

Robert Prudhomme
-
Posts
4,105 -
Joined
-
Last visited
Content Type
Profiles
Forums
Events
Store
Posts posted by Robert Prudhomme
-
-
Hello Bjorn:
Actually there is no "supposed to be" about the image - it is Connally's hat. What you have posted is an enlargement from one of two images taken by a local Dallas newspaper reporter/photographer. [i want to indicate it was Jack Beers, but I do not have my file in front of me at the moment; I am sure that Gary Mack will correct me on this if wrong]. This same reporter noticed the hat on a coat rack/tree in the corridor/hallway outside of Jessie Curry's office. The images were taken at approximately 8:00 p.m. CST on the evening of November 22, 1963. Curry confirmed for this same reporter that it was indeed Connally's hat. I do have the entire images in a file somewhere and if I can find them later I will post them. In 2004 I exchanged correspondence with a former member of Connally's staff who indicated that the hat was returned to Connally after his return to Austin from PMH in December of 1963. It was also indicated to me that Connally had the hat cleaned and is holding it in his hand in the infamous LIFE image from the 1967 "Why Kennedy Went To Texas" issue, but I have been unable to confirm this as true. What the photograph does appear to indicate is that the hat has no visible damage to it - i.e. "bullet" holes, something that this same employee stated was his observation as he handled the hat. However, as your enlargement does show, the hat is speckled with blood; whether this is the blood of John Connally or is from the fatal impact to JFK's head is not known.
Gary Murr
Considering he never let go of his hat on the way to PMH, even while unconscious, and he was wounded severely in the chest and forearm which would be in close proximity, one would suppose, to the hat, there is a remarkably minute amount of blood on this hat.
-
The hole in the cuff is indicative of a bullet entering sideways. The corresponding wound in JBC's right forearm, at 2.5 cm. (1 inch) x .5 cm., can be caused by nothing other than a tumbling bullet, unless, of course, a grenade went off close to JBC.
The exit hole in the shirt is not a very clean hole, either, and could be from a tumbling bullet or broken bone matter exiting along with the bullet.
People like to discuss the penetrating capabilities of a FMJ 6.5 Carcano bullet without realizing the variabilities that must be considered when such a bullet contacts irregularly shaped bones at oblique angles.
-
I was hoping the exhibit would include JBC's Stetson hat. Any idea what became of it?
-
Looks like Fritz walking behind him.
Coincidentally, the Model 8 had the same scope mounting problems as the 6.5 Carcano.
http://i1224.photobucket.com/albums/ee363/Traveller111/imagesCAZKM37L_zps863133af.jpg
-
Hard to say. He looks like a DPD detective.
Interesting bit of info from Wikipedia:
"The primary market for the Model 8 was sport hunting. The Model 8 was used as a police gun, modified to use detachable extended capacity magazines, among other changes. It is noted as the rifle of choice of famed Texas Ranger Frank Hamer.[4] Hamer's rifle was a customized .35 Remington Model 8 with a special-order 15 round magazine from Petmeckey's Sporting Goods store in Austin, Texas. He was shipped serial number 10045, and this was just one of at least two Model 8's used in the ambush of Clyde Barrow and Bonnie Parker.[4] The rifle was modified to accept a "police only" 20 round magazine obtained through the Peace Officers Equipment Company in St. Joseph, Missouri.["
-
It was a Remington Model 8, manufactured by Remington in the USA and by Fabrique Nationale of Liege, Belgium.
-
Seems to be a semi-automatic of some type. Reminds me of an old Fabrique Nationale (Belgian) I saw once.
-
One of the mantras chanted by the Lame Nuts is, "After 50 years, why hasn't someone with knowledge or evidence of a conspiracy spoken out?".
The truth of the matter is this, if I did not frequent the Education Forum on an almost daily basis, I would likely never have heard of Dr. Donald Teel Curtis, or have read an account of what he saw on 22/11/63.
People are speaking out but, if the MSM will not give them voice, who will hear them?
