

Robert Prudhomme
-
Posts
4,105 -
Joined
-
Last visited
Content Type
Profiles
Forums
Events
Store
Posts posted by Robert Prudhomme
-
-
Frangible bullets would have been used for two reasons. 1. As they are designed to disintegrate to powder after travelling through semi-liquid matter and flesh a couple of inches, they transfer all of their energy to surrounding tissue and have the potential to be more lethal than any other bullet, except perhaps an exploding bullet. 2. Frangible bullets not only disintegrate to powder inside of a wound, they also disintegrate if they hit something hard like steel or concrete.This would tend to keep collateral damage to a minimum. 3. The general characteristics of a frangible bullet jacket are very similar to a full metal jacket bullet jacket, to the point where someone finding a piece of bullet jacket on Elm St. would be unable to identify it as a frangible bullet jacket, unless he knew what to look for.
I think your frangible bullet scenario makes a lot of sense, particularly given that Kennedy had a punctured lung seeming to have come from the back wound, yet no noticeable puncture through the pleura.
I think a tiny fragment must have punctured the pleura. (Please let me know if there's a problem with this statement.)
If it can be shown or reasoned that the velocity of a standard bullet would have been much less than the 380 fps in my analysis -- say below 250 fps -- then I would definitely favor your theory over the one I adopted from Purvis. Your comment on the speed of Ruby's bullet sank in after all.
Well, the problem is that I doubt any bullet, even a frangible bullet, would break apart after only penetrating an inch in flesh and then stopping. Frangible bullets require much more velocity and travelling through a few inches of flesh, lung or brain matter to make them break up. Of course, I have no idea how a frangible bullet would have been constructed in 1963, and I won't discount the possibility of a particle of that bullet escaping.
But I thought it was your belief that a frangible bullet is what caused the back wound. I thought that that was how you explained that there were no fragments found. Now you're saying you doubt that could be the case because the bullet wouldn't fragment.
Please explain. Maybe I misunderstood or read too much into what you said.
Also, wasn't your point, when posting the testimony about the collapsed lung, to support the idea of a bullet particle having passed through the pleura? (I don't remember your actually stating that. But there had to have been some point in posting that information. I suppose.)
This is going to get very technical but I will try to simplify things as much as possible.
It may sound odd but, in order to understand how a frangible bullet functions in a wound, it is necessary to first understand how a hollow point bullet functions in a wound.


Winchester "PDX1 Defender" 7.62x39mm 120 grain hollow point.
As you know, the bullets fired at JFK were supposed to have been FMJ bullets, possessing a bullet jacket that completely envelops the nose of the bullet. This type of bullet is universally banned for hunting purposes for one simple reason. It is extremely resistant to expansion in a wound, and has a tendency to pass straight through its intended victim instead of opening up and inflicting mortal damage.
On the other end of the spectrum are hollow point bullets. These bullets expand so well in wounds, new designs, such as the PDX1 Defender above, possess features that limit the expansion of these bullets to a point midway down the bullet.
Two important things to know about hollow points. 1. They will not "explode" on the outer surface of the skull in a head shot. I have taken head shots on deer with hollow point bullets, and they make the same tiny entrance wound through skull bone as any other bullet does. 2. The forces that cause a hollow point bullet to open up and expand work better in soft tissue, such as brain, lung or other organs.
Here is how they work. Let us say a hollow point bullet enters the skull at 2000 fps, making an entrance wound through the skull bone not much larger than the diameter of the bullet, and retaining the majority of its velocity (and energy) once inside the skull. As it passes through semi-liquid brain matter, the tiny cavity at the nose of the bullet fills up with semi-liquid matter and begins exerting an enormous hydraulic pressure on the interior walls of this tiny cavity. This hydraulic pressure causes the soft hollow point to begin opening up, allowing the hollow point to capture even more semi-liquid material and exert even higher pressures on the interior of the bullet. Within a couple of inches, it often will look like this:

6.5x55mm Swedish hollow point bullet before and after firing. This bullet possesses expansion limiting features that do not allow the opening up of the nose of the bullet past the point seen above. Without this, this bullet would have likely fragmented into many pieces.
Of course, as the bullet opens up, the surface area of its face gets larger and creates more drag passing through the brain, slowing the bullet down and creating a large pressure wave ahead of the bullet, often to the point the bullet will come to a complete halt and transfer all of its energy to surrounding tissue. This transfer of energy, plus the pressure wave, is what creates the massive amount of damage in a head wound. Often, the pressure wave is so great, a large section of skull will be blown out, and not always in line with the path of the bullet. Nor does the bullet have to exit to create such a blowout.
Modern lethal frangible bullets are essentially jacketed hollow point bullets with one major difference. Instead of a solid lead core, they use something completely different.
The core of a frangible bullet begins as lead (or other metal) powder. This metal powder is then formed into the shape of a bullet and either compressed by several thousand pounds of pressure or glued or sintered until it becomes a solid bullet. This bullet is then encased in a hollow point copper alloy jacket.

Dynamic Research Technologies frangible hollow point bullet in cartridge, calibre unknown. Note the hollow point opening on the tip of the bullet. http://www.drtammo.com/DRT-Technology
When the frangible bullet is fired at the skull of a game animal, it makes the same tiny entrance wound as the other bullets. As it passes through the semi-liquid brain matter, the hollow point opening fills up with fluid the same as the hollow point bullet, and the fluid exerts the same massive hydraulic force on the core of this bullet. This time, instead of just expanding, the massive hydraulic pressure exerts enough force to cause the compressed metal core to disintegrate back into a cloud of powdered metal; stopping the bullet instantly and transferring ALL of its energy to surrounding tissue. Needless to say, the results are devastating, and qualify these bullets as some of the most lethal bullets on the market.
So, getting back to the back wound, if the frangible bullet had "come apart" in the shallow back wound, there would have been much more damage visible than just a tiny entrance wound. I am saying the entire bullet went through the pleura and entered the lung, disintegrating there. Remember the hundreds of tiny metallic particles seen in the x-rays of JFK's skull? Obvious evidence of a frangible bullet that has disintegrated.
-
Tom's description:
This is the kind of nonsense I was speaking of. According to Tom, if you shoot a rifle sighted in at 100 yards, any shot less than 100 yards will impact lower than the line of sight.
Crap!
Look at this diagram:

As can be seen, the line of sight (through the scope) is slightly higher than the tip of the barrel. Once the rifle is sighted in at the target, the barrel will be tilted up slightly, so that the bullet will follow a parabolic curve that crosses the line of sight first just a few feet out from the end of the barrel, and again at the target.
Anywhere in between these two crossing points, the bullet will be higher than the line of sight, and impact a target higher than what the shooter is aiming at. To hit a target at 50 yards, the shooter, if the rifle is sighted in at 100 yards, must aim slightly low on his target.
This is further exacerbated by the fact it was downhill from the 6th floor to the limo, and a bullet will always impact higher than the aiming point when shooting downhill (or uphill).
-
The only footage I have that tries to replicate.
https://spideroak.com/browse/share/JFKFILES/JFKVIDEOS
Password: assassination
chris
Shoot! I couldn't get the audio to work when I watched the video. Oh well, no matter.
When we were discussing branches, I was thinking about something a little more substantial than those "twigs" they had set up there. I seriously do not think passing through those little things is going to rob the bullet of 1700 fps. But what do I know, eh? I'll tell you one thing, though. That bullet had a serious yaw to it and had definitely not lost much of its original velocity. I wonder how many shots it took until they had one that wasn't tumbling?
Something else to think about. If Tom Purvis reported his bullets were flattened on one side (or both) but undamaged on the nose, he could not have been hitting the branches "nose on" with the bullets. A flattened bullet, with a pristine nose, is indicative of a bullet hitting something hard at an oblique or tangential angle (almost "side on" as we would say around here. A bullet hitting at this kind of angle is guaranteed to be tumbling, and way off its mark.
P.S.
Tom
Mark a point on the ground and run two lines out from it about 75 feet. A couple of inches out from the origin, separate the lines by an inch. Go out to the 75 foot mark and see how far apart the lines are.
-
As an extension of the experiment shooting through live oak branches, it would be interesting to have a chronograph set up on the far side of the branch to measure the velocity of the bullet, once it had passed through the branch.
-
Since we're talking about the back wound...O'Connor has drawn several bullet fragments, and the sketch is labelled "bullet" fragments, does it seem peculiar that a FMJ bullet has 'fragmented' after penetrating only soft tissue?

