronting Fetzer on this seeing as Fetzer discredited Livingston all by himself when he disavowed the transcript of Livingston's testimony in the Crenshaw case (testimony arranged by Fetzer and put into the record by Doug Horne). You see, I actually read the transcript and spotted some clear problems with it. The one thing that comes to mind is that Livingston said he'd decided to come forward in order to 'save the world". Yikes! A retired man in his seventies who comes forward with a bizarre story without any back-up in order to save the world, and is driven to his court testimony by Dr. James Fetzer, the very same Fetzer who believes the airplanes filmed crashing into the twin towers were holograms, and that Paul McCartney is an imposter impersonating the original Paul McCartney.
Now, that's what I call evidence! Uh, no, I don't.
According to Dr. Humes and the WCR, Humes did not know about the throat wound till the morning after the autopsy. This is not true.
The truth is that he learned of it long before Kennedy's body had even arrived in Maryland.
How do we know that?
First we have the testimony of Dr. Robert Livingston, who at the time was Science Director of the National Institutes of Health. He had heard news reports regarding the throat wound and felt it necessary to pass this information on to whomever would be performing the autopsy. He called Bethesda Naval Hospital and spoke with Dr. Humes about the throat wound at around 3:30 or 4:00 PM eastern time. (Kennedy's body didn't arrive at the hospital till 6:35 PM ET.)
Dr. Livingston has related this story a number of times. One time was when he testified in Dr. Crenshaw's defamation lawsuit against the American Medical Association. (Dr. Livingston's testimony here.)
Testimony given by Lt. Richard Lipsey also indicates that Humes knew about the throat wound on the day of the autopsy. He testified that the autopsy doctors were convinced that the throat wound was the exit for the entrance wound located near the external occipital protuberance (EOP), which is near the hairline on the back of the head. Of course, for them to form that conclusion, they had to have known about the throat wound. [Need to find Lipsey's testimony.]
I'm posting this for the benefit of anybody who is unaware of this particular WCR L.I.E.
Dumb question but, doesn't anyone think with Humes being a doctor and all he might have been just a little bit curious to know why Perry had elected to, in the absence of any damage to JFK's airway, perform a complicated and time consuming tracheotomy when a simple intubation with an endotracheal tube would have been much quicker and achieved the same objective?
As is obvious from the testimonies of Perry and Carrico, the endotracheal tube would have worked just fine if only the inflatable cuff had been lower than the tracheal wound.
-
Craig Carvalho said:
"As far as where and when the ammunition was manufactured is irrelevant in this case. The design flaw built into this cartridge in the late 19th century was still there in 1963 even when Western was manufacturing it. Bob's assertion that Western's version of this cartridge was all but devoid of malfunctions is patently absurd. Research any of the "recreations/documentaries" on this topic and you will find more than one instance where Western's 6.5mm cartridges malfunctioned."
First off, Craig, no one was manufacturing ammunition for the 6.5mm Carcano in 1963, outside of the Italian government who had kept a handful of Carcanos following the Second World War.
Second, the flaws in the 6.5mm Carcano were completely restricted to Italian military ammo.
There were two main flaws with Italian military ammo, mostly manufactured by the Societa Metallurgica Italiana (SMI) and those flaws were the primers used to begin ignition of the cartridge's gunpowder and the crimps used to seal the brass cartridge neck to the bullet.
The Italian primers contained a mixture of chlorate and mercury fulminate, which proved to be somewhat corrosive and was the primary cause of the hangfires and misfires seen in 6.5mm Carcanos. Contrary to what you may believe, American ammo producers, including the Western Cartridge Co., did not use primers containing chlorate and mercury fulminate and thereby avoided the corrosive primer problem, as well as the hangfire and misfire problems. I challenge you to produce evidence of WCC 6.5mm ammo experiencing the same degree of problems experienced by the SMI 6.5mm Carcano ammo, and I know full well you won't be able to do it.
The second flaw was the bullet crimp SMI employed to crimp the neck of the brass cartridge against the cannelure of the bullet. Rather than crimping all around the neck to provide a good seal, as is typical of American ammo producers, SMI employed a curious three point crimp that did not exactly make the best seal.

One of the three point crimps can be seen in the lower cartridge above.
As the WCC employed neither of these features in their 6.5mm Carcano ammo, I fail to see how my assertions can be "patently absurd", Craig. Perhaps you would be so good as to post links to some of these "recreations/documentaries" you speak of that show multiple instances of WCC 6.5mm Carcano ammo failing.
-
Hi Craig
The difference in volume between the first shot and the following shots is likely due to the first shot being fired from a rifle fitted with a suppressor (silencer). I have gone into the evidence supporting this extensively on other threads but would be glad to repeat it here for you.
-
As I have pointed out many times, it has long been held as fact that the bullet that hit JFK's back only penetrated the flesh of his back a mere inch; not far enough to enter JFK's right pleural cavity. This shallow penetration, supposedly probed by Commander Humes' finger, is credited to a phenomenon known as a "short shot", in which a rifle cartridge is either loaded with an insufficent gunpowder charge or the entirety of the gunpowder charge in the cartridge does not ignite, drastically reducing the muzzle velocity of the bullet.
In order to reduce the penetrating power of a 6.5mm Carcano bullet, at a 50 yard range, to the point where this bullet will not penetrate more than an inch in soft tissue, its normal muzzle velocity of 2200 feet per second would have to be reduced to less than about 400 feet per second (fps). This presents all kinds of problems in a) accurately hitting within 20 feet of your target and
 actually getting the bullet to its target.
actually getting the bullet to its target.If you have a rifle that is properly sighted in at a range of, for argument sake, 100 yards, and you chamber a good round into the breech, hitting a target at 50-100 yards is a simple matter of aiming and squeezing the trigger. However, bullets begin to drop as soon as they leave the barrel, and if that bullet leaves the barrel travelling at 1/5th the expected velocity, and the shooter is aiming in a normal fashion and expecting his bullet to be travelling 2200 fps, that bullet will end up impacting the ground (or pavement) far short of the aim point. In the case of JFK, I would not even expect it to hit the back of the limo. This is why it is called a "short shot", as the bullet impacts far "short" of the point of aim.
The next problem you would have with such a slow moving bullet is stability in flight. While the rifling grooves in the rifle's barrel that impart a gyroscopic spin to the bullet in flight account for most of the bullet's stability, the velocity that bullet is travelling at also plays a big part in whether the bullet remains stable in flight, or whether it begins to yaw and tumble on its way to its target. I have seen this problem when handloading rifle cartridges and experimenting with different types of gunpowder, different loads of gunpowder and different weights and styles of bullets. Just by changing the velocity of the bullet slightly, by adding more or less gunpowder, it is possible to over- or under-stabilize a bullet, with the resulting "keyhole" effect on a paper target. A "keyhole" is when a tumbling bullet goes through a paper target side on, leaving the inevitable "keyhole" in the target instead of a round hole. If a bullet still travelling in excess of 2000 fps can be under-stabilized by a reduction in velocity, imagine the lack of stability in the typical 2200 fps bullet reduced in velocity to only 400 fps.
Quite frankly, I don't believe such a slow bullet could have ever made it to JFK's back, making the shallow back wound a myth; at least in my eyes anyways.
My point is this Bob, if Oswald experienced a hang fire, or a combination of perhaps two related malfunctions during his first shot, could this not have caused the shallow back wound? As someone who has a moderate degree of experience with firearms I can tell you that a hang fire would certainly effect the striking point of a projectile on a moving target.
Craig,
It's good to hear such enthusiasm for this subject, but you need to re-read the paragraphs I have copied above from Bob.
This subject has already been covered in depth in an earlier thread on the back wound, and Bob is absolutely correct. To restate it briefly, it's not a simple matter of reducing the velocity of the bullet so that it penetrates the body only an inch or so. Remember this: the shooter doesn't know he's going to get a low energy shot, so he is aiming at the head or the back. The low energy bullet won't even reach the street.
Plot the trajectory and you will see for yourself.
Tom
Hi Tom
I did not see your post before I posted my long reply to Craig. Thanks for the support. It amazes me that you see this so clearly while the more obtuse amongst us have such difficulty grasping the concept.