-
Hello Robert:
I thank you for taking the time to construct a thoughtful response to my posting. And while it is not my intent to debate the semantics of just what Dr. Gregory stated in the quote you posted - which is from Gregory's testimony session of April 21, 1964 - he did make a somewhat similar statement almost a month earlier on March 23, 1964, during his deposition session with the same Arlen Specter. At that time he phrased his description of the "wrist" wound in this manner:
MR. SPECTER. What did you observe with respect to the wound of his wrist?
DR. GREGORY. I didn't see the wound of his wrist until after the chest operation had been completed, because his arm was covered by the operation drapes, the surgical drapes for the chest procedure.
MR. SPECTER. And when you did have the opportunity to observe the wound of the wrist, what then did you see?
DR. GREGORY. I observed the wound on the dorsal aspect of his wrist, which was about 2 cm in length, ragged, somewhat irregular, and lay about an inch and a half or two inches above the wrist joint. It was a little to the radial side of the wrist area. There was a second wound in the wrist on the volar surface, about a centimeter and a half proximal to the distal flexion crease and this wound was a transverse laceration no more than a centimeter in length and did not gape.
MR SPECTER. When you say on the dorsal aspect, what is that?
DR. GREGORY. In lay terms thats equivalent to the back of the hand.
MR. SPECTER. And the volar is equivalent to what?
DR. GREGORY. The palm surface of the hand. [4H97-98]
I find it interesting that in describing the "wrist" wound of entrance Dr. Gregory while indicating this entrance point was on the dorsal aspect [not dorsal surface] of the wrist the doctor also indicates that this same entrance aperture was a "little to the radial side of the wrist area." Again, we can argue semantics all we want, but my interpretation of this deposition description is an attempt on Dr. Gregory's part to indicate to Specter that the entrance wound was not directly on the dorsal aspect/"back of the hand" -his afformentioned "lay terms" - but rather lay a little on/to the side of the fractured right radius, as Gregory drew it on his post-op note sheet. This description by Dr. Gregory mirrors what the doctor wrote on the same sheet of his handwritten post-op notes, which were constructed in point form and I list them below as he wrote them, complete with the doctors abbreviations etc.:
Op note: -
Open, comminuted fracture of the R radius - distal 1/4 due to missile wound.
- wound of entry 2 cm x .5 cm, oblique, radial, side
- wound of exit 0.5 cm - mid line, 2 cm proximal to flexion crease of wrist
And I agree wholeheartedly with you when you indicate that irrespective of interpretation, John Connally's wrist wound "does not bode well for Specter's SBT." It never did, and it never will. And of course this little discussion is but the tip of the colloquial iceberg when it comes to the wounding of John Connally.
FWIW
Gary Murr
Hello Gary
To this point, I had not read Dr. Gregory's post-op notes, in which he had written "wound of entry 2 cm x .5 cm., oblique, radial, side". This is somewhat of a revelation, as it is in direct contradiction to the testimony he presented to the WC. Describing a radial wound (wound to the radius bone) as "side" can only be interpreted as an anterior lateral wound to the radius.
Just to be clear, a doctor describing the "dorsal aspect" of the wrist translates to the same thing as the dorsal surface being described. Dr. Gregory confirms this by equating the dorsal aspect to the back of the hand, in lay terms, and by locating the dorsal wound "a little to the radial side of the wrist"; still placing the wound well onto the dorsal surface. Actually, "a little to the radial side of the wrist" is quite an understatement, considering the bullet struck the radius square on. How could the bullet possibly get closer to the radial side of the wrist than that?
Seeing contradictions between the post-op notes and the testimony given to the WC by Dr. Gregory reminds me of how many doctors, and other medical personnel, described a large gaping wound to the right rear of JFK's head in their first day notes and remembrances, only to have their memories "improve" by the time they testified to the WC.
As we both see quite clearly, locating the wrist wound in the dorsal lateral or anterior lateral area of JBC's wrist makes no difference; upon close examination, both locations present impossibilities for Specter's SBT.
-
I am very pleased that Gary has posted this Charles Gregory drawing. I have had it for some time but left it to Gary when he wanted to post it or use it.