Tom
Hi Tom
Interesting drawing by Paul O'Connor, and one I have not seen before. No, a FMJ bullet would not do that. Neither would a soft tipped or hollow point bullet. In fact, at that low of a velocity, a frangible bullet would not even do anything like that.
The obvious question comes to my mind; how did O'Connor know those bullet fragments were down at the bottom of that wound? Did Humes tell him, or was he allowed to put his finger into the wound, too?
I almost hate to say this, as it will give support to Purvis' tumbling-bullet-entering-the-back-base-first theory, but there actually is a way a FMJ bullet could deposit fragments like this.
A full metal jacket does not really cover the lead core of a bullet completely. The base of a FMJ bullet is open, exposing the lead core, and on the base of a 6.5 mm FMJ bullet, the opening is approximately 4.5 mm in diameter. This opening allows the FMJ bullet to retain its "humane" characteristics in a wound. I'll try to explain.

Construction of FMJ bullet showing open base.
External forces acting on a bullet (ie. striking bone) tend to deform bullets and often result in the space inside the bullet jacket being reduced. As lead, like water, cannot be compressed, a fully jacketed lead core would, under compression, cause internal pressures inside the jacket to rise, to the point the jacket would rupture and the bullet likely fragment into many pieces. This, of course, would lead to horrible large wounds; exactly the opposite of what a FMJ bullet is intended to do. The open base of the FMJ bullet acts as a sort of safety vent, or pressure relief valve. As the bullet jacket is compressed in a wound, lead is extruded out the base of the bullet; similar to toothpaste extruding from a tube.
To give Purvis (and O'Connor) the benefit of the doubt, yes, the bullet could have hit the branch, deformed and had lead hanging out its base as it tumbled toward JFK. IF it struck JFK base first (and that is a BIG if) it is remotely possible these lead flakes could have broken away from the base of the bullet, and stayed in the wound after the bullet had fallen out.
However, I would pay good money to see someone re-create this, as I do not believe it to be possible.
-
Frangible bullets would have been used for two reasons. 1. As they are designed to disintegrate to powder after travelling through semi-liquid matter and flesh a couple of inches, they transfer all of their energy to surrounding tissue and have the potential to be more lethal than any other bullet, except perhaps an exploding bullet. 2. Frangible bullets not only disintegrate to powder inside of a wound, they also disintegrate if they hit something hard like steel or concrete.This would tend to keep collateral damage to a minimum. 3. The general characteristics of a frangible bullet jacket are very similar to a full metal jacket bullet jacket, to the point where someone finding a piece of bullet jacket on Elm St. would be unable to identify it as a frangible bullet jacket, unless he knew what to look for.
I think your frangible bullet scenario makes a lot of sense, particularly given that Kennedy had a punctured lung seeming to have come from the back wound, yet no noticeable puncture through the pleura.
I think a tiny fragment must have punctured the pleura. (Please let me know if there's a problem with this statement.)
If it can be shown or reasoned that the velocity of a standard bullet would have been much less than the 380 fps in my analysis -- say below 250 fps -- then I would definitely favor your theory over the one I adopted from Purvis. Your comment on the speed of Ruby's bullet sank in after all.
Well, the problem is that I doubt any bullet, even a frangible bullet, would break apart after only penetrating an inch in flesh and then stopping. Frangible bullets require much more velocity and travelling through a few inches of flesh, lung or brain matter to make them break up. Of course, I have no idea how a frangible bullet would have been constructed in 1963, and I won't discount the possibility of a particle of that bullet escaping.
-
o
o
o
Autopsy witnesses said that Humes probed the back wound but found that the pleura had not been penetrated. So you must be saying that there was indeed a hole in the pleura, it's just that it was a tiny one that the probe wouldn't fit through. Is that right?
o
o
o
From what we know of the autopsy proceedings, the only probe used by Humes in examining JFK's back wound was his little finger.
o
o
o
Humes mentions the probe(s) in his WC testimony (see below).
According to ARRB's Douglass Horne:
[Autopsy technician] Jim Jenkins recalled a very shallow back wound in JFK's upper posterior thorax, that did not transit the body. He recalled Dr. Humes sticking his finger in the wound, and seeing Dr. Humes' finger making an indentation in the intact pleura as he viewed Humes' probing from the other side, where the right lung would have been before its removal. The pleura was intact. Jenkins also recalled seeing a bruise at the top of the middle lobe of the right lung (but not at the top, or apex of the right lung). Jenkins also recalled that the back wound was 10 centimeters lower than the tracheotomy site in the anterior neck.
HUMES WC TESTIMONY
Commander HUMES - I--our previously submitted report, which is Commission No. 387, identified a wound in the low posterior neck of the President.
The size of this wound was 4 by 7 mm., with the long axis being in accordance with the long axis of the body, 44 mm. wide, in other words, 7 mm. long.
We attempted to locate such wounds in soft tissue by making reference to bony structures which do not move and are, therefore, good reference points for this type of investigation.
We then ascertained, we chose the two bony points of reference we chose to locate this wound, where the mastoid process, which is just behind the ear, the top of the mastoid process, and the acromion which is the tip of the shoulder joint. We ascertained physical measurement at the time of autopsy that this wound was 14 cm. from the tip of the mastoid process and 14 cm. from the acromion was its central point--
Mr. SPECTER - That is the right acromion?
Commander HUMES - The tip of the right acromion, yes, sir, and that is why we have depicted it in figure 385 in this location.
This wound appeared physically quite similar to the wound which we have described before in 388 "A," with the exception that its long axis was shorter than the long axis of the wound described above. When the tissues beneath this wound were inspected, there was a defect corresponding with the skin defect in the fascia overlying the musculature of the low neck and upper back.
I mentioned previously that X-rays were made of the entire body of the late President. Of course, and here I must say that as I describe something to you, I might have done it before or after in the description but for the sake of understanding, we examined carefully the bony structures in this vicinity well as the X-rays, to see if there was any evidence of fracture or of deposition of metallic fragments in the depths of this wound, and we saw no such evidence, that is no fracture of the bones of the shoulder girdle, or of the vertical column, and no metallic fragments were detectable by X-ray examination.
Attempts to probe in the vicinity of this wound were unsuccessful without fear of making a false passage.
Mr. SPECTER - What do you mean by that, Doctor?
Commander HUMES - Well, the defect in the fascia was quite similar, which is the first firm tissue over the muscle beneath the skin, was quite similar to this. We were unable, however, to take probes and have them satisfactorily fall through any definite path at this point. [Emphases added.]
Welcome to the insanity that was the autopsy conducted on JFK's corpse at Bethesda, Maryland.
Do you see a problem with Jenkins' description of probing the wound and Humes' description of the same process?
According to Jenkins, he saw, from the inside of JFK's empty chest cavity, Humes' finger making an indentation in the parietal pleura membrane. This is the membrane lining the inside of the chest cavity that is visible once the lungs are removed.
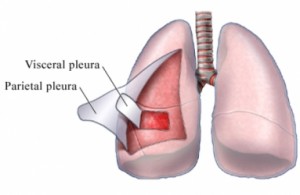
Why is Humes discussing the use of probes and his concern they might make a false track in the back wound? The wound, at least according to this story, obviously went as far as the thin membrane known as the parietal pleura. If Jenkins had looked closely enough, he might have been able to see Humes' fingertip through the membrane. Would he not have mentioned this to Humes? What was there left to probe, anyways? The first slight push of a metal probe and it would have been inside the chest cavity.
"Jenkins also recalled seeing a bruise at the top of the middle lobe of the right lung (but not at the top, or apex of the right lung)."
Here we go down the rabbit hole. Look closely at the diagrams below for a few seconds:


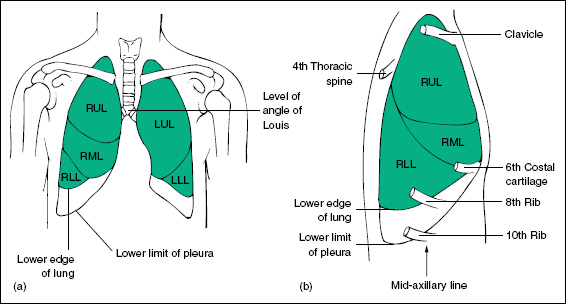

Hopefully, I have not overwhelmed you with all of these diagrams. The purpose of showing them is to highlight the very strange observation made by Jenkins; that being the bruising he observed at the top of the middle lobe of JFK's right lung. As can be seen in the 2nd to last diagram, the top of the middle lobe ends well below the 4th thoracic vetebra, or T4. The diagram above this one shows thoracic vertebra T3 to be on a level with the top of the right lung, and this is where many witnesses at Bethesda reported seeing the entrance wound in the back.