-
Things have been pretty dull around here lately so, I thought it might be a good time to take another look at JFK's "shallow" back wound; observed by many witnesses to be almost six inches below JFK's collar line (about the level of thoracic vertebra T3) and about 1.5-2 inches to the right of JFK's spinal midline.
First, let's see whereabouts on JFK's back that entrance wound would have been, and how it relates to the location of bones and organs in the upper thorax.

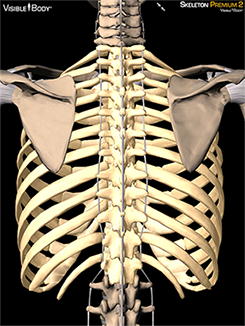
As seen in the top diagram, a bullet entering the back at the level of T3 and 1.5-2 inches to the right of the spine would have nowhere to go but into the Right Upper Lung (RUL). As the skeletal diagram shows, this bullet would miss both the vertebrae and the scapula (shoulder blade) and would have an excellent chance of passing between two ribs, without touching either of them.
As I have pointed out many times, it has long been held as fact that the bullet that hit JFK's back only penetrated the flesh of his back a mere inch; not far enough to enter JFK's right pleural cavity. This shallow penetration, supposedly probed by Commander Humes' finger, is credited to a phenomenon known as a "short shot", in which a rifle cartridge is either loaded with an insufficent gunpowder charge or the entirety of the gunpowder charge in the cartridge does not ignite, drastically reducing the muzzle velocity of the bullet.
In order to reduce the penetrating power of a 6.5mm Carcano bullet, at a 50 yard range, to the point where this bullet will not penetrate more than an inch in soft tissue, its normal muzzle velocity of 2200 feet per second would have to be reduced to less than about 400 feet per second (fps). This presents all kinds of problems in a) accurately hitting within 20 feet of your target and
actually getting the bullet to its target.If you have a rifle that is properly sighted in at a range of, for argument sake, 100 yards, and you chamber a good round into the breech, hitting a target at 50-100 yards is a simple matter of aiming and squeezing the trigger. However, bullets begin to drop as soon as they leave the barrel, and if that bullet leaves the barrel travelling at 1/5th the expected velocity, and the shooter is aiming in a normal fashion and expecting his bullet to be travelling 2200 fps, that bullet will end up impacting the ground (or pavement) far short of the aim point. In the case of JFK, I would not even expect it to hit the back of the limo. This is why it is called a "short shot", as the bullet impacts far "short" of the point of aim.
The next problem you would have with such a slow moving bullet is stability in flight. While the rifling grooves in the rifle's barrel that impart a gyroscopic spin to the bullet in flight account for most of the bullet's stability, the velocity that bullet is travelling at also plays a big part in whether the bullet remains stable in flight, or whether it begins to yaw and tumble on its way to its target. I have seen this problem when handloading rifle cartridges and experimenting with different types of gunpowder, different loads of gunpowder and different weights and styles of bullets. Just by changing the velocity of the bullet slightly, by adding more or less gunpowder, it is possible to over- or under-stabilize a bullet, with the resulting "keyhole" effect on a paper target. A "keyhole" is when a tumbling bullet goes through a paper target side on, leaving the inevitable "keyhole" in the target instead of a round hole. If a bullet still travelling in excess of 2000 fps can be under-stabilized by a reduction in velocity, imagine the lack of stability in the typical 2200 fps bullet reduced in velocity to only 400 fps.
Quite frankly, I don't believe such a slow bullet could have ever made it to JFK's back, making the shallow back wound a myth; at least in my eyes anyways.
Bob, I realize this thread is now examining the medical evidence, and I do not want to go OT, but your original post touched on something I have considered and suggested many times in the past.
In my research I have come to conclusion that, where Oswald's rifle was concerned, the problem was not so much with the firearm itself but with the ammunition it chambered. When the FBI visited Klein's in Chicago, (I believe this was in early 1964), a rifle identical to Oswald's was test fired for them by the same employee who claimed to have mounted Oswald's scope. During this test firing the shop employee recalled that the rifle experienced several "hang-fires" which he believed the FBI may not have even noticed.
I'm sure you are aware Bob what a hang-fire is, but for those reading this post who may not be... a hang-fire is a delay between the pulling of the trigger and the moment at which the round discharges. This can be caused by either a faulty primer, (the small round chamber visible at the base of the cartridge which is struck by the firing pin causing the powder within the casing to ignite), or by the introduction of moisture into the powder within the casing itself. Here is a quote from the same time period in which the MC's ammunition was initially manufactured...
"A paper from 1885 laments that "Gunpowder is such a nervous and sensitive spirit, that in almost every process of manufacture it changes under our hands as the weather changes." Pressing times to the desired density could vary by a factor of three depending on the atmospheric humidity.[89]"
My point is this Bob, if Oswald experienced a hang fire, or a combination of perhaps two related malfunctions during his first shot, could this not have caused the shallow back wound? As someone who has a moderate degree of experience with firearms I can tell you that a hang fire would certainly effect the striking point of a projectile on a moving target.
At any rate, this is quite an interesting subject in particular.
Regards,
Craig C.
P.S. Another interesting point to be considered in this theory is that a majority of eye-witnesses stated that there was a marked difference in the report/sound regarding the first shot fired, and those that followed.
Hi Craig
Klein's was indeed marketing ammunition for the 6.5mm Carcano that was subject to misfires and hangfires. However, this was not the same ammunition reputedly fired at JFK in Dealey Plaza.
The 6.5mm Carcano ammo being marketed by Klein's was exclusively Italian military surplus ammo, and this ammo has been well known for decades for hangfires and misfires. The problem with this ammo is mainly in the corrosive compound used in the primers in these cartridges, compounded by poorly sealed crimps holding the neck of the cartridge to the bullet. This problem is so bad, military surplus websites have advised against shooting these cartridges for years.
OTOH, the ammo reputedly owned by LHO and fired at JFK on 22/11/63 was also 6.5mm Carcano ammo, but manufactured by the Western Cartridge Company of the USA. No corrosive primers were to be found in this ammo, and the crimps were sealed to the bu;lets much better. Consequently, hangfires and misfires are virtually unheard of in this ammo, even today with this ammo being 60+ years old.
The odds of one of these cartridges being fired at JFK and being defective are, to say the least, astronomical. Quoting an article on gunpowder from 1885 is hardly supportive of your argument. You do realize that black powder was still quite prevalent at this time, and that the manufacturing process of gunpowder in 1885 was vastly inferior to modern processes in 2016, don't you?
Now, EVEN IF the bullet fired at JFK's back was fired from a defective cartridge, you seem to be missing the point of my argument. Look at the diagram below.
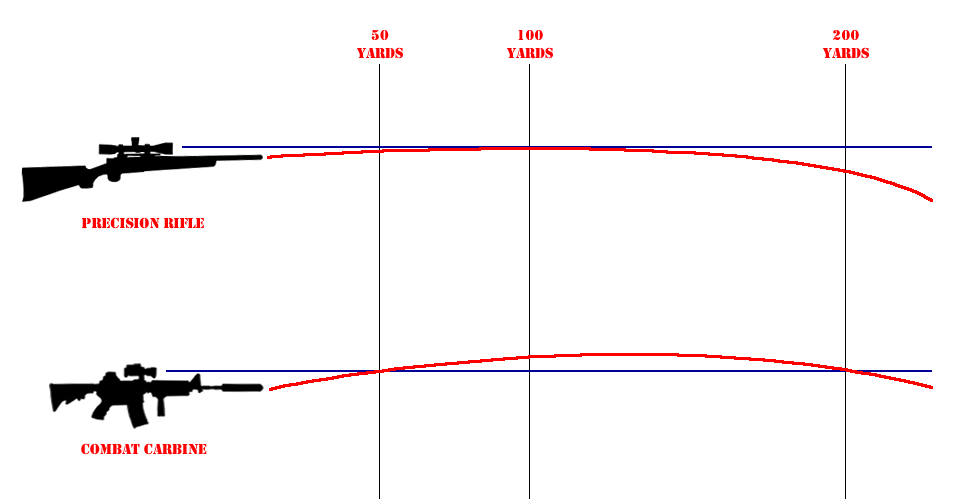
If the barrel of a rifle is pointing straight at a target, as in the top drawing, gravity will pull the bullet earthward as it travels through the air, and it will fall short of the target. It is necessary to elevate the barrel, in relation to the sights (scope) in order to make the bullet follow a high parabolic curve or "trajectory" on its way to the target. Adjusting the height of that parabolic curve at, let's say, 100 yards to make the bullet hit a bullseye is known as "sighting in" or "zeroing" a rifle.