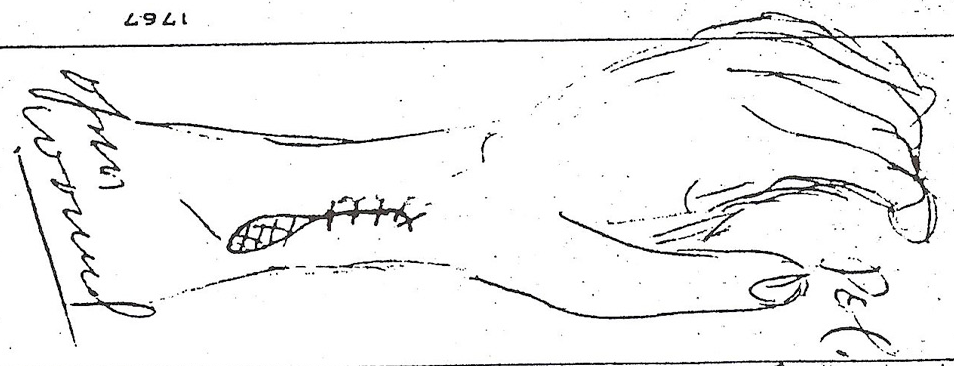
It is impossible to over emphasise the importance of this drawing. As Gary pointed, Charles Gregory is not suggesting that it was John Connally’s left hand that was injured. He used his own left hand to model the damage on John Connally’s right hand.
Unless there are members who insist on being obstinate, there now can be no dispute as to where this bullet entered John Connally’s right wrist. As I have pointed out above this bullet exited on the Volar side, i.e. the palm side.
Charles Gregory wrote his medical report in the afternoon after he completed his surgery of Connally’s wrist. As I recollect it was written even before Air Force 1 landed at Andrews Air Force base.
The importance of this drawing, especially for L/N’s, is how could the SBT, being fired from the rear, enter this wrist – where Gregory describes it does – and somehow exit through Volar or palm side of the right hand. And of course, at the point this is happening John Connally has the palm of his hand against his chest.
If the SBT is such a clear description of fact ( as L/N’s enjoy informing us ), then it should not be too difficult to explain how the bullet does that before going on to injure John Connally’s left thigh.
James.
At the risk of being "obstinate", there are a couple of things troubling me with regards to the description of JBC's forearm entrance wound location as "anterior lateral", as is clearly shown in the drawing with the red dot locating the site of the entrance wound, shown below:

There is no doubt that this drawing depicts an anterior lateral entrance wound, and it would be quite possible for JBC to have had his forearm in this position at the moment the SBT was to have occurred. However, there is a problem here, and that problem is that Dr. Gregory, in his testimony to the WC, never described this wound as "anterior lateral". Here is an excerpt from his testimony:
"Mr. Specter. Now what did you observe with respect to the wound on the Governor's wrist?
Dr. GREGORY. I did not have an opportunity to examine the wound on the Governor's wrist until Dr. Shaw had completed his surgical treatment of the Governor's chest wound.
At that time he was turned to his back and it was possible to examine both the right upper extremity and the left lower extremity for wounds of the wrist and left thigh respectively.
The right wrist was the site of a perforating wound, which by assumption began on a dorsal lateral surface. In lay terms this is the back of the hand on the thumb side at a point approximately 5 centimeters above the wrist joint.
There is a second wound presumed to be the wound of exit which lay in the midline of the wrist on its palmar surface about 2 centimeters, something less than 1 inch above the wrist crease, the most distal wrist crease."
So, he describes the entrance wound as on "....a dorsal lateral surface. In lay terms this is the back of the hand..." I am a part time paramedic with BCAS and although I am not nearly as qualified as a teaching surgeon such as Dr. Gregory, I have been taught to accurately describe wound locations. If someone told me the wound was on the "back of the hand" and was on "a dorsal lateral surface", I would be checking the back, not the lateral, surface of the wrist; either directly over the ulna (posterior) or over the radius (anterior). In my opinion, Dr. Gregory is describing a wound with the back side of the wrist squarely facing JBC's chest.
Either way, it does not bode well for Specter's SBT. If the wound was on the dorsal side of the wrist, the bullet could not have come from the rear (JBC's chest) as it would be impossible for him to have his forearm in that position.