So, if the top of the middle lobe of the right lung is way down near thoracic vertebra T5, how could Jenkins see bruising of the top of the middle lobe if, according to the WC, the bullet entered JFK's back at the level of vertebrae C7/T1? An entrance wound at T3 would still be too high to account for this bruising.
There is a possible explanation for this. The visceral pleura, the membrane inside the parietal pleura, is a continuous membrane that completely envelops the lungs. It is also continuous with the membranes that separate the lobes of the lungs. This part is known as the "fissures" of the lungs, and they effectively separate the lobes of the lung into separate, isolated units. If bleeding were to occur in the top lobe of JFK's right lung it could, by gravity, collect at the lower part of this lobe, where it would be prevented from going into the middle lobe by the membrane. Is it possible Jenkins mistook pooling blood in the bottom of the top lobe for bruising in the top of the middle lobe?
Many WC supporters would jump on this and tell us yes, this is possible, but the blood was from the bullet passing ABOVE the right lung, on its way to the throat wound. The theory is that the shock wave surrounding the bullet, as it passed through the neck, would rupture blood vessels in the top of the lung, and this would account for the blood. Close, but not quite. I have seen many deer shot through the base of the neck with high powered rifles, although it is not really fair to compare this to the assassination, as these shots were all made with soft tipped bullets. Yes, the shock can actually rupture blood vessels in the top of the lungs, as well as blood vessels going to the front legs. The big difference is that when the lungs are removed, the bruising to the tops of the lungs is quite obvious, unlike what Jenkins described to Horne.
The thing to remember about the autopsy is that there were many lies told about it, and that, as the saying goes, within every lie is an element of the truth. For example, between Humes and Jenkins, only one of these two can be telling the truth about probing the back wound. Yet, if we use our imaginations, could it not be possible both of these men are telling a lie, with just enough truth mixed in to make the story work?
-
Robert,
Wow, Kennedy had a collapsed lung! I did not know that. I can't believe others haven't made a bigger deal of this information. It makes a big difference in how I think about the wounds.
Autopsy witnesses said that Humes probed the back wound but found that the pleura had not been penetrated. So you must be saying that there was indeed a hole in the pleura, it's just that it was a tiny one that the probe wouldn't fit through. Is that right?
BTW I found a good thread for me to review your and Cliff's beliefs on the back wound:
For Cliff Varnell: Where did the Bullet in JFK's Back go?
http://educationforum.ipbhost.com/index.php?showtopic=21592
I skimmed over some of it and one thing you said surprised me. You said that you thought the throat wound was an exit for one of the particles from the base-of-the-skull frangible bullet. (If I understood you correctly.) What mabe you decide the particle came from that bullet? Why not from the back-wound frangible bullet? The particle would have had to make quite a sharp turn had it come from the base-of-head bullet.
Also, why not postulate that the throat wound was a shot from the front and was a frangible bullet. Oh, I remember now... you argued that there would be more blood if that shot came from the front. Maybe. Or maybe the bullet (from a frontal shot) fragmented after passing though the esophagus, and the blood splatter was contained therein.
Do you believe all the bullets used were frangible? If so, how do you explain the bullet that reportedly was found behind the ear in Bethesda? (This bullet seems to be rarely mentioned.)
Why do you think that frangible bullets would be used to kill Kennedy?
From what we know of the autopsy proceedings, the only probe used by Humes in examining JFK's back wound was his little finger.
The bullets for the 6.5mm Carcano are actually 6.8 mm in diameter (6.5 mm being the calibre). This equates to just a shade over 1/4". (6.8 mm = .267" while 1/4" = .250", a difference of 17/1000ths of an inch) When I measured my little finger at the first knuckle, I found it to be just under 3/4" in diameter. I know that skin and muscle is somewhat elastic but, unless Humes had fingers like a four year old girl, I fail to see how an effective probing could have been done with his little finger.
The throat wound is indeed a mystery, and I believe I mentioned the source as a shrapnel particle from the head wound only as a possibility.
The throat wound could only have been an exit for the back wound if the back wound was as high up as the autopsy results attempted to portray it. If the back wound was at the level of thoracic vertebra T3, as observed by most witnesses, a fragment from the bullet would be required to make a severe change of direction upwards to exit at the throat.
Yes, I believe all of the bullets used were frangible, including the bullet that struck Tague with a fragment. I really don't know what to say about the bullet that was supposedly lodged behind JFK's ear, although it may have been a section of the copper alloy bullet jacket mistaken by onlookers for a bullet.
Frangible bullets would have been used for two reasons. 1. As they are designed to disintegrate to powder after travelling through semi-liquid matter and flesh a couple of inches, they transfer all of their energy to surrounding tissue and have the potential to be more lethal than any other bullet, except perhaps an exploding bullet. 2. Frangible bullets not only disintegrate to powder inside of a wound, they also disintegrate if they hit something hard like steel or concrete.This would tend to keep collateral damage to a minimum. 3. The general characteristics of a frangible bullet jacket are very similar to a full metal jacket bullet jacket, to the point where someone finding a piece of bullet jacket on Elm St. would be unable to identify it as a frangible bullet jacket, unless he knew what to look for.
-
Here is something else to think about. A 158 grain bullet fired from a .38 Special revolver (similar to the weapon Ruby used to kill Oswald) will leave the barrel of that revolver at a muzzle velocity of 587 feet/second (fps); a mere 193 fps faster than the theoretical bullet that supposedly only penetrated JFK's back a mere inch.
At 587 fps, according to the medical report from Parkland Memorial Hospital, this bullet travelled a left to right course through Oswald's abdomen; passing through almost every abdominal organ on its way through and coming very close to exiting the right side of Oswald's abdomen.
Considering the mass of a Carcano bullet is 162 grains, does anyone think that slowing this bullet to 380 fps would severely limit its penetrating capabilities in flesh, as opposed to the same bullet travelling at 587 fps?
-
The late Tom Purvis offered the theory that the bullet passed through a branch of the live oak tree outside the TSBD, which flattened it somewhat, slowed it down, caused some of the lead core to extrude from the base, and sent the bullet on a tumbling track. He believed that the reason the bullet wound in JFK's back was the shape it was [not round] was because the bullet was still tumbling...and that the tearing of the cloth of the jacket and the shirt in the fashion it did was due to the bullet striking the jacket base first, and acting more like a "wadcutter" bullet than the round-nosed projectile that started its flight. Purvis then claimed that this bullet was CE399, which did NOT strike Connally.
Many have disagreed with Purvis' theory, but Purvis also noted that at the time of the WC re-enactments in Dealy plaza, some branches from that live oak tree were trimmed...begging the question, for what purpose?
Mr. Purvis is no longer around to answer any questions about this, but there are several of us here to whom he sent copies of his work on the topic. Perhaps one of the other recipients of the Purvis materials could explain this in greater detail.
Thanks guys for your replies. I'm happy to see that there are indeed some plausible explanations for the back wound.
I'll get to the other ideas in turn. Right now I'll focus on Tom Purvis's theory.
The key to this problem's solution (assuming a traditional lead bullet was used) is that the bullet became slowed down, not as far away as the TSBD, but close enough to Kennedy that it would have dropped only a few inches before hitting him. (Because slow bullets drop so far as to render them too inaccurate at long ranges.) With that in mind I will test Purvis's theory.
I believe that the WC concluded that the nearest distance a shot was possible was at about 170 ft from the TSBD. From a diagram in this link
http://img835.imageshack.us/img835/3966/dppluschartsupdated1111.gif
I've determined that the tree was located about half way between the TBSD and Kennedy at that point. So the bullet traveled about 85 ft at the slow velocity.
I've read that back wound looked consistent with a bullet traveling perhaps 300 fps. So I'll use that figure.
We can determine the approximate drop based upon these two figures. (Approximate because I will be ignoring wind resistance and the fact that the gun was shot at a downward angle, among other things.)