Let's say, for argument's sake, that Oswald had sighted his rifle in for 100 yards and, from experience, knew that he had to shoot a couple of inches low at 50 yards, due the the high point of the parabola, in order to accurately hit a target.
The muzzle velocity of a WCC 6.5mm cartridge's bullet, fired from Oswald's M91/38 6.5mm Carcano short rifle, is just under 2200 feet per second. At 50 yards (the approximate range of the back shot) this bullet would likely still be moving at just over 2100 feet per second. At this velocity, and with the weight and design of this bullet, I would expect a shot impacting JFK's back to go right through JFK's chest, right through John Connally and possibly through the seat in front of Connally, with the potential of injuring Roy Kellerman.
In order for this bullet to merely penetrate the flesh of JFK's back a mere inch, the velocity of this bullet would have to be reduced to the absolute minimum and, just as a guess, I would say it could not have been over 300 feet per second. Look again at the diagram above, and imagine the bullet dropping to earth while the bullet travelled at only 1/7th of its expected velocity. Not knowing he had a defective cartridge, Oswald would be aiming right at JFK, and the bullet would hit the pavement short of the limo, if it made it out of the rifle barrel at all, and did not begin tumbling halfway to where it hit.
-
I'm a bit on the fence with the throat wound, as I find it far more baffling than the back wound. But I agree with you. The apex of the right lung, as the diagrams show, is extremely close to the throat wound. It is not uncommon for the shock wave of a bullet passing through tissue to bruise tissue adjacent to the bullet path. Then again, the bruise at the apex of the right lung reported by Humes may be a total fabrication, or a downplaying and moving of much more extensive lung damage.
"Do you believe that the missile that bruised the lung (as described by Humes) produced ALL of the blood/air as described by Perry and Baxter (as seen through the trach incision)? "
So we are in agreement. Good.No I do not, for three reasons.
1. Humes reported ONLY a small bruise to an otherwise intact lung.
2. Humes reported no collection of blood in the pleural cavity. In order to reach the mediastinum, the blood would have to pass from the pleural cavity, through the hilum of the lung, and OUTSIDE of the right bronchus.
3. Despite 1 & 2, there simply was not enough blood lost into the bruise at the apex of the right lung.
What is it that you "are on the fence" about regarding the throat wound? I made some interesting discoveries regarding the throat a few months back, but haven't posted them due to a lack of interest here on the forum. Maybe they can help you decide...
Hi Tom
My post, # 78, explains what I believe to be another distinct possibility for the throat wound.
What did you discover about the throat wound? Not sure about anyone else but I'm always interested in hearing new information.
-
Just to throw another monkey wrench into the works, it is interesting to return to Lt. Richard Lipsey's deposition to the HSCA.
While he was relating how the autopsists spent so much time dissecting lower organs in search of a bullet of bullet fragments, he also discussed the head wound and the throat wound. I can only assume he was relating what he overheard Humes, Finck and Boswell discussing, as Lipsey had no medical training himself, and was only an observer, and took no active part in the autopsy.
Lipsey related to the HSCA that the consensus was that one bullet struck JFK's just to the right of the external occipital protuberance while another bullet struck JFK's head in (you won't believe this) the cowlick area.
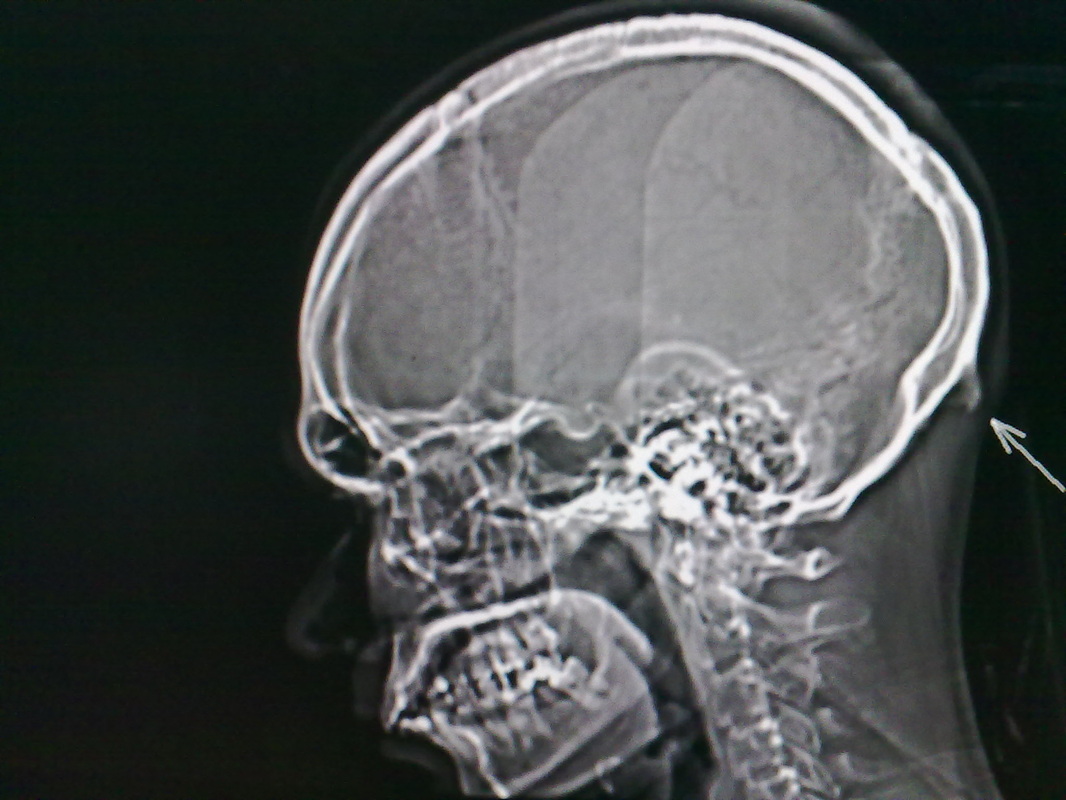
Look at this x-ray with the arrow pointing toward the external occipital protuberance (EOP) and imagine JFK leaning slightly forward, following the back shot, much like the figure in the x-ray is leaning forward. Now imagine a bullet travelling at a 23° angle downward (Dal-Tex Building?) striking JFK just to the right of the EOP.
Would the bullet enter the skull. or slide under the skull and impact the cervical (neck) vertebrae? According to Lipsey, the consensus at the autopsy, at least while he was listening, was that the throat woundwas caused by a bullet fragment from the shot that struck at the EOP, and that the bullet passed under the skull, grazing it as it passed.
We find additional clues to this matter in the HSCA deposition of Jerrol Custer, the x-ray technician who took all of the x-rays of JFK on 22/11/63. He claimed the x-rays he saw of JFK's neck are not the ones he was shown by the HSCA, and that the x-rays he recalled showed many bullet fragments in the vicinity of cervical vertebrae C3/C4.
If we allow for JFK's forward lean, plus the 3% downhill slope of Elm St., is it possible to line up a bullet path that passes through the right of the EOP (under the base of the skull), right side of cervical vertebrae C3/C4 and the right side of JFK's trachea at about the 2nd tracheal ring? I believe JFK was first shot, in the back, when behind the Stemmons sign, and this theoretical shot that passed under his skull may be the "lunge" forward we can see JFK making just as he appears from behind the sign; the one many people have interpreted as JFK "coughing up" a bullet. A bullet impact this high on the torso would account for the "lunge" forward.