If the bullet struck the lateral edge of JBC's forearm (striking the radius bone quite squarely), as Mr. Murr presents to us, what path did it then take to allow it to pass between the radius and ulna bone and exit the palm (volar) side of JBC's forearm in the midline of this surface? Did it pass through the radius? How then did it make a 90° turn to allow it to pass between the radius and the ulna? If so much energy had been robbed from this bullet by striking the radius that it was nearly spent, as we are told by the LN, wouldn't it simply come up against the ulna bone and stop there?
-
David Von Pein made the following point.
“A bullet that was almost completely out of gas hit that thigh.”
Until I saw the 2013 Nova program I might well have agreed with him. However Nova made clear that David’s statement is complete and utter nonsense. And that is not a comment of disrespect but fact. They were able to demonstrate that a Mannlicher Carcano bullet had the power to go through, I believe, 13 slats of pine. And what is even more amazing still be intact.
Staying with the SBT, from JFK’s entrance wound to Connally’s wrist wound the only bone the bullet actually strikes is Radius bone. The bullet does not strike the 5th rib, it knocks into it from its side.
Therefore, unless David can cast doubt on the experiment on Nova, carried out by Lucien Haag, and demonstrate it is invalid then the idea that the Single bullet that can successfully pass through 13 slats of wood would be out of power having only struck the radius bone, it is clearly very wrong to suggest that the bullet was out of “gas” by the time it struck the thigh.
Robert Prudhomme made the following point.
“Enlarging this x-ray photo will help you to see that the radius bone (right side of right photo and same side as thumb) was not actually hit squarely by a bullet. In fact, the radius bone was hit more on the edge AWAY from the gap between the radius and ulna bones, yet somehow, CE 399 was able to pass BETWEEN the radius and the ulna. Did it put itself in reverse, back up two inches, and take another run at the gap between the bones? Enlarging this x-ray photo will help you to see that the radius bone (right side of right photo and same side as thumb) was not actually hit squarely by a bullet. In fact, the radius bone was hit more on the edge AWAY from the gap between the radius and ulna bones, yet somehow, CE 399 was able to pass BETWEEN the radius and the ulna. Did it put itself in reverse, back up two inches, and take another run at the gap between the bones?”
Robert makes the point I have also, at times, directed at David Von Pein and which he also ignored.