FORMULA
The distance an object drops due to gravity is given by the formula
d = (g * t^2)/2
where * denotes multiplication, / denotes division, and ^ denotes “to the power of” (so t^2 is t squared).
g = 32 is a constant. It is the downward acceleration of an object due to gravitational pull. Its units are ft/s^2 (feet per second squared).
t is the time the object is allowed to drop. We don’t know offhand what t is, but we can calculate it from the distance the bullet traveled toward the target. It is calculated from the equation
t = D / v
where D is the distance the bullet travels toward its target and v is its velocity. Substituting this equation into the formula above ,we get
d = (g * (D/v)^2)/2
CALCULATION
The distance D is 85 ft and the velocity is 300 fps. Plugging those into the formula we get
d = (32 * (85/300)^2)/2
d = 1.28 ft
So a 300 fps bullet would drop 15.4 inches, which is 15.1 inches lower than a where a 2000 fps bullet would hit. (I used the same formula to determine that a high speed bullet (2000 fps) would drop about 0.3".)
CONCLUSION
For my conclusion I will use a bullet velocity of 380 fps instead of the 300 fps I used above. The reason for doing so will be apparent.
If the shooter were aiming for the head and hitting a limb slowed the bullet down to 380 fps, it would hit the back about where it hit Kennedy. I can't take into account bullet deflection or tumbling, but the calculation here shows that we’re in the right ballpark. Purvis may be on to something.
(BTW, I don't believe a Carcano shot that bullet. I don't believe Oswald shot any bullet. But I do believe the shot may have come from the TSBD.)
In order to believe your theory would work requires ignoring everything I know about bullets in flight. It also requires believing that slowing a bullet from 2000 fps to 300-380 fps, by having it travel through a tree branch, will not de-stabilize the bullet to the point it will begin tumbling.
Sorry, I happen to know better.
P.S.
Your mathematics are impressive but, it is just as easy to use an on line ballistics calculator to calculate bullet drop.
-
The late Tom Purvis' scenario on the events of November 22, 1963 were indeed "complex" and I nor others who knew Tom need not defend that which Tom wrote; if you are truly interested his writings they are available. I had the pleasure of exchanging correspondence with Tom on a number of issues for over twenty years and can agree with comments written in this thread by both Mark and Don - in particular Tom's unwavering conviction that the assassination and its drawn out aftermath were indeed the "results" of a conspiracy. However, regardless of the semantics of feigning reverence for the dead, I do find it rather interesting that the individual who appears to be the self-appointed ballistics and firearms expert of the Education Forum, an individual who as far as I know does not own a Mannlicher Carcano weapon nor possess any of the alleged ammunition said by officialdom to have been involved in Dealey Plaza, would find Tom's theoretical nuances of a tumbling bullet scenario, a scenario I might add that Tom actually tested, as entering the realm of "astronomical". Would it be fair to ask more "astronomical" than a "frangible" bullet of unknown caliber, fired by an unknown assassinfrom an unknown weapon from an unknown location at an unknown specific point in time along Elm Street - presumably from behind?
I don't believe for one second that Purvis actually tested his tumbling bullet theory, just as I don't believe a lot of the other nonsense he wrote about firearms and Carcanos. You can slag me all you want, Mr. Murr but, don't think I have any illusions about where your defense of Tom Purvis is coming from. BTW, you never did answer my question about the diameter of Carcano bullets, and the diameter SA Robert A. Frazier obtained when he measured pristine WCC Carcano bullets.
Having handloaded my own rifle cartridges for many years, I can speak with experience about tumbling bullets, as this effect occurs when one is experimenting with different loads of gunpowder and different bullets. The wrong load can either under- or over-stabilize a bullet in flight and cause it to begin tumbling. When looking at a paper target, we refer to this as "keyholing", as the bullet, instead of making a neat little round hole in a paper target, will make an oblong hole resembling a keyhole as it goes through the paper sideways. Know how many times I saw a tumbling bullet make a round hole in a paper target instead of a "keyhole"? ZERO.
As I said earlier, EVEN IF the bullet did magically manage to hit JFK's back at the exact moment the base of the bullet was pointing in the line of travel, this was still a tumbling bullet, and as it entered the flesh of JFK's back, it would have continued to tumble. It would make a wound that bore no resemblance at all to the wound seen on JFK's back.
As I said, defend Tom Purvis all you want. I see this as a continuation of the effort to place a shooter on the SE corner of the 6th floor of the TSBD.
-
I've seen a couple of estimates on what the speed of the bullet hitting Kennedy's back must have been to make such a shallow wound. Using those figures I calculated how far the bullet would have dropped had it been fired from the TSBD at such low speeds and was surprised at the result. The bullet would have dropped over 20 feet! In other words, a sniper would have had to aim 20 feet high in order to hit the president.
Not believing that figure, I did the same calculation for a high-speed bullet, and found it would have dropped around 3 inches. Now that seemed reasonable, and it gave me confidence that my calculation for the low speed bullet was correct. (The reason for the huge difference between a high-speed and low-speed bullet is that the calculation has a square in it. So a bullet that is a that is, say, a fourth the speed will drop sixteen times as far.)
Since then I've been trying to figure out how to explain the back wound. I can't.
Are there any prevailing theories on how the back wound came to be?
After having read several of the posts on this relevant thread:
http://educationforum.ipbhost.com/index.php?showtopic=22173&hl=%20back%20%20wound&page=1
I'm left with the feeling there are no prevailing theories. Which is odd, if true, given that researchers have had fifty years to think about it.
Hi Sandy
I see you have linked to a thread I began some time ago. I will assume you are familiar now with my low opinion of the "short shot" and the "shallow" back wound.
If you read more of my threads, you will see that I personally believe the type of bullet that entered JFK's back, as well as the bullet(s) that entered his skull, were a type of bullet known as a "frangible" bullet; a bullet made from compressed, sintered or glued lead (or other metals) powder. The lethal version of a frangible bullet also has a hollow point nose to exert maximum fluid pressure on the interior of this bullet, after it penetrates a few inches, to cause it to disintegrate back into a cloud of metal powder capable of inflicting lethal internal injuries.
From the medical report of Dr. Marion T. Jenkins, surgeon, Parkland Memorial Hospital, Nov. 22, 1963, 1630 hours:
"Upon receiving a stat alarm that this distinguished patient was being brought to the emergency room at Parkland Memorial Hospital, I dispatched Doctors A . H. Giesecke and Jackie H. Hunt with an anesthesia machine and resuscitative equipment to the major surgical emergency room area, and I ran down the stairs . On my arrival in the emergency operating room at approximately 1230 I found that Doctors Carrico and/or Delaney had begun resuscitative efforts by introducing an orotracheal tube, connecting it for controlled ventilation to a Bennett intermittent positive pressure breathing apparatus . Doctors Charles Baxter, Malcolm Perry, and Robert McClelland arrived at the same time and began a tracheostomy and started the insertion of a right chest tube, since there was also obvious tracheal and chest damage . Doctors Paul Peters and Kemp Clark arrived simultaneously and immediately thereafter assisted respectively with the insertion of the right chest tube and with manual closed chest cardiac compression to assure circulation."
From the Warren Commission testimony of Dr. Marion T. Jenkins, March 25, 1964, 1730 hours:
"Dr. JENKINS - Well, I was aware of what he was in an agonal state. This is not a too unfamiliar state that we see in the Service, as much trauma as we see, that is, he had the agonal respiratory gasp made up of jerking movements of the mylohyoid group of muscles. These are referred to sometimes as chin jerk, tracheal tug or agonal muscles of respiration. He had this characteristic of respiration. His eyes were opened and somewhat exophthalmic and color was greatly suffused, cyanotic---a purplish cyanosis.
Still, we have patients in the state, as far as cyanosis and agonal type respiration, who are resuscitatable. Of course, you don't step at this time and think, "Well, this is a hopeless circumstance,"--because one in this state can often be resusciated--this represents the activities prior to one's demise sometimes, and if it can be stepped, such as the patient is oxygenated again and circulation reinstituted, he can be saved.
Dr. Carrico had just introduced an endotracheal tube, I'm very proud of him for this because it's not as easy as it sounds. At times and under the circumstances--it was harder--he had. just completed a 3-month rotation on the anesthesiology service, and I thought this represented good background training for a smart individual, and he told me he had a cuff on the endotracheal tube and he introduced it below the wound.