If I am correct in this theory, and the Z film is authentic, we would know the exact moment a bullet struck and grazed the lower rear of JFK's skull. Not only that, we know the almost exact location of the entrance and exit wound, assuming the fragment continued on in a straight path. If we could determine the exact position JFK was in at this moment, it should be possible to determine exactly which window of the Dal-Tex Building th shot came from.
-
Bob, given your belief that the back entry is at T3, and I agree, do you agree with my above statement from a previous post? I think you do, but I want to be certain before I move on...Also, IMO, the damage at the apex of the lung is associated ONLY with the throat wound, NOT the back wound. What is your position on this?
Perry and Baxter reported blood and air in the mediastinum which Perry interpreted as indicative of blood in the pleural cavity. Although they didn't see blood between the inner and outer pleura, working only through the trachea incision they could NOT see the entire lung.The main point is that Humes never reported seeing a collection of blood in the pleural cavity between the parietal (outer) pleura and the visceral (inner) pleura that envelops the lung.
As you may recall, I believe the bullet that inflicted the back injury at T3 fragmented, and spread dust-like particles into the right lung. Depending how deeply the bullet penetrated prior to fragmenting, a bullet-sized hole in the lung is certainly a possibility. At some point it obviously fragmented, or it certainly would have exited through his chest. This damage, independent of the injury at the apex of the lung certainly could cause all the symptoms you describe.
Do you believe that the missile that bruised the lung (as described by Humes) produced ALL of the blood/air as described by Perry and Baxter (as seen through the trach incision)? IMO, it would NOT have produced enough blood to create what was seen by Perry and Baxter. If true, then lung damage MUST exist elsewhere. The only candidate for that is the entry wound at T3. I *think* you agree. Can you confirm or deny?
Hi Tom
I'm a bit on the fence with the throat wound, as I find it far more baffling than the back wound. But I agree with you. The apex of the right lung, as the diagrams show, is extremely close to the throat wound. It is not uncommon for the shock wave of a bullet passing through tissue to bruise tissue adjacent to the bullet path. Then again, the bruise at the apex of the right lung reported by Humes may be a total fabrication, or a downplaying and moving of much more extensive lung damage.
"Do you believe that the missile that bruised the lung (as described by Humes) produced ALL of the blood/air as described by Perry and Baxter (as seen through the trach incision)? "
No I do not, for three reasons.
1. Humes reported ONLY a small bruise to an otherwise intact lung.
2. Humes reported no collection of blood in the pleural cavity. In order to reach the mediastinum, the blood would have to pass from the pleural cavity, through the hilum of the lung, and OUTSIDE of the right bronchus.
3. Despite 1 & 2, there simply was not enough blood lost into the bruise at the apex of the right lung.
Once again, it is evidence vs. evidence, Bethesda vs. Parkland. Only one can be true.
-
Bob,
There certainly was damage to the upper portion of the right lung, but I'm undecided as to whether or not the pleura was penetrated. I'm not aware of any evidence stating that the cited damage at the apex of the right lung could only occur if the pleura was ruptured.
If the pleura was NOT damaged at the apex of the lung, then what you are saying can only be true IF there was significant lung damage elsewhere. Do you agree?
Also, IMO, the damage at the apex of the lung is associated ONLY with the throat wound, NOT the back wound. What is your position on this? If this is true then we have the entry wound in the back that due to its location MUST have caused SOME damage to the right lung. IMO this damage alone could have caused all of the symptoms as you have described.
Yes, that was my point and we are in agreement. Also, In this example I believe that ALL blood and escaping air REMAIN contained within the outer pleura. It seems virtually impossible that inflicting a "bruise" at the apex of the right lung would rupture enough blood vessels to create the situation as described by Perry and Baxter. I believe we are in agreement on this, also. It's been a LONG time since I've read these statements so I may be incorrect as to their blood/air descriptions.It is possible to have a tension pneumothorax without the parietal (outer) pleura having an opening in it. A classic example is a blunt blow to the rib cage severe enough to rupture the lung and visceral (inner) pleura surrounding the lung, but not severe enough to rupture the parietal (outer) pleura. This would prevent the lung from fully inflating, and allow air to escape through the damage in the lung into the pleural cavity outside of the lung.
If true, then a considerably more severe wound MUST exist elsewhere. Such as the acknowledged back wound that according to Humes did no lung damage at all.
Certainly not Gerald Ford, nor Humes veracity...If the back wound was moved from the level of T3, almost 6 inches below the collar line, to the level of C7, right at the collar line, what was to stop them from moving the damage in the lung upward as well?
The main point is that Humes never reported seeing a collection of blood in the pleural cavity between the parietal (outer) pleura and the visceral (inner) pleura that envelops the lung. All Humes reported was this nice intact right lung with a tiny 2 inch bruise at the apex, much higher than the entrance wound at T3 and even more impossible if you believe the bullet was travelling downward when it struck JFK.
Humes' report of an intact lung and pleurae is in total contradiction of the signs of right pneumothorax and hemothorax reported by Humes.
-
I think that James's theory, where the bruise to the right apical lobe is attributed to a bullet to the throat, is an interesting one. And is worthy of further study (though in another, dedicated thread).
James's theory requires that the throat wound be one of entrance. Which, I believe, requires that the location of the throat wound be above the shirtline. And this possibility has NOT been ruled out AFAIK. (Though there are some arguments against it.)
I currently believe that the throat wound is one of exit, and was probably made by a bone fragment. If true, Jame's theory would be invalid. So Robert's presentation here is of great interest to me.
It has been demonstrated to my satisfaction that Humes fibbed in his accounts when necessary. So if his account of something disagrees with others' accounts, I tend to question his first. Especially when it would make sense for him to fudge the story in order to support the lone nut theory.
I believe that Robert has demonstrated that pneumothorax did occur, and probably tension pneumothorax as well. He has indicated that a large amount of damage would have been required for that to have occurred. I confess that I would like to hear from some doctors on this point. Because I am wondering if the level of damage reported by Humes could have been sufficient to cause pneumothorax. If so, that could resolve some unexplained issues.
I'm glad that James reminded us of the triangle shaped damage described by Humes. I'd forgotten about it. In my opinion, Humes's detailed description of the damage's shape gives it some credibility. However, I wouldn't be surprised if Humes fibbed regarding the location of the damage. Apparently Robert feels the same, given that he said:
If the back wound was moved from the level of T3, almost 6 inches below the collar line, to the level of C7, right at the collar line, what was to stop them from moving the damage in the lung upward as well?
Here is a hypothetical summary of autopsy events that attempts to explain all the testimony regarding the autopsy:
- Humes sees the back wound and assumes a bullet penetrated the pleural lining.
- He removes the organs and sees the bruise on the pleura, and the triangular damage to the lung, at roughly the location of the back wound.
- He searches the organs for the bullet but cannot find it.
- He gives up and pretends to probe the back wound with his finger, and to probe the pleura. He proclaims that the bullet wound was shallow.
- What actually happened was that a frangible bullet hit the back, fragmented into particles, and many of these particles penetrated the pleural linings and the right lung. These particles show up on x-ray but are wrongly attributed to film cartridge dust.
- A rib took the bulk of the blow and absorbed most the kinetic energy. Only a small percentage of the bullet particles actually enter the lung. This explains the minimal damage to the lung.
Hi Sandy
Well, there's another way of looking at this.
A lot of people don't realize this but, the apex of the lung is much higher than most think, as these diagram show.

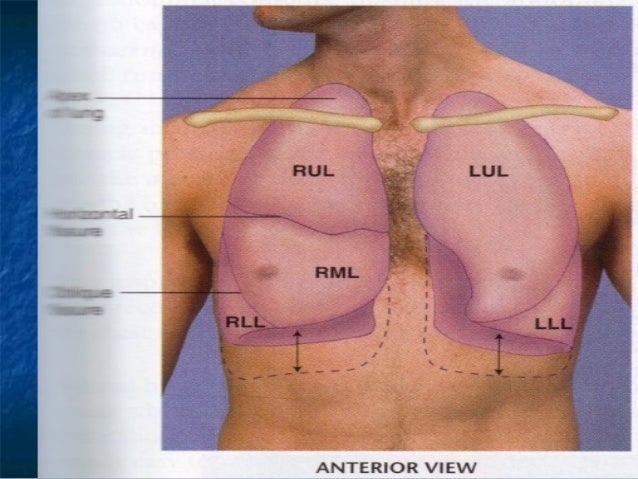
Do you see how far above the clavicle (collarbone) the apex of the right lung extends? If the widest part of the bruise was at the apex of the lung, and the bruise only extended 2 inches downward, and diminished drastically as it extended downward, wouldn't Humes be just a bit puzzled as to how a bullet entering at the level of T3 vertebra could do such damage, and not even make a hole in the outer pleural lining?