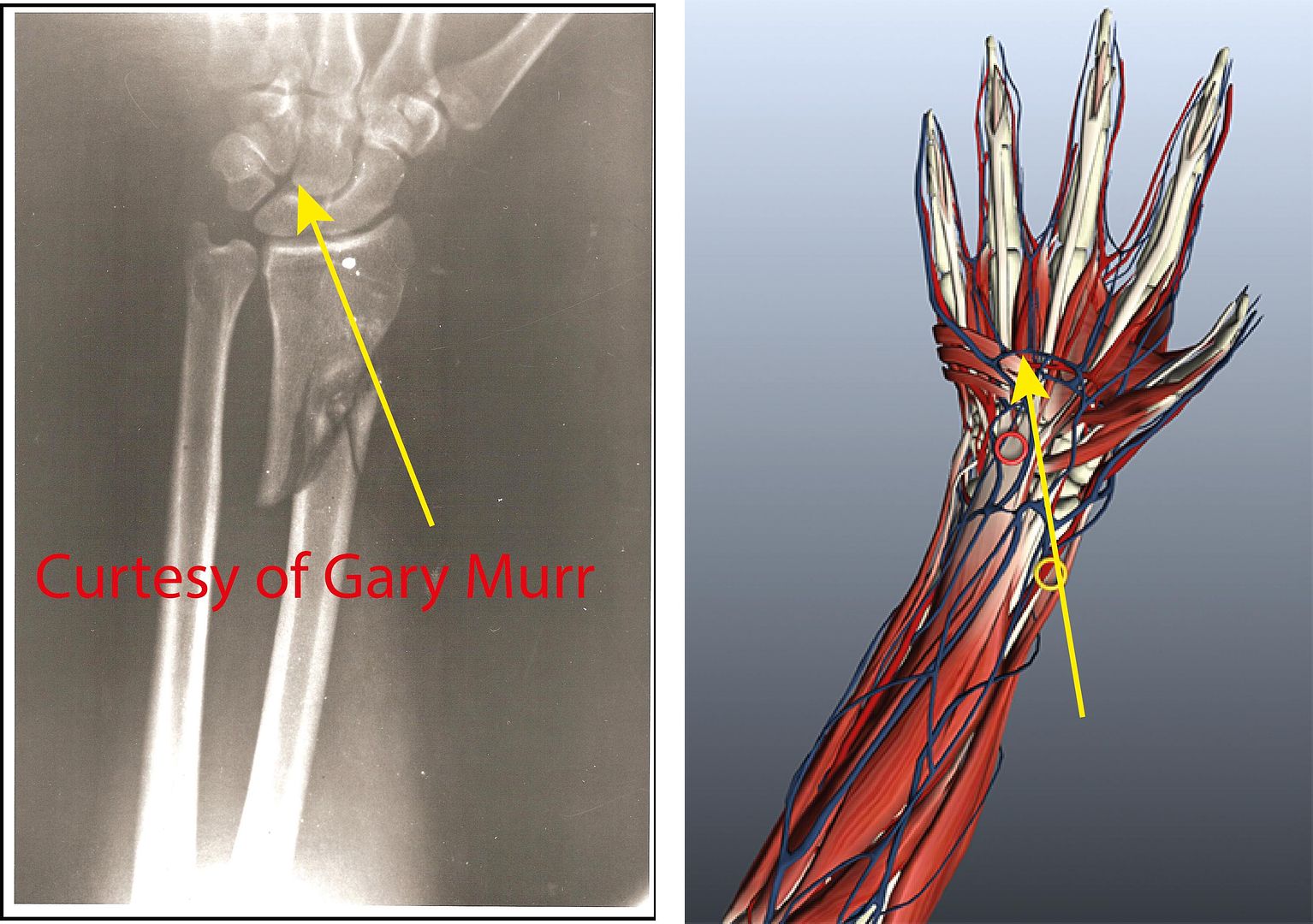
In lay language this bullet struck just behind the thumb on Dorsal side of the right hand. On the 3D model of the hand this is illustrated by the yellow circle. It exits on the palm side, or Volar side, around the middle of the wrist. In exiting in that position what the bullet has done is to separate the Hamate bone from metacarpal 5, which can be seen on the x-ray
The point that Robert makes, that is spot on, is if the bullet entered just below the thumb why does it not exit out the Dorsal side, the back of the hand? That is how Nova 2013 shows the exit. It should have exited out the Volar side.
Now why is Robert’s point so important and why did David ignore him? Because at this point the palm of the right hand, the Dorsal, was towards Connally’s chest.
So if the Single Bullet theory correctly follows the injuries sustained by John Connally, then it should have entered on his Dorsal just below the right thumb and exited in the middle of the Volar………………..
and then re-entered John Connally’s chest!!!!!!
Now that really is a magic bullet.
James.
Excellent post, James, and thank you for stating so simply and eloquently what I often find difficult to express.
I believe the wound to JBC's wrist to be the least studied aspect of the entire SBT debacle yet, in its simplicity, it has the potential to destroy Arlen Specter's mythology.
When pressed by Arlen Specter, Dr. Gregory adamantly states the path of the bullet to be from the back side of JBC's wrist, between the radius and ulna bone and exiting the volar or palm side of JBC's wrist. He has many reasons for believing this, including material from JBC's suit dragged into the wound. His WC testimony may be read here:
http://www.maryferrell.org/mffweb/archive/viewer/showDoc.do?docId=34&relPageId=126
As James points out, this is a trifle difficult, as the palm side of JBC's wrist was facing JBC's chest when the bullet exited his chest. Even if there had been no film footage of JBC at this moment, the simple fact of the matter is that no one, unless severely double jointed in the elbow, can hold his wrist at chest level and rotate his forearm backwards to the point the back of his wrist is facing his chest.
What is puzzling is that Dr. Gregory, in his testimony, endorses Specter's theory that a bullet exiting JBC's chest could enter the back of his wrist and exit the palm side of his wrist. Dr. Gregory has clearly not thought this through and seen the impossibility of this scenario OR he is another witness pressured into endorsing Specter's SBT theory. Either way, it does not matter; holding the back of the wrist flat to the chest cannot be done.