The reason I said this, of course, this is a reflex--there is a tube, the endotracheal tube, if it is pushed down a little too far it can go into the right main stem of the bronchus impairing respiration from both lungs, or both chest.
There was in the room an intermittent positive pressure breathing apparatus, which can be used to respire for a patient. As I connected this up, however, Dr. Carrico and I connected it up to give oxygen by artificial respiration, Dr. Giesecke and Dr. Hunt arrived on the scene with the anesthesia machine and I connected it up instead with something I am more familiar with--not for anesthesia, I must insist on that--it was for the oxygenation, the ability to control ventilation with 100 percent oxygen.
As I came in there, other people came in also. This is my recollection. Now, by this time I was in familiar surroundings, despite the anguish of the circumstance.
Despite the unusual circumstance, in terms of the distinguished personage who was the patient, I think the people who had gathered or who had congregated were so accustomed to doing resuscitative procedures of this nature that they knew where to fit into the resuscitation team without having a preconceived or predirected plan, because, as obviously--some people were doing things not necessarily in their specialty, but there was the opening and there was the necessity for this being done.
There were three others who came in as I did who recognized at once the neck wound, in fact, where the wound was, would indicate that we would have serious pulmonary problems unless a tracheotomy tube was put in. This is one way of avoiding pushing air out through a fractured trachea and down into each chest cavity, which would cause a pneumothorax or a collapse of the lungs. These were doctors Malcolm Perry, Charley Baxter, and Robert McClelland, who with Dr. Carrico's help, I believe, started the tracheotomy.
About this time Drs. Kemp Clark and Paul Peters came in, and Dr. Peters because of the appearance of the right chest, the obvious physical characteristics of a pneumothorax, put in a closed chest drainage chest tube. Because I felt no peripheral pulse and was not aware of any pulse, I reported this to Dr. Clark and he started closed chest cardiac massage.
There were other people--one which started an I.V. in a cutdown in the right leg and one a cutdown in the left arm. Two of my department connected up the cardioscope, in which we had electrical silence on the cardioscope as Dr. Clark started closed chest massage. That's the sequence of events as I reconstructed them that day and dictated them on my report, which you have here, I think."
Note that Jenkins, in his medical report, speaks only of the insertion of a right chest tube (and not a left chest tube) to deal with "obvious tracheal and chest damage", not suspected tracheal and chest damage. He expands on this in his WC testimony, as seen in the 2nd last paragraph I quoted from his testimony above, where he describes Dr. Paul Peters inserting a "closed chest drainage chest tube" because of "the appearance of the right chest, the obvious physical characteristics of a pneumothorax".
What Jenkins is telling the WC, is that something had entered JFK's right chest cavity and damaged his right lung, to the point the lung was no longer airtight and had, effectively, collapsed. Whenever a breath was drawn in by JFK (agonal breathing by JFK was witnessed in Trauma Room One and I believe this proves that JFK did not die instantly at the scene of the assassination and there was breathing, albeit it limited, all the way to Parkland), the indrawn breath would pass through the hole in JFK's right lung and fill the pleural cavity between lung and chest wall. When he exhaled, the hole in the lung would seal, trapping the air in the pleural cavity. With each breath, the volume of air would grow, until this air volume began exerting pressure on the left lung and heart; impairing their function to the point death could occur.
The medical procedure to alleviate this condition is, as described by Dr. Jenkins, the insertion into the pleural cavity of a large bore needle or tube, through the intercostal space between the 2nd and 3rd rib at the midclavicular line, and connecting that tube to closed chest drainage. This closed chest drainage allows air to escape from the chest on exhalation but prevents air returning to the chest cavity on inhalation.
A frangible bullet entering JFK's back, 1.5-2 inches to the right of the spinal midline and at the level of thoracic vertebra T3, would go directly into the top of JFK's right lung. A well made hollow point frangible bullet would disintegrate to powder part way through the lung, and not exit.
It was vital to conceal the damage done by this bullet to the right lung, as knowledge of its disintegrating quality would ultimately lead people to inquire about the explosive characteristics of the bullet that struck JFK in the head.
-
The late Tom Purvis offered the theory that the bullet passed through a branch of the live oak tree outside the TSBD, which flattened it somewhat, slowed it down, caused some of the lead core to extrude from the base, and sent the bullet on a tumbling track. He believed that the reason the bullet wound in JFK's back was the shape it was [not round] was because the bullet was still tumbling...and that the tearing of the cloth of the jacket and the shirt in the fashion it did was due to the bullet striking the jacket base first, and acting more like a "wadcutter" bullet than the round-nosed projectile that started its flight. Purvis then claimed that this bullet was CE399, which did NOT strike Connally.
Many have disagreed with Purvis' theory, but Purvis also noted that at the time of the WC re-enactments in Dealy plaza, some branches from that live oak tree were trimmed...begging the question, for what purpose?
Mr. Purvis is no longer around to answer any questions about this, but there are several of us here to whom he sent copies of his work on the topic. Perhaps one of the other recipients of the Purvis materials could explain this in greater detail.
Hi Mark
The odds of a tumbling bullet just happening to strike JFK's back as the base of the bullet, in mid tumble, was presented forward are, at the very least, astronomical. Also, there would be nothing to stop the bullet from continuing to tumble as it entered JFK's back. Instead of a neat little hole, a tumbling bullet should leave a much larger furrowed oval wound, despite having entered base first.
I hate to speak ill of the dead but, I found serious flaws in a great deal of Mr. Purvis' writings, especially on the subjects of firearms, ballistics and, in particular, the 6.5 Carcano rifle.
-
Dr. McCLELLAND (WC Testimony) - As I took the position at the head of the table that I have already described, to help out with the tracheotomy, I was in such a position that I could very closely examine the head wound, and I noted that the right posterior portion of the skull had been extremely blasted. It had been shattered, apparently, by the force of the shot so that the parietal bone was protruded up through the scalp and seemed to be fractured almost along its right posterior half, as well as some of the occipital bone being fractured in its lateral haft, and this sprung open the bones that I mentioned in such a way that you could actually look down into the skull cavity itself and see that probably a third or so, at least, of the brain tissue, posterior cerebral tissue and some of the cerebellar tissue had been blasted out. There was a large amount of bleeding which was occurring mainly from the large venous channels in the skull which had been blasted open.
ARRB Testimony
DR. McCLELLAND: And I think as testimony that this wound looked like everybody else has described it here. It was a very large wound and I would agree that it was at least seven or eight centimeters in diameter and was mostly really in the occipital part of the skull. And as I was looking at it, a fairly large portion of the cerebellum fell out of the skull, There was already some brain there, but during the tracheostomy more fell out and that was clearly cerebellum. I mean, there was no doubt about it, and I was that far from it (indicating).
MR. GUNN: When you say "that far," you're putting your hands about twelve
inches apart.
DR. McCLELLAND: Twelve to 18 inches.
Boy, McClelland sure sounds confused, eh, Pat?
If all else fails, they're either "confused" or just good ol' "mis-remembering".

Do I really have to explain this? These are two statements picked out because they are relatively consistent. Watch every interview of McClelland you can find on youtube. Read his ARRB testimony. Watch his conference appearances. Then go back and read what you can of his position before he found religion in the 70's. The man is anything but consistent. Heck, he's changed his story about the "McClelland drawing" so many times it will make your head spin.
Prior to his viewing the Zapruder film, McClelland was not only a supporter of the Warren Commission, but someone who actively discouraged people (such as journalist Richard Dudman and author Harold Weisberg) from believing the fatal shot came from the front. Wrap your mind around that. Now, most who reach this point come up with something about him being scared to tell the truth. But, guess what? He's been asked about this. And has adamantly denied that he was ever scared to tell the truth, or that he and his colleagues were encouraged to lie about what they saw. So, no, McClelland is not a stand-in for Dr. Crenshaw. He adamantly defends the integrity of Carrico, Jenkins, Perry, Baxter, etc--who many CTs believe were cowards and liars. He also insists the tracheotomy incision in the autopsy photos is the tracheotomy incision he saw at Parkland.
He is not the droid you've been looking for. LOL
You bet, Pat. Just keep on shooting the messenger, and ignore the message.