I have seen many lung shots on deer, and even a .22 Long Rifle bullet travelling through a lung makes a lot of very messy and very obvious damage. Humes had to know there was something fishy going on.
A rib is not a thick enough or heavy enough bone to absorb enough of a bullet's energy to make any difference in a wound in a lung. I have seen chest shots on deer where the bullet missed the rib and where the bullet struck the rib. The difference in damage is negligible. In fact, as in the case of John Connally, the shattering of the rib only serves to make more secondary missiles that go on to cause their own damage in the lung.
However, as none of JFK's ribs were struck by a bullet, we can only conclude a frangible bullet disintegrated into dust as it was travelling through his right lung.
-
Bob,
There certainly was damage to the upper portion of the right lung, but I'm undecided as to whether or not the pleura was penetrated. I'm not aware of any evidence stating that the cited damage at the apex of the right lung could only occur if the pleura was ruptured.
If the pleura was NOT damaged at the apex of the lung, then what you are saying can only be true IF there was significant lung damage elsewhere. Do you agree?
Also, IMO, the damage at the apex of the lung is associated ONLY with the throat wound, NOT the back wound. What is your position on this? If this is true then we have the entry wound in the back that due to its location MUST have caused SOME damage to the right lung. IMO this damage alone could have caused all of the symptoms as you have described.
Tom
Hi Tom
It is possible to have a tension pneumothorax without the parietal (outer) pleura having an opening in it. A classic example is a blunt blow to the rib cage severe enough to rupture the lung and visceral (inner) pleura surrounding the lung, but not severe enough to rupture the parietal (outer) pleura. This would prevent the lung from fully inflating, and allow air to escape through the damage in the lung into the pleural cavity outside of the lung. However, this kind of damage is almost guaranteed to rupture several blood vessels, and there will inevitably be an accumulation of blood in the pleural cavity, referred to as a "hemothorax" by Perry.
If the back wound was moved from the level of T3, almost 6 inches below the collar line, to the level of C7, right at the collar line, what was to stop them from moving the damage in the lung upward as well?
Correction: The ribs are outside of both pleura, and to tear the visceral pleura with a broken rib, it is necessary to first tear the parietal (outer) pleura. the only difference is there is no opening to the atmosphere from the pleural cavity, still making this a tension pneumothorax.
-
Bob,
Like Sandy I am not here to interrupt your thread which I find interesting. However, though I agree the right lung was indeed damaged, it was damaged at the top and not in the body of the lung. In a document I wrote about JFK's injuries I described this observation. It is a wonderful description by Humes. Senator Cooper asks him what was the character of this bruise at the top of the lung. Humes reply is wonderful and I am not sure he was fully aware of what he actually said. Below is the section describing this moment.
A few pages later, Senator Cooper interrupts Commander Humes and asks him what was the character of this bruise that he saw. Humes replies and in doing so describes just what an incredible anomaly this “bruise” was. This is just such an important point I will parse what he says.
First Commander Humes reply.
Commander HUMES. “The bruise here, photographs are far superior to my humble verbal description, but if I let my hand in cup shaped fashion represent the apical parietal pleura, it was an area approximately 5 cm. in greatest diameter of purplish blue discoloration of the parietal pleura. Corresponding exactly with it, with the lung sitting below it, was a roughly pyramid-shaped bruise with its base toward the surface of the upper portion of the lung, and the apex down into the lung tissue, and the whole thing measured about 5 cm., which is a little - 2 inches in extent, sir.” H2 369
a) First Humes describes the shape of the Apical Parietal Pleura.
“if I let my hand in cup shaped fashion represent the apical parietal pleura, it was an area approximately 5 cm. in greatest diameter of purplish blue discoloration of the parietal pleura.”
• So what he is saying is that the Apical Parietal Pleura was rounded like his cupped hand.
• He then says that this area of the Apical Parietal Pleura was bruised and the size of the bruise was 5cm.
• Then he describes the colour of the Pleura as purpilish blue.
Now this first reference of 5cm refers not just to the size of the Apical Parietal Pleura that was damaged but also the size of the base of the anomaly, which was underneath it.
Now Humes goes on to describe the shape of the anomaly.“Corresponding exactly with it, with the lung sitting below it, was a roughly pyramid-shaped bruise with its base toward the surface of the upper portion of the lung, and the apex down into the lung tissue, and the whole thing measured about 5 cm., which is a little - 2 inches in extent, sir. ”
a) “Corresponding exactly with it, with the lung sitting below it,” The “it” refers to the bruise on the Apical Parietal Pleura. He then says that the lung was positioned below the Apical Parietal Pleura .. as indeed it is.
“was a roughly pyramid-shaped bruise.”He now describes what the shape looked like. He likens it to a pyramid.
c) “with its base toward the surface of the upper portion of the lung.” Normally pyramids have their pointed portion facing upwards. However, this anomaly is actually upside down and it is the base, or bottom, which is facing upwards. However there is another point he makes here. Humes says that the base of this anomaly is towards the surface of the lung itself. Above the surface of the lung are the Apical Parietal Pleura, the Parietal Pleura and finally the Visceral Pleura. If the base is toward the surface of the lung, then it has to be below these three surfaces.
d) “and the apex down into the lung tissue.” The pointed end of this pyramid is not just facing downwards, with the use of the word “into” Humes is saying that this part of the anomaly is actually inside the actual tissue of the lung.
e) “and the whole thing measured about 5 cm., which is a little - 2 inches in extent, sir.” The use of the word “thing” refers to the shape of the anomaly. This part of the description has been about where the base of the anomaly was in relation to the top of it. Therefore this reference to 5cm, refers to distance between the base and the top. It is that which is 5 cm. Hence the anomaly is 2 inches tall. The first description of 5cm, although describing the area of the Apical Parietal Pleura that was bruised, is also describing the measurement of the base of the object that lies below it.
In his description Humes has just admitted that the right lung was damaged. He has said that:-
a) The base of this anomaly is towards the “surface of the upper portion of the lung.”
AND
“and the apex down into the lung tissue.” The top of this pyramid is inside the lung itself. He is therefore saying that the tissue of the lung has been pierced.What caused this damage is another matter. However, Humes is quite clear that the damage is at the top of the lung and not the middle and body of the lung. Unless you have evidence that I had been unaware of, there is no evidence that the body of the lung was damaged or pierced.
I disagree that the wound to the back was anything but a shallow wound. However I am not going to interrupt your thread by arguing my corner. Nor am I going to interrupt the thread by arguing where I believe the lung was damaged. However I did want to place my opinion into the record.
James.
Hi James
This is likely one of the best presentations of Humes describing the bruise at the apex (top) of JFK's right lung that I have seen to date. You have obviously spent some time studying this matter.
The only problems with linking this bruise to the suspected pneumothorax and hemothorax I have described in JFK's right pleural cavity are the extremely small size of this bruise and the fact that Humes does not describe it as anything more than a bruise. In his own words, the right lung was completely intact and there was no great accumulation of blood in JFK's right pleural cavity.
In order for Dr. Perry to be able to observe blood in the right mediastinum, from the perspective of an incision in the throat to gain access to the trachea, do you have any idea how much blood had to accumulate in the right pleural cavity, in order to leak out the right hilum of the lung and migrate out past the trachea wound? Where is Humes' account of the discovery of this accumulation of blood in the right pleural cavity?