This is the one glaring defect of the SBT, and numerous Lame Nut cartoons, such as Nova 2013, have attempted to evade this problem by showing CE 399 entering the palm side of JBC's wrist and exiting the back of his wrist, as James pointed out. This type of deception is typical of the LN crowd.
-
Could you explain to me how CE 399 was able to strike the radius bone so squarely, yet be able to have enough velocity left to pass cleanly between the radius and the ulna and penetrate JBC's left thigh?
And just how much velocity do you think it would take to enter JBC's thigh (but not strike the femur beneath the skin)?
The thigh wound was quite superficial. A bullet that was almost completely out of gas hit that thigh. (Unless you'd like to theorize that a small fragment from the JFK head shot caused Connally's thigh injury. But in such a case, where did the bullet go that just exited Connally's wrist? Did it just disappear?)
There is no argument you can make that diminishes the validity of the Single-Bullet Theory. None.
IOW, every argument that anyone makes in favor of some OTHER theory to explain the non-fatal wounds to JFK & JBC can always be amply countered by an argument that makes much more sense.
A perfect example being the conspiracy theory that has three different bullets striking JFK and John Connally (none of which is CE399, naturally), with all three of these bullets just vanishing, including TWO missiles in JFK's neck and back--even though neither of those bullets made a journey into his body of more than just a few measly inches.
(See what I mean?)
Dave
I think Blair is way off in his nicknames for you. He should be calling you the Artful Dodger.
You have completely ignored the main point of my question, which is typical of an evasive person such as yourself; especially when cornered with a difficult question.
Now, once again, let us look at the x-ray:

Enlarging this x-ray photo will help you to see that the radius bone (right side of right photo and same side as thumb) was not actually hit squarely by a bullet. In fact, the radius bone was hit more on the edge AWAY from the gap between the radius and ulna bones, yet somehow, CE 399 was able to pass BETWEEN the radius and the ulna. Did it put itself in reverse, back up two inches, and take another run at the gap between the bones?
As CE 399 did not fully penetrate and pass through the radius bone, and as this was never claimed by the WC, looking at this x-ray could only lead one to believe the bullet was stopped at the radius bone and either fell out in the limo or at the hospital.
And you ask, where did the bullets go? Maybe you should tell us. The limo was a crime scene, and was violated by the Secret Service and God only knows what other branch of the government.
bump just for Dave
-
Baron Von Painhausen has run away.

Sir:
He has not "run away"; rather, he has made a strategic withdrawal from the field.
*SNICKER*
-
".....When Danger reared its ugly head....Dave bravely turned his tail and fled.......Running away and buggaring off....He is David, brave Sir David......."
(apologies to Monty Python and the Holy Grail)
-
And you ask, where did the bullets go? Maybe you should tell us. The limo was a crime scene, and was violated by the Secret Service and God only knows what other branch of the government.
Yep. Let's blame the Government for everything. That's always a good fall-back. Right, Bob?
Funny, isn't it, that the HSCA saw those same X-rays that Bob is looking at, and the HSCA had no problem at all accepting the fact that CE399 did, indeed, go through JFK and Connally.
Maybe I should cry "Doesn't prove a damn thing, Davey! Those guys were on the Government payroll! So of course they're all liars!
As usual, Dave, you have nothing to say. Please try to stay on topic and explain the magical feats performed in JBC's right forearm by CE 399. Unless, of course, you have no explanation.
-
Could you explain to me how CE 399 was able to strike the radius bone so squarely, yet be able to have enough velocity left to pass cleanly between the radius and the ulna and penetrate JBC's left thigh?
And just how much velocity do you think it would take to enter JBC's thigh (but not strike the femur beneath the skin)?
The thigh wound was quite superficial. A bullet that was almost completely out of gas hit that thigh. (Unless you'd like to theorize that a small fragment from the JFK head shot caused Connally's thigh injury. But in such a case, where did the bullet go that just exited Connally's wrist? Did it just disappear?)
There is no argument you can make that diminishes the validity of the Single-Bullet Theory. None.
IOW, every argument that anyone makes in favor of some OTHER theory to explain the non-fatal wounds to JFK & JBC can always be amply countered by an argument that makes much more sense.