-
Dr. McCLELLAND (WC Testimony) - As I took the position at the head of the table that I have already described, to help out with the tracheotomy, I was in such a position that I could very closely examine the head wound, and I noted that the right posterior portion of the skull had been extremely blasted. It had been shattered, apparently, by the force of the shot so that the parietal bone was protruded up through the scalp and seemed to be fractured almost along its right posterior half, as well as some of the occipital bone being fractured in its lateral haft, and this sprung open the bones that I mentioned in such a way that you could actually look down into the skull cavity itself and see that probably a third or so, at least, of the brain tissue, posterior cerebral tissue and some of the cerebellar tissue had been blasted out. There was a large amount of bleeding which was occurring mainly from the large venous channels in the skull which had been blasted open.
ARRB Testimony
DR. McCLELLAND: And I think as testimony that this wound looked like everybody else has described it here. It was a very large wound and I would agree that it was at least seven or eight centimeters in diameter and was mostly really in the occipital part of the skull. And as I was looking at it, a fairly large portion of the cerebellum fell out of the skull, There was already some brain there, but during the tracheostomy more fell out and that was clearly cerebellum. I mean, there was no doubt about it, and I was that far from it (indicating).
MR. GUNN: When you say "that far," you're putting your hands about twelve
inches apart.
DR. McCLELLAND: Twelve to 18 inches.
Boy, McClelland sure sounds confused, eh, Pat?
If all else fails, they're either "confused" or just good ol' "mis-remembering".
-
So what's with an entry wound at the left temple (McClelland). I'd like to know more about that. (It could certainly account, I assume, for a gaping exit wound in the right rear of the head, depending on where the shot came from.)
Nope. The Parkland witnesses saw one head wound. Clark, the only one to take a good look, presumed this was a wound of both entrance and exit. McClelland wrote, moreover, that the wound was "of the left temple" and not an entrance wound "to the left temple" that presumably might have exited elsewhere. It follows then that McClelland thought, if only for a short period, that the one wound observed by himself and others was by the left temple.
Of course, he was looking at him upside down, and may have got his left and right mixed up. It is most intriguing then that within weeks--perhaps even days--of the shooting, the article written from the first day reports of the Parkland doctors quoted McClelland as claiming it was a wound of the right temple, not left.
Here is what Dr. Robert McClelland actually wrote in his medical report, 4:45 PM, Nov. 22/ 1963:
"At approximately 12:45 PM on the above date I was called from the second floor of Parkland Hospital and went immediately to the Emergency Operating Room. When I arrived President Kennedy was being attended by Drs Malcolm Perry, Charles Baxter, James Carrico, and Ronald Jones. The President was at the time comatose from a massive gunshot wound of the head with a fragment wound of the trachea. An endotracheal tube and assisted respiration was started immediately by Dr. Carrico on Duty in the EOR when the President arrived. Drs. Perry, Baxter, and I then performed a tracheotomy for respiratory distress and tracheal injury and Dr. Jones and Paul Peters inserted bilateral anterior chest tubes for pneumothoracis secondary to the tracheomediastinal injury. Simultaneously Dr. Jones had started 3 cut-downs giving blood and fluids immediately, In spite of this, at 12:55 he was pronounced dead by Dr. Kemp Clark the neurosurgeon and professor of neurosurgery who arrived immediately after I did. The cause of death was due to massive head and brain injury from a gunshot wound of the left temple. He was pronounced dead after external cardiac message failed and ECG activity was gone. He was pronounced dead after external cardiac message failed and ECG activity was gone."
Note that McClelland states ".....cause of death was due to massive head and brain injury from a gunshot wound of the left temple" If the massive brain injury was from the gunshot wound, I seriously believe McClelland is telling us he believed there was a gunshot wound in JFK's left temple. However, Pat, you believe whatever you want to believe.
"There are none so blind, as those who will see only what they wish to see."
-
So what's with an entry wound at the left temple (McClelland). I'd like to know more about that. (It could certainly account, I assume, for a gaping exit wound in the right rear of the head, depending on where the shot came from.)
Nope. The Parkland witnesses saw one head wound. Clark, the only one to take a good look, presumed this was a wound of both entrance and exit. McClelland wrote, moreover, that the wound was "of the left temple" and not an entrance wound "to the left temple" that presumably might have exited elsewhere. It follows then that McClelland thought, if only for a short period, that the one wound observed by himself and others was by the left temple.
Of course, he was looking at him upside down, and may have got his left and right mixed up. It is most intriguing then that within weeks--perhaps even days--of the shooting, the article written from the first day reports of the Parkland doctors quoted McClelland as claiming it was a wound of the right temple, not left.
This is from the medical report written by Dr. Kemp Clark regarding JFK:
"Dr. Carrico noted the President to have slow, agenal respiratory efforts. He could hear a heartbeat but found no pulse or blood pressure to be present. Two external wounds, one in the lower third of the anterior neck, the other in the occipital region of the skull, were noted. Through the head wound, blood and brain were extruding. Dr. Carrico inserted a cuffed endotracheal tube. While doing so, he noted a ragged wound of the trachea immediately below the larynx."
"There was a large wound in the right occipito-parietal region, from which profuse bleeding was occurring. 1500 cc. of blood were estimated on the drapes and floor of the Emergency Operating Room. There was considerable loss of scalp and bone tissue. Both cerebral and cerebellar tissue were extruding from the wound."
Two problems here, Pat. Nowhere in his report does Dr. Clark say he presumed this large wound in the rear of JFK's head was a wound of entrance and exit. He also states that he saw cerebral AND cerebellar tissue extruding from the wound, and that the wound was in the occipito-parietal region.
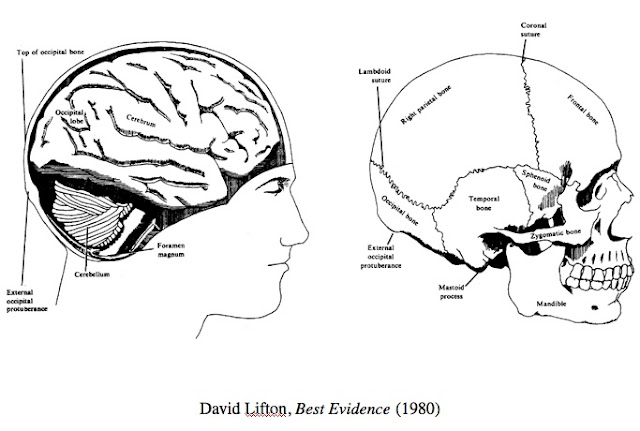
Cerebellum (source of cerebellar tissue seen by Dr. Clark) seen at lower rear of cranial cavity
-
Chris, twenty years ago certainly does feel wrong...not sure if it seems longer or shorter than that though. The individual who presented was not a practicing Doctor at the time of the assassination, only an intern - wish I could remember his name but he presented well after that summary was done, at least ten years or more. I'll ask Deb and see if she remembers him....
From patspeer.com, chapter 18d:
This brings us to Zelditz... When contacted by Vince Palamara in 1998, Dr. William Zelditz reported that he arrived in Trauma Room One just before the tracheotomy was performed and noted "a massive head injury to the right occipito-parietal area (right posterior-lateral) of the cranium." He said the wound covered an area approximately 10-12 centimeters in diameter. Well, this is too big to be the wound in the McClelland drawing, but it appears to be close enough. Zelditz spoke in public at the 2003 Lancer Conference in Dallas, however, and further detailed his observations. He said Kennedy was supine (flat on his back) when he (Zelditz) came in the room. He then said the head wound was "massive--the entire posterior and right side of the head was nothing but matted hair and clots, and pieces of bone and tissue, and it was a mess. I gently palpated the area and it felt like somebody had boiled an egg and then dropped it. And then picked it up. The bones were just in crinkly pieces." He was asked about this again and added: "There was an area, I'd say, 8 by 12 centimeters in the back of the head on the right hand side on the occipito-parietal area, that was gone. And it was filled with blood, tissue, hair, bone fragments, and brain fragments, and that's all you could see." Well, this is not the gaping hole behind the ear depicted in the McClelland drawing. Zelditz was then asked to depict the location of Kennedy's head wound on his own head. He placed his hand on the back of his head, with his fingers stretching from above his right ear on back to just below the top of his ear. He then admitted that beyond this area one "couldn't really tell the depth of it, or the extent of it." He was then asked if he had to rotate Kennedy's head to get a good look at the wound, and responded "No, no, there was enough of it there." He was then asked if he'd placed his hand under the head to palpate the skull, and said "No, it was in the back, and to the side." When then asked if he'd felt the extent of the wound, he admitted "No, I didn't see all of the wound. I couldn't see all of it because he was laying on that." (He then pointed to the back of his head)." He was then asked about the wound again. He put his hand back where the wound is in the McClelland drawing, and responded "It wasn't strictly straight back." He then moved his hand up to the top of his head with his fingers stretching above his right ear, and continued "It was top, back, and side." When then asked if the skull in this area was gone, he replied "It was in pieces." When then asked if the shattered skull in this area was still attached to the scalp, he continued "I could not tell. It was covered with blood and hair and other stuff. I could feel the bones but they felt like they were (he wiggled his fingers) loose." He expanded "The bony fragments that were there were loose. And there was a spongy mass in the center of that, most obvious without bone, so I guess part of the bone was gone, but still there were fragments of bone still there." When then asked the million dollar question if he felt the autopsy photos showing the back of the head to be intact were altered, he clarified "The back of the head was not intact, but it was covered, as again I mention, with hair, blood, tissue, y'know, it was all there so you couldn't tell whether it was intact underneath that or not."