If we are to take Humes strictly at his word, which you seem so inclined to do regarding the shallow back wound and the 5 cm. bruising of the top of the right lung, there would be no further injury to the lung than the bruising, and certainly no tension pneumothorax or hemothorax in the right pleural cavity. Humes' description of an intact pristine right lung and right pleural cavity simply do not jive with the signs of damage observed by Carrico and Perry. This is hardly surprising, though, as Humes' observations are in complete contradiction of everything else observed by the doctors at Parkland.
Why you continue to treat Humes' word as Gospel is beyond me, James.
-
Bob,
Like Sandy I am not here to interrupt your thread which I find interesting. However, though I agree the right lung was indeed damaged, it was damaged at the top and not in the body of the lung. In a document I wrote about JFK's injuries I described this observation. It is a wonderful description by Humes. Senator Cooper asks him what was the character of this bruise at the top of the lung. Humes reply is wonderful and I am not sure he was fully aware of what he actually said. Below is the section describing this moment.
A few pages later, Senator Cooper interrupts Commander Humes and asks him what was the character of this bruise that he saw. Humes replies and in doing so describes just what an incredible anomaly this “bruise” was. This is just such an important point I will parse what he says.
First Commander Humes reply.
Commander HUMES. “The bruise here, photographs are far superior to my humble verbal description, but if I let my hand in cup shaped fashion represent the apical parietal pleura, it was an area approximately 5 cm. in greatest diameter of purplish blue discoloration of the parietal pleura. Corresponding exactly with it, with the lung sitting below it, was a roughly pyramid-shaped bruise with its base toward the surface of the upper portion of the lung, and the apex down into the lung tissue, and the whole thing measured about 5 cm., which is a little - 2 inches in extent, sir.” H2 369
a) First Humes describes the shape of the Apical Parietal Pleura.
“if I let my hand in cup shaped fashion represent the apical parietal pleura, it was an area approximately 5 cm. in greatest diameter of purplish blue discoloration of the parietal pleura.”
• So what he is saying is that the Apical Parietal Pleura was rounded like his cupped hand.
• He then says that this area of the Apical Parietal Pleura was bruised and the size of the bruise was 5cm.
• Then he describes the colour of the Pleura as purpilish blue.
Now this first reference of 5cm refers not just to the size of the Apical Parietal Pleura that was damaged but also the size of the base of the anomaly, which was underneath it.
Now Humes goes on to describe the shape of the anomaly.“Corresponding exactly with it, with the lung sitting below it, was a roughly pyramid-shaped bruise with its base toward the surface of the upper portion of the lung, and the apex down into the lung tissue, and the whole thing measured about 5 cm., which is a little - 2 inches in extent, sir. ”
a) “Corresponding exactly with it, with the lung sitting below it,” The “it” refers to the bruise on the Apical Parietal Pleura. He then says that the lung was positioned below the Apical Parietal Pleura .. as indeed it is.
“was a roughly pyramid-shaped bruise.”He now describes what the shape looked like. He likens it to a pyramid.
c) “with its base toward the surface of the upper portion of the lung.” Normally pyramids have their pointed portion facing upwards. However, this anomaly is actually upside down and it is the base, or bottom, which is facing upwards. However there is another point he makes here. Humes says that the base of this anomaly is towards the surface of the lung itself. Above the surface of the lung are the Apical Parietal Pleura, the Parietal Pleura and finally the Visceral Pleura. If the base is toward the surface of the lung, then it has to be below these three surfaces.
d) “and the apex down into the lung tissue.” The pointed end of this pyramid is not just facing downwards, with the use of the word “into” Humes is saying that this part of the anomaly is actually inside the actual tissue of the lung.
e) “and the whole thing measured about 5 cm., which is a little - 2 inches in extent, sir.” The use of the word “thing” refers to the shape of the anomaly. This part of the description has been about where the base of the anomaly was in relation to the top of it. Therefore this reference to 5cm, refers to distance between the base and the top. It is that which is 5 cm. Hence the anomaly is 2 inches tall. The first description of 5cm, although describing the area of the Apical Parietal Pleura that was bruised, is also describing the measurement of the base of the object that lies below it.
In his description Humes has just admitted that the right lung was damaged. He has said that:-
a) The base of this anomaly is towards the “surface of the upper portion of the lung.”
AND
“and the apex down into the lung tissue.” The top of this pyramid is inside the lung itself. He is therefore saying that the tissue of the lung has been pierced.What caused this damage is another matter. However, Humes is quite clear that the damage is at the top of the lung and not the middle and body of the lung. Unless you have evidence that I had been unaware of, there is no evidence that the body of the lung was damaged or pierced.
I disagree that the wound to the back was anything but a shallow wound. However I am not going to interrupt your thread by arguing my corner. Nor am I going to interrupt the thread by arguing where I believe the lung was damaged. However I did want to place my opinion into the record.
James.
James
What do you make of the HSCA testimony of Lt. Richard Lipsey, in which he describes Humes et al spending a good portion of the autopsy dissecting chest and abdominal organs in search of a bullet or bullet fragments?
Also, how much damage do you believe the 5 cm. bruise reported at the top of JFK's right lung caused? Did Humes report rupturing of the visceral pleura and lung at the site of the bruise, or did he report the lung to be bruised but still intact, and capable of normal respiration?
-
If an animal is shot through the lungs or (God forbid) through the guts, there is NO mistaking the fact a bullet has passed through these organs. There will always be blood clotting along the track. The same goes for after the animal has been skinned. A bullet passing through a hind quarter, front quarter or other muscle tissue will leave a trail of blood clots and bruised tissue obvious for anyone to see.
My question is this: Unless Humes was a complete idiot, why would he be dissecting organs if there was absolutely no sign whatsoever that a bullet had passed through JFK's thorax or abdomen?
Bob,
Your analysis has me thoroughly convinced that the right pleural sack was indeed punctured. That being the case, it is reasonable to conclude the Humes did indeed see signs that a bullet, or something else (frangible bullet particles), had passed through. So that would explain his search for the bullet within the internal organs.
But there was that one technician who said he saw Humes push a metal probe up against an intact pleural lining. I don't remember the tech's name, but I'm pretty sure that he was a medical professional. It baffles me that he would talk as though the pleural lining was intact, but not make the point that, on the other hand, the lung had clearly been hit. Unless the lung didn't show as much damage as is typical.
I've wondered if a special bullet might have been developed specifically for shots to the thorax, designed to make numerous puncture holes in the pleural lining. And maybe also to pepper the lungs with particles. (I don't know how serious a condition a lung peppered with particles is compared to a collapsed lung.) But not exit the body so as to not risk injury to others.
This is the reason I wanted to know earlier if the shooter may have intentionally shot JFK in the back.
(BTW, don't assume that I am here only to interrupt and ask these questions. I am following your presentation carefully.)
This is a perfect example of the mixed bag of half truths and fabrications that came out of the autopsy that night.
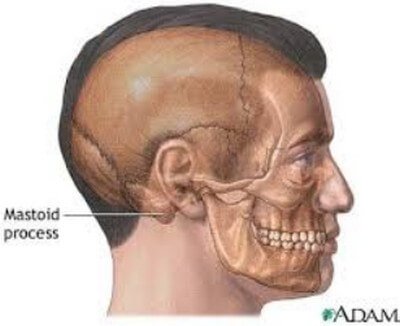
The mere fact this technician recalls seeing, from inside the chest cavity, a probe pushed up against an intact pleural lining is itself a contradiction of everything the autopsy results told us, placing the entrance wound on the back much lower than Humes stated. If the bullet entered JFK's neck where Humes claimed it did, 14 cm. (5.5 inches) below the mastoid process, there should not have been a wound track leading anywhere near the top of JFK's right lung or right parietal pleura.
"I've wondered if a special bullet might have been developed specifically for shots to the thorax, designed to make numerous puncture holes in the pleural lining. And maybe also to pepper the lungs with particles. (I don't know how serious a condition a lung peppered with particles is compared to a collapsed lung.) But not exit the body so as to not risk injury to others."