A perfect example being the conspiracy theory that has three different bullets striking JFK and John Connally (none of which is CE399, naturally), with all three of these bullets just vanishing, including TWO missiles in JFK's neck and back--even though neither of those bullets made a journey into his body of more than just a few measly inches.
(See what I mean?)
Dave
I think Blair is way off in his nicknames for you. He should be calling you the Artful Dodger.
You have completely ignored the main point of my question, which is typical of an evasive person such as yourself; especially when cornered with a difficult question.
Now, once again, let us look at the x-ray:
Enlarging this x-ray photo will help you to see that the radius bone (right side of right photo and same side as thumb) was not actually hit squarely by a bullet. In fact, the radius bone was hit more on the edge AWAY from the gap between the radius and ulna bones, yet somehow, CE 399 was able to pass BETWEEN the radius and the ulna. Did it put itself in reverse, back up two inches, and take another run at the gap between the bones?
As CE 399 did not fully penetrate and pass through the radius bone, and as this was never claimed by the WC, looking at this x-ray could only lead one to believe the bullet was stopped at the radius bone and either fell out in the limo or at the hospital.
And you ask, where did the bullets go? Maybe you should tell us. The limo was a crime scene, and was violated by the Secret Service and God only knows what other branch of the government.
-
Hi Dave
If you wish to discuss WC evidence, let us look at an x-ray of JBC's right forearm:
http://www.maryferrell.org/wiki/images/9/97/Photo_hsca_ex_85.jpg
Could you explain to me how CE 399 was able to strike the radius bone so squarely, yet be able to have enough velocity left to pass cleanly between the radius and the ulna and penetrate JBC's left thigh?
-
*once again, the lonely sound of crickets chirping*
-
How do we know the French president had not been stating this for years but, like most revelations in the JFK assassination, it somehow did not make it into the news?
-
Mr. Hocking, surely you are not saying the Babushka Lady's film might be presented to us in a *GASP* altered form??

-
There is also the fact that, the new up and coming event since the 50th anniversary has
come and gone, that 2017 is the date, all the remaining JFK files are slated to be released.
more.....
http://www.theindychannel.com/news/u-s-world/five-decades-later-some-jfk-probe-files-still-sealed
excerpt
Congress passed the President John F. Kennedy Assassination Records Collection Act of 1992, which established the Assassination Records Review Board, or ARRB, to carry out release of records. As a result, about five million pages of documents have been released and are available for review at the National Archives and Records Administration in Maryland.
But the review board agreed to withhold about 1,100 records - each record comprises 1-20 pages - that are considered to contain information about confidential sources or methods or have national security implications.
The JFK Act required all records to be released by 2017, but it left some wiggle room for agencies to petition to have records withheld if disclosure would compromise "military defense, intelligence operations, law enforcement, or conduct of foreign relations."
It is unknown whether the CIA will try to keep some documents classified past 2017; if it does, that may only increase Morley's resolve.
"You have to wonder what is so important in a 50-year-old document," he said. "I've come to the conclusion that they're guarding something big, and that has stiffened my determination."
A CIA spokesman, Ned Price, said the agency has complied with the law in releasing documents and the archives center "has all of the Agency's documents and files on the Kennedy assassination. Price didn't comment on the Joannides material specifically, citing Morley's lawsuit.
"The classified information contained in the files remains subject to the declassification provisions of the Act," he said.
Meanwhile, the documents sit in metal boxes on shelves in "a big room that's temperature- and humidity-controlled," said Martha Murphy, the Archives' chief of special.......
I hope the film from the Babushka Lady's camera is in those 1,100 records.
-
*crickets chirping in the ensuing silence*
-
I just realized it is November 23 and we haven't all dried up and blown away, as the Lame Nuts predicted we would.
-
look at these clowns fondling the evidence...
i know it was 1963 and in nut country, but Perry Mason had been on tee vee how long at this point?
and there is the four foot bag again...
I've always wondered what is keeping the bag upright in that photo.





{kind=link}
Oswald Leaving TSBD?
in JFK Assassination Debate
Posted
I just figured it all out! LHO shot JFK with venetian blinds!