Yikes, Zelditz had placed the wound about half-way between the location of the wound in the autopsy photos and the location of the wound in the McClelland drawing. His extended description of the wound, and insistence he could see it without rotating Kennedy's head, moreover, supported that the wound was as depicted in the autopsy photos, and not as depicted in the McClelland drawing.
Wouldn't the wound described by Zelditz be visible in the Back of Head autopsy photo? In Zelditz's own words, "massive--the entire posterior and right side of the head was nothing but matted hair and clots, and pieces of bone and tissue, and it was a mess."
How could such a wound be cleaned up to appear to be in a pristine state in the BOH photo?
When pushed, he explained it at the end. He said "The back of the head was not intact, but it was covered, as again I mention, with hair, blood, tissue, y'know, it was all there so you couldn't tell whether it was intact underneath that or not."
He had thereby supported the statements of the autopsy doctors, and James Jenkins, etc, and the authenticity of the x-rays. The scalp at the back of the head was intact but the bone was shattered beneath the scalp.
Once again, did they wash all of this mess away before they took the BOH photo? That hardly seems likely, Pat.
-
DVP makes a valiant attempt to have us all chasing our tails over who ordered the body be taken to Bethesda. Meanwhile, the topic of this thread is still the large gaping wound seen by many witnesses in the right rear of JFK's head, and if you can't stay on topic, DVP, I kindly invite you to go start another thread.
-
I don't think Bethesda was pre-planned. My guess is the plotters planned to hide the evidence of frontal shots in Parkland neurology, but the EOP bullet damaged the brainstem enough to stop JFK's breathing. Walter Reed was clearly the second choice. By the time they got to Bethesda, they were scrambling and if you read the witness reports to the Bethesda autopsy, it was mostly an exercise in finding the bullets. I suppose someone gave the autopsy doctors the speech about national security, and maybe they did some preautopsy explorations to take the bullet out of the neck and open the head wound. But the evidence they left behind argues strongly for two shots to the head; so that indicates they reported much of the autopsy as they saw it and then went with the national security required two shots from the back conclusions.
Regarding the difference in head wound appearance between Parkland and Bethesda, how about between the Z film and Bethesda? Frame Z335 shows a big skull flap hanging down in front of JFK's right ear; exactly as the back of head photos do.
When people talk about Clint Hill's testimony about looking down into a hole in JFK's head, they should realize that JFK was lying on his left side in Jackie's lap, so he would be looking down into the right side of JFK's head.
Sorry, Ollie but, your last statement requires Clint Hill, along with a number of trained surgeons, to be unable to distinguish between the right rear of JFK's headf and the right side of his head ahead of his right ear.
If there was a large gaping wound between JFK's right ear and his face, would it not have been obvious to the surgeons at Parkland? Wouldn't one of them have mentioned it in his medical report?
Why did they all refer to the large gaping wound as involving JFK's occipital bone?
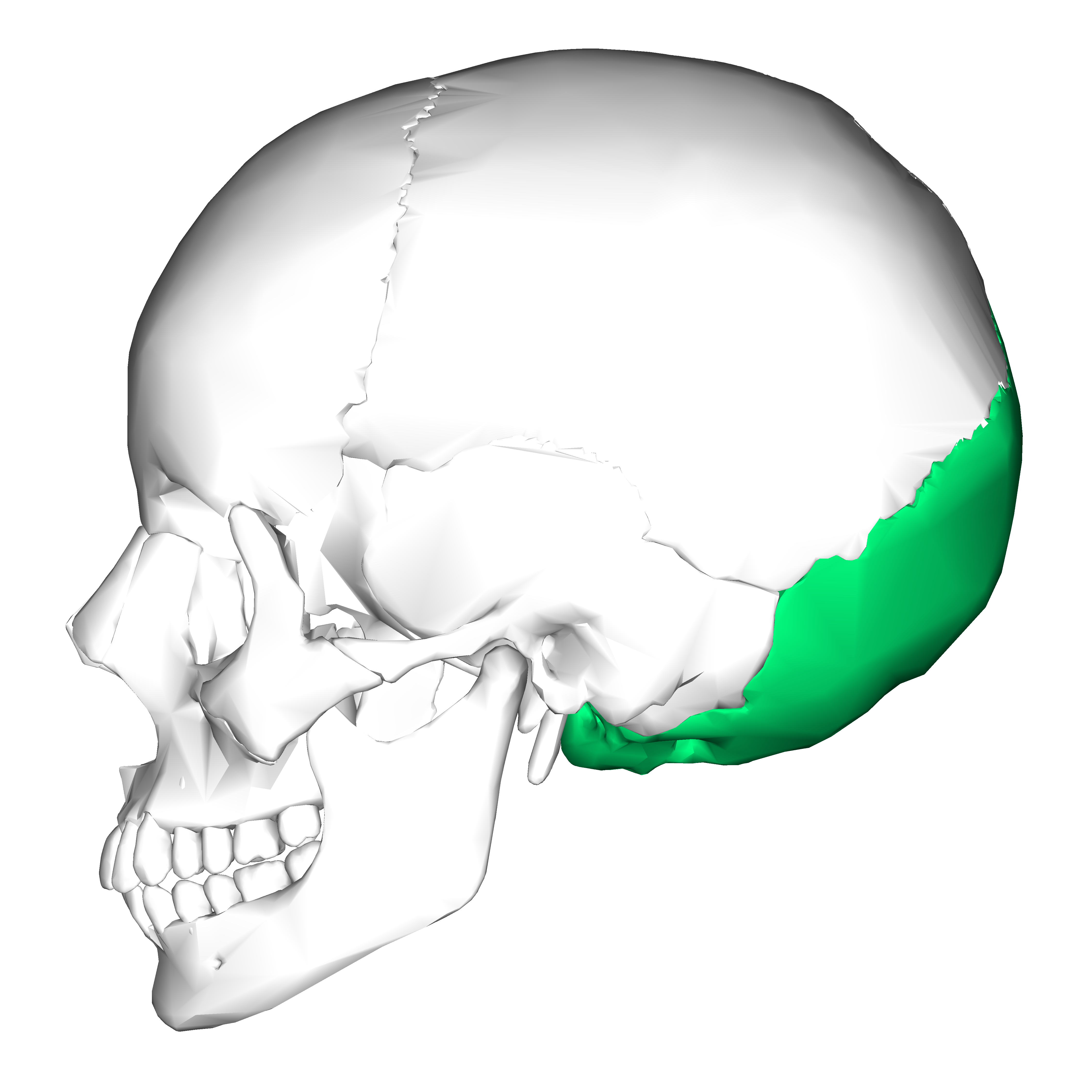

Occipital bone shown in green.
They didn't. Perry and McClelland made no mention of the occipital bone. A better question, IMO, is why didn't McClelland say the wound was on the back of the head, if it were so obviously on the back of the head.