The problem with this theory is there is so little distance between the surface of the back, at the level of the T3 vertebra, and the parietal pleural lining that I cannot see how a bullet could make such a small entrance wound and be able to break up and spread out in such a tiny distance. Even if the lung was "peppered" with tiny particles, in order to produce the signs of pneumothorax observed by Carrico and Perry still requires considerable damage to the right lung, and this damage would have been quite obvious.
-
Okay, let's get back to looking for evidence of a tension pneumothorax in JFK's right lung by examining the testimonies of Drs. Carrico and Perry.
In my previous long post regarding Carrico's testimony, I showed that, after JFK was intubated with an endotracheal tube and hooked up to positive pressure ventilation via a respirator, Carrico listened to the air going into JFK's lungs and found that "Breath sounds were diminished, especially on the right....". The standard LN argument is that Carrico clumsily over inserted the endotracheal tube into JFK's left bronchus, but this was impossible, as air was leaking from the throat wound, and the only way this was possible was if Carrico accidentally placed the cuff ABOVE the wound in the trachea. With the cuff so high on the trachea, the tip of the endotracheal tube could be nowhere near the bronchi. Wit air leaking from the tracheal wound, there would be diminished breath sounds bi-laterally, but this does not explain the right breath sounds being more diminished. Conclusion: tension pneumothorax in JFK's right lung.
Just about the time Carrico was observing diminished breath sounds and air leaking out of the throat wound, Dr. Perry entered Trauma Room One and assumed control of JFK's airway. I would imagine there was a brief discussion between Carrico and Perry, with Carrico swearing he had placed the endotracheal tube cuff below the tracheal wound. It would have been very easy to tell Carrico to simply re-insert the endotracheal tube (again using the laryngoscope) and try to get the cuff below the tracheal wound on the second attempt. However, Perry seemed to be a quick thinker, and it likely occurred to him that the cuff of the e. tube was in its proper place below the tracheal wound, and the real reason that air was being lost out through the throat wound was that JFK's trachea was more damaged (and lower down) than Carrico had first surmised.
Time was extremely limited for JFK, and rather than waste time reinserting the e. tube, just to find that was not the problem, Perry elected to perform a tracheotomy on JFK's trachea. There were good reasons for doing so.
1. By exposing JFK's trachea, Perry could check for further damage, such as ruptured blood vessels or a second or third tear in the trachea below the one seen by Carrico.
2. The tip of the tracheostomy tube does not extend as far below its inflatable cuff as does the cuff on the endotracheal tube, allowing the tracheostomy cuff to be placed deeper in the trachea without overinserting the tip into one of the bronchi. If there was only one tear in the trachea (as there actually was), placing the tracheostomy through an incision made through this tear would guarantee the inflatable cuff would be below the tear.
When Perry made the incision in JFK's throat, exposing his trachea, he made one VERY important observation that pretty much means JFK had to have had a tension pneumothorax in his right lung:
"Mr. SPECTER - Dr. Perry, you mentioned an injury to the trachea.
Will you describe that as precisely as you can, please?
Dr. PERRY - Yes. Once the transverse incision through the skin and subcutaneous tissues was made, it was necessary to separate the strap muscles covering the anterior muscles of the windpipe and thyroid. At that point the trachea was noted to be deviated slightly to the left and I found it necessary to sever the exterior strap muscles on the other side to reach the trachea.
I noticed a small ragged laceration of the trachea on the anterior lateral right side. I could see the endotracheal tube which had been placed by Dr. Carrico in the wound, but there was evidence of air and blood around the tube because I noted the cuff was just above the injury to the trachea."The most important words in the above excerpt are
"At that point the trachea was noted to be deviated slightly to the left..."
Remember, in an earlier post, how I told you a tension pneumothorax in the right lung will cause a large volume of air to accumulate on the right side of the chest? And remember how I told you this building volume of air will put pressure on the heart, left lung and major blood vessels connected to the heart, to the point the function of these things will be impaired enough to kill the patient? Well, I neglected to tell you one small thing. Not only will a right tension pneumothorax exert pressure on the heart and left lung, it will also shift everything in the chest over to the left. As the trachea is in the chest, just below the larynx, it too gets shifted away from the affected side.
The universal sign of a tension pneumothorax, and this is taught to everyone from surgeons and nurses to the lowliest ambulance driver or first aid attendant, is deviation of the trachea AWAY from the side of the chest affected by the tension pneumothorax. There is NOTHING else a deviated trachea could be. The Lone Nutters will try to explain this away by claiming the wound on the right side of the trachea caused swelling on the right side of the trachea, and this pushed the trachea to the left, but this is absolute nonsense. If there was a hard bony structure up against the right side of the trachea, this might be possible. However, the trachea is out in the open, and this did not happen.
If there had been even ONE surgeon on the Warren Commission, and he was not bought or scared off, he would have pursued this obvious comment by Perry (along with several others) and there is a very good chance the Single Bullet Theory might never have come about. However, as we all know, no surgeons were asked to sit on the WC. Much better to have the fired head of the CIA.
So, Perry makes the incision in JFK's throat, and confirms that Carrico had placed the e. tube cuff too high, and that the e. tube was NOT overinserted into JFK's left bronchus.
"I noticed a small ragged laceration of the trachea on the anterior lateral right side. I could see the endotracheal tube which had been placed by Dr. Carrico in the wound, but there was evidence of air and blood around the tube because I noted the cuff was just above the injury to the trachea."
No doubt about it now. The greatly diminished breath sounds in JFK's right lung were from the built up air pressure of the right tension pneumothorax not allowing air into the right lung.
Perry describes what he did next:
"At that point I was down in the trachea. Once the trachea had been exposed I took the knife and incised the windpipe at the point of the bullet injury. And asked that the endotracheal tube previously placed by Dr. Carrico be withdrawn slightly so I could insert a tracheotomy tube at this level. This was effected and attached to an anesthesia machine which had been brought down by Dr. Jenkins and Dr. Giesecke for better control of circulation.
I noticed there was free air and blood in the right mediastinum and although I could not see any evidence, myself any evidence, of it in the pleura of the lung the presence of this blood in this area could be indicative of the underlying condition.
I asked someone to put in a chest tube to allow sealed drainage of any blood or air which might be accumulated in the right hemothorax.
This occurred while I was doing the tracheotomy. I did not know at the time when I inserted the tube but I was informed subsequently that Dr. Paul Peters, assistant professor of urology, and Dr. Charles Baxter, previously noted in this record, inserted the chest tube and attached it to underwater seal or drainage of the right pneumothorax."I noticed there was free air and blood in the right mediastinum....."
I don't imagine these words mean a thing to anyone reading this but, if you were an ER doctor, this would be one of the most important statements in Perry's entire testimony. The importance of this statement is revealed by what Perry stated he did following this observation, which we will examine shortly.
To understand the importance of this statement, let's take another look at this diagram:
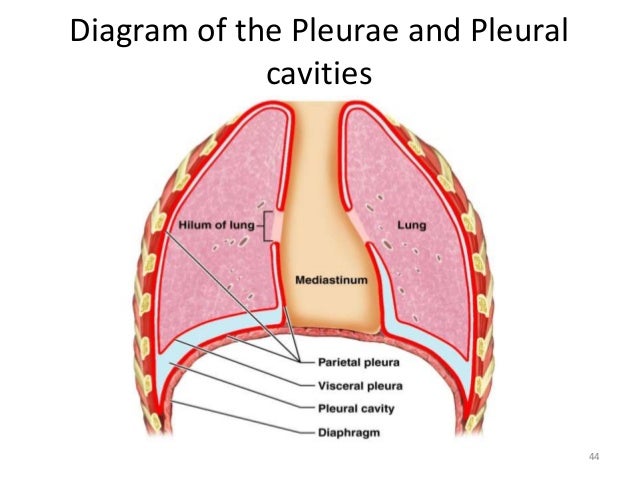
As can be seen, the pleural cavities are like two s contains the heartealed bags on either side of the chest and they are separated by a space called the "mediastinum". The mediastinum contains the heart and aorta, major veins (superior and inferior vena cava) pulmonary arteries and veins as well as the trachea. Within the mediastinum, the trachea splits into the two bronchi. Now, look closely at the inner walls of the pleural cavities, where they border the mediastinum, and you will see two openings known as the "hilum of the lung". This is the ONLY opening in the pleural cavity, and through this poorly sealed opening must pass the bronchi and pulmonary arteries and veins.
If the right lung were collapsed, and air pressure was building in the right pleural cavity, due to the use of the respirator, air would begin escaping between the inner side of the hilum and the bronchus and blood vessels passing through it. If blood was building up in the right pleural cavity (hemothorax) it too would escape out through the hilum. With JFK on his back, and his trachea exposed below the larynx, this blood and air would find its way out through this opening. The fact that Perry could see this, so shortly after the respirator was connected, is an indication of the amount of damage to the right lung.
So, seeing blood and air in the mediastinum, how did Perry interpret this? What measures did he undertake to deal with what he perceived?
"I noticed there was free air and blood in the right mediastinum and although I could not see any evidence, myself any evidence, of it in the pleura of the lung the presence of this blood in this area could be indicative of the underlying condition."
Notice Perry immediately makes the connection between air and blood in the mediastinum, and there being something wrong in the pleura (pleural cavity)? Care to guess what he meant by "the underlying condition"? Don't bother, Perry tells you in the next breath.
"I asked someone to put in a chest tube to allow sealed drainage of any blood or air which might be accumulated in the right hemothorax."
Not "suspected" right hemothorax or "possible" right hemothorax, but plain old right hemothorax. Perry was a good man, well trained in his profession, and he was responding instinctively to very obvious signs of a medical emergency in JFK's right lung. Now before anyone says, "Hey! Perry said hemothorax, not pneumothorax!" I would recommend you hold your water and read what Perry said in his next breath.
"This occurred while I was doing the tracheotomy. I did not know at the time when I inserted the tube but I was informed subsequently that Dr. Paul Peters, assistant professor of urology, and Dr. Charles Baxter, previously noted in this record, inserted the chest tube and attached it to underwater seal or drainage of the right pneumothorax."
At this point, Perry is calling it the right pneumothorax. I don't believe there was any doubt in Perry's mind at this point that, should JFK have lived, they would be doing emergency surgery on JFK's right lung. Imagine how puzzled Perry and the other Parkland doctors must have been when they learned that Humes and Arlen Specter had determined the bullet had missed the lung altogether!
Take note that, despite the insertion of left and right chest tubes at Parkland, Perry only requested the insertion of a right chest tube, as this was the side he observed the deficiencies on. Also take note that Perry states he was informed subsequently that Drs. Peters and Baxter not only inserted the chest tube, they also connected the tube to underwater sealed drainage. Would this statement not make a xxxx out of Humes, who testified that no chest tubes were found to be inserted at the autopsy, and that only shallow incomplete incisions had been made in JFK's chest? What reason would Perry and the other Parkland doctors have to lie about the chest tubes? Can we believe anything that came out of Humes?
Perry's final comment on the condition of JFK's right lung, followed closely by badgering from Specter:
"Mr. SPECTER - Now, you described a condition in the right mediastinum. Would you elaborate on what your views were of the condition at the time you were rendering this treatment?
Dr. PERRY - The condition of this area?
Mr. SPECTER - Yes, sir.
Dr. PERRY - There was both blood, free blood and air in the right superior mediastinum. That is the space that is located between the lungs and the heart at that level.
As I noted, I did not see any underlying injury of the pleura, the coverings of the lungs or of the lungs themselves. But in the presence of this large amount of blood in this area, one would be unable to detect small injuries to the underlying structures. The air was indicated by the fact that there was some frothing of this blood present, bubbling which could have been due to the tracheal injury or an underlying injury to the lung.
Since the morbidity attendant upon insertion of an anterior chest tube for sealed drainage is negligible and the morbidity which attends a pneumothorax is considerable, I elected to have the chest tube put in place because we were giving him positive pressure oxygen and the possibility of inducing a tension on pneumothorax would be quite high in such instances.
Mr. SPECTER - What is pneumothorax?
Dr. PERRY - Hemothorax would be blood in the free chest cavity and pneumothorax would be air in the free chest cavity underlying collapse of the lungs.
Mr. SPECTER - Would that have been caused by the injury which you noted to the President's trachea?
Dr. PERRY - There was no evidence of a hemothorax or a pneumothorax my examination; only it is sufficient this could have been observed because of the free blood in the mediastinum.Mr. SPECTER - Were the symptoms which excited your suspicion causable by the injury to the trachea?
Dr. PERRY - They were."
Good old Specter, faithful mutt right to the end.
Can you imagine yourself in Perry's shoes? He never got beyond performing a tracheotomy on JFK, and despite what he suspected was going on in JFK's right lung, without opening JFK's chest up, there was no way to confirm his suspicions. Then, of course, there is Specter pressuring him to state that all of the signs he observed were caused by the trachea wound. But, they weren't. Know why?
1. With the open wound in JFK's throat, how did free air accumulate in JFK's right superior (upper) mediastinum, nowhere close to the trachea wound? If the tracheal wound was connected through the throat wound to the outside air, would not any air from the tracheal wound simply escape, instead of building up in the mediastinum?
2. If enough blood accumulated to be observed in the right upper mediastinum, why was JFK's shirt collar and tie not soaked in blood on the trip to Parkland, while JFK was lying in the back seat of the limo? With the open wound in the throat, it would be very easy for this blood to escape out this wound. Could it be because the blood only escaped from the right pleural cavity, through the right hilum, when positive pressure ventilation from the respirator forced blood and air from his right pleural cavity?
Here is one exchange that was guaranteed to never have taken place:
"Mr. Specter: When JFK's right chest tube was connected to sealed drainage, what was the nature of the material being drained from JFK's right pleural cavity?
Dr. Perry: When the chest tube was first connected, there was a great escape of frothy red-tinged air escaping as the pressure from the pneumothorax was relieved. Once connected to sealed drainage, a mixture of air and blood continued to drain from the right pleural cavity."
-
Hi Sandy
I don't know if you've ever done much hunting or not but, for the benefit at least of those reading this that are non-hunters, I should explain something here that will make Humes' actions (or at least Lt. Lipsey's HSCA account of them anyways) appear utterly ridiculous, for a physician with any experience with gunshot wounds.
When you shoot an animal such as a deer for meat, it is necessary to disembowel and bleed the animal immediately, especially in warmer weather. The incision we make is on the belly; beginning at the genitals and ending at the bottom of the anterior ribcage. The colon is cut at the rectum and the entire abdominal contents (the "guts") are removed through this opening, with the oesophagus cut at the throat. Next, the diaphragm is carefully excised around the interior perimeter of the ribcage, the trachea is severed and the heart and lungs removed. At this point, the animal is ready to be hung by the back legs for skinning and quartering.
If an animal is shot through the lungs or (God forbid) through the guts, there is NO mistaking the fact a bullet has passed through these organs. There will always be blood clotting along the track. The same goes for after the animal has been skinned. A bullet passing through a hind quarter, front quarter or other muscle tissue will leave a trail of blood clots and bruised tissue obvious for anyone to see.
My question is this: Unless Humes was a complete idiot, why would he be dissecting organs if there was absolutely no sign whatsoever that a bullet had passed through JFK's thorax or abdomen?
-
Where is Lee Harvey Oswald when you need him?
 actually getting the bullet to its target.
actually getting the bullet to its target.
Why Humes Thought the Back Missile Hit at a Sharp Angle -- a Hypothesis
in JFK Assassination Debate
Posted · Edited by Robert Prudhomme
Ok, let's look at it from strictly the perspective of a bullet that would "fragmentize" in a wound, as O'Neill put it. There is no report from Humes about this bullet fragmenting completely in the shallow entrance wound in JFK's back. If it did, it would be a simple matter for Humes to recover the fragments from this entrance wound with a pair of tweezers, as the thickness of the back at this point from outside chest to pleural lining is only about an inch. They would also show up on an x-ray of the back or chest.
According to Humes, though, he did not find any fragments in this entrance wound. If the bullet "fragmentized", just where did it do so? Humes reported the pleural lining of the ribcage to be intact, with no bullet hole (or fragment holes) in it.
Do you see now how Humes painted himself into a corner?