PARKLAND MEMORIAL HOSPITAL
ADMISSION NOTE
DATE AND HOUR Nov. 22, 1963 4:45 P.M. DOCTOR: Robert N. McClelland
Statement Regarding Assassination of President Kennedy
At approximately 12:45 PM on the above date I was called from the second floor of Parkland Hospital and went immediately to the Emergency Operating Room. When I arrived President Kennedy was being attended by Drs Malcolm Perry, Charles Baxter, James Carrico, and Ronald Jones. The President was at the time comatose from a massive gunshot wound of the head with a fragment wound of the trachea. An endotracheal tube and assisted respiration was started immediately by Dr. Carrico on Duty in the EOR when the President arrived. Drs. Perry, Baxter, and I then performed a tracheotomy for respiratory distress and tracheal injury and Dr. Jones and Paul Peters inserted bilateral anterior chest tubes for pneumothoracis secondary to the tracheomediastinal injury. Simultaneously Dr. Jones had started 3 cut-downs giving blood and fluids immediately, In spite of this, at 12:55 he was pronounced dead by Dr. Kemp Clark the neurosurgeon and professor of neurosurgery who arrived immediately after I did. The cause of death was due to massive head and brain injury from a gunshot wound of the left temple. He was pronounced dead after external cardiac message failed and ECG activity was gone.
Robert N. McClelland M.D.
Asst. Prof. of Surgery
Southwestern Med.
School of Univ of Tex.
Dallas, Texas
I would think that "a gunshot wound of the left temple" would indicate McClelland believed the bullet entered JFK's left temple, but you believe whatever you like, Pat.
-

Note that Zelditz describes the wound as being "occipito-parietal". "When contacted by Vince Palamara in 1998, Dr. William Zelditz reported that he arrived in Trauma Room One just before the tracheotomy was performed and noted "a massive head injury to the right occipito-parietal area (right posterior-lateral) of the cranium." "
As the only place on the skull where the parietal and occipital bones meet anywhere close to being on the side of the skull is quite a distance behind the ear, a massive wound in the right occipito-parietal area should have been visible on the Back of Head autopsy photo.
Looking at the above diagram, it is clear that the temporal bone occupies a large portion of the side of the skull and, as the occipital bone occupies chiefly the rear of the skull, a large gaping wound in the occipito-parietal region would have to be somewhat low in the rear of the skull, and should be plainly visible in the Back of Head autopsy photo.
-
Chris, twenty years ago certainly does feel wrong...not sure if it seems longer or shorter than that though. The individual who presented was not a practicing Doctor at the time of the assassination, only an intern - wish I could remember his name but he presented well after that summary was done, at least ten years or more. I'll ask Deb and see if she remembers him....
From patspeer.com, chapter 18d:
This brings us to Zelditz... When contacted by Vince Palamara in 1998, Dr. William Zelditz reported that he arrived in Trauma Room One just before the tracheotomy was performed and noted "a massive head injury to the right occipito-parietal area (right posterior-lateral) of the cranium." He said the wound covered an area approximately 10-12 centimeters in diameter. Well, this is too big to be the wound in the McClelland drawing, but it appears to be close enough. Zelditz spoke in public at the 2003 Lancer Conference in Dallas, however, and further detailed his observations. He said Kennedy was supine (flat on his back) when he (Zelditz) came in the room. He then said the head wound was "massive--the entire posterior and right side of the head was nothing but matted hair and clots, and pieces of bone and tissue, and it was a mess. I gently palpated the area and it felt like somebody had boiled an egg and then dropped it. And then picked it up. The bones were just in crinkly pieces." He was asked about this again and added: "There was an area, I'd say, 8 by 12 centimeters in the back of the head on the right hand side on the occipito-parietal area, that was gone. And it was filled with blood, tissue, hair, bone fragments, and brain fragments, and that's all you could see." Well, this is not the gaping hole behind the ear depicted in the McClelland drawing. Zelditz was then asked to depict the location of Kennedy's head wound on his own head. He placed his hand on the back of his head, with his fingers stretching from above his right ear on back to just below the top of his ear. He then admitted that beyond this area one "couldn't really tell the depth of it, or the extent of it." He was then asked if he had to rotate Kennedy's head to get a good look at the wound, and responded "No, no, there was enough of it there." He was then asked if he'd placed his hand under the head to palpate the skull, and said "No, it was in the back, and to the side." When then asked if he'd felt the extent of the wound, he admitted "No, I didn't see all of the wound. I couldn't see all of it because he was laying on that." (He then pointed to the back of his head)." He was then asked about the wound again. He put his hand back where the wound is in the McClelland drawing, and responded "It wasn't strictly straight back." He then moved his hand up to the top of his head with his fingers stretching above his right ear, and continued "It was top, back, and side." When then asked if the skull in this area was gone, he replied "It was in pieces." When then asked if the shattered skull in this area was still attached to the scalp, he continued "I could not tell. It was covered with blood and hair and other stuff. I could feel the bones but they felt like they were (he wiggled his fingers) loose." He expanded "The bony fragments that were there were loose. And there was a spongy mass in the center of that, most obvious without bone, so I guess part of the bone was gone, but still there were fragments of bone still there." When then asked the million dollar question if he felt the autopsy photos showing the back of the head to be intact were altered, he clarified "The back of the head was not intact, but it was covered, as again I mention, with hair, blood, tissue, y'know, it was all there so you couldn't tell whether it was intact underneath that or not."
Yikes, Zelditz had placed the wound about half-way between the location of the wound in the autopsy photos and the location of the wound in the McClelland drawing. His extended description of the wound, and insistence he could see it without rotating Kennedy's head, moreover, supported that the wound was as depicted in the autopsy photos, and not as depicted in the McClelland drawing.
Wouldn't the wound described by Zelditz be visible in the Back of Head autopsy photo? In Zelditz's own words, "massive--the entire posterior and right side of the head was nothing but matted hair and clots, and pieces of bone and tissue, and it was a mess."
How could such a wound be cleaned up to appear to be in a pristine state in the BOH photo?
-
I don't think Bethesda was pre-planned. My guess is the plotters planned to hide the evidence of frontal shots in Parkland neurology, but the EOP bullet damaged the brainstem enough to stop JFK's breathing. Walter Reed was clearly the second choice. By the time they got to Bethesda, they were scrambling and if you read the witness reports to the Bethesda autopsy, it was mostly an exercise in finding the bullets. I suppose someone gave the autopsy doctors the speech about national security, and maybe they did some preautopsy explorations to take the bullet out of the neck and open the head wound. But the evidence they left behind argues strongly for two shots to the head; so that indicates they reported much of the autopsy as they saw it and then went with the national security required two shots from the back conclusions.
Regarding the difference in head wound appearance between Parkland and Bethesda, how about between the Z film and Bethesda? Frame Z335 shows a big skull flap hanging down in front of JFK's right ear; exactly as the back of head photos do.
When people talk about Clint Hill's testimony about looking down into a hole in JFK's head, they should realize that JFK was lying on his left side in Jackie's lap, so he would be looking down into the right side of JFK's head.
Sorry, Ollie but, your last statement requires Clint Hill, along with a number of trained surgeons, to be unable to distinguish between the right rear of JFK's headf and the right side of his head ahead of his right ear.
If there was a large gaping wound between JFK's right ear and his face, would it not have been obvious to the surgeons at Parkland? Wouldn't one of them have mentioned it in his medical report?
Why did they all refer to the large gaping wound as involving JFK's occipital bone?
Occipital bone shown in green.
-
Pretty clearly to me, the autopsy was pre-planned. Not by Humes, et al. But by guys like McGeorge Bundy.
And when such a fantastic (and absurd) notion gets embedded in a person's mind, it becomes all but impossible for an innocent party to exonerate himself. Such as when Dr. Humes made the following statement in 1991. Is any CTer who has decided (without a speck of proof, of course) that JFK's autopsy was "pre-planned" going to believe a single word uttered by Dr. Humes now? Of course not. Just like gum on your shoe, a false allegation, if repeated by enough people, is almost impossible to combat....
"In 1963, we proved at the autopsy table that President Kennedy was struck from above and behind by the fatal shot. The pattern of the entrance and exit wounds in the skull proves it, and if we stayed here until hell freezes over, nothing will change this proof. It happens 100 times out of 100, and I will defend it until I die. This is the essence of our autopsy, and it is supreme ignorance to argue any other scenario. This is a law of physics and it is foolproof--absolutely, unequivocally, and without question. The conspiracy buffs have totally ignored this central scientific fact, and everything else is hogwash. ***There was no interference with our autopsy, and there was no conspiracy to suppress the findings.***" -- Dr. James J. Humes; October 1991
Sounds as if Humes, in his old age and possible senility, was actually beginning to believe the charade he participated in was reality. How sad.


{kind=link}
Any prevailing theories on the back wound?
in JFK Assassination Debate
Posted
"Curiouser and curiouser" or "Here we are going down the rabbit hole....."