

Robert Prudhomme
-
Posts
4,105 -
Joined
-
Last visited
Content Type
Profiles
Forums
Events
Store
Posts posted by Robert Prudhomme
-
-
Thanks for answering my question, Pat.
So Humes raised the back-wound location so that it could be associated with the throat wound. But alas he didn't raise it enough, so the WC had to raise it further.
But why didn't Humes raise it higher to begin with? I suppose because then it wouldn't have jibed at all with what witnesses had seen and were recording about the wound.
Yeah, that makes sense.
Only if you're desperate to claim the autopsy photos are fake. To my way of thinking, the back wound in the photos proves the lie orchestrated by Ball and Specter at Warren's urging. It proves the lie, and disproves the SBT.
Good point.
Well, except, the photo in question must have been altered given that the hole in the shirt doesn't line up with the wound shown on the back. I very much doubt that a shirt rises up with a jacket when raising a hand. It doesn't on me.
The hole on the back was 14 cm down from the bottom tip of the mastoid process. The hole on the clothing was measured at 14 cm below the top of the collar. So...could the bottom tip of JFK's mastoid process have come into alignment with the top of his collar, while he was sitting against the back seat of a limousine? I don't see why not. I tried this on myself and came away convinced that it makes sense.
No one has proven otherwise, that's for sure. For all their bluster, those holding that the clothing measurements prove the autopsy photos a fake have never done a series of re-enactments using clothes marked 14 cm below the top of the collar. There's a reason for that, IMO. It's because the clothing measurements are consistent with a wound at T-1.
Now, to my way of thinking, this ought to fill them with delight. This proves the drawings created for the Warren Commission, which moved the wound up to about C-5, even though the simplest of re-enactments involving the clothing would have proved the wound to have been around T-1, to have been a sham. But no, instead of marveling at the hubris of the Warren Commission, and Arlen Specter in particular, those pushing that the bullet entered at T-3 have chosen to act as though my failure to march in lockstep with their theory is the problem.
Pat,
I haven't studied the location of the back wound in great detail. But it's quite obvious to me that the location of the wound on the back photo is significantly higher than the hole location on the shirt.
Is it? Or is the fact JF's head is pulled back a great amount creating an illusion in that photo, in which the hairline appears to be much closer to the wound than it would be normally?
-
According to Pat Speer the base of JFK's neck was a quarter inch or so above the bullet hole in the jacket.
Could anything be more obviously fallacious?
No, I don't think so. I'm baffled by a few other things I've seen recently on this thread, too.
-
Compare this very accurate drawing

to the drawing you originally posted
The superior angle of the right scapula, in your drawing, appears to have been grossly exaggerated, placing it higher than the acromial process (acromion) of the shoulder, when, in fact, it is actually much lower.
Everything in the world looks different when viewed not only from behind, but also from a different angle.
--Tommy

Wrong. The scapula depicted in James' diagram is a gross distortion of the real thing. Period. If you can't see that, I don't know how to help you.
-
Robert,
I am not adjusting my position. When I entered this conversation it was to suggest that Pat Speer was more correct than you.
I am not able to explain the anomalies with regard to that skeleton. The 3D model whose image I used, makes clear that the "superior angle" is indeed close to T1.
This model is very accurate.
I have no intention of entering into an endless conversation. If you are insistent that you are right - no problem. All I am saying is - from my perspective - it appears to me that Pat was more correct than you.
James
I just CLEARLY demonstrated how GROSSLY exaggerated your diagram's scapula is.
Your only response is that you don't understand how ALL of your diagrams and photos are exaggerated, and that now you just don't want to discuss this matter any further?
-
Robert,
I have no idea of the cause of it looking like that.
I should have added. That although it is a real skeleton it has also been rebuilt. That might be the reason.
James.
Is this your way of admitting you are wrong, and that T1 is nowhere near the superior angle of the scapula?
-
Compare this very accurate drawing
to the drawing you originally posted
The superior angle of the right scapula, in your drawing, appears to have been grossly exaggerated, placing it higher than the acromial process (acromion) of the shoulder, when, in fact, it is actually much lower.
-
Robert,
If you are talking about the skeleton in post 271, that is a real skeleton.
It may be that adjustments had to be made when it was constructed.
James.
If that is a real, untouched photo of a skeleton, why is the scapular ridge (spine) lying horizontal, instead of running upward at an angle to the shoulder, as seen below?

-
Baloney! Show me one doctor who would measure a back wound from the top of the head. I've never heard of such nonsense. Why not just measure from the bottom of the heels? Makes about as much sense.
Now, look at your diagram, specifically the left hand drawing made by Boswell and showing the back wound well below the collar AND equi-distant from the mastoid and acromion processi. There is a very good chance we are saying the same thing, but just not communicating properly with each other. Do you believe the entrance wound depicted by Boswell in the Autopsy Face Sheet made on 22/11/63 was at the level of T1 or T3?
Also, are you saying that the collar of a suit jacket is normally at the level of the earlobes? Plus, how did you know the mark on your back was precisely where the entrance wound was in the photo? What did you use for landmarks?
I'm sorry to report, Robert, that you're misinformed regarding autopsy protocol. The currently accepted norm is to measure all wounds from the top of the head.
Source (among others): the template provided for wound descriptions on page 354 of Autopsy Pathology: a Manual and Atlas (2009).
The doctors I've spoken with must not have read that book. They all agree with Cliff Varnell, in that the spine is the appropriate landmark to measure back wounds from.
-
Robert,
I am not sure what you are getting at about the right scapula?
James.
You're just not looking closely enough. There is something drastically wrong with the right scapula in this photo.
The scapular spine is horizontal in this photo, contrary to its normal upwardly climbing angle, as seen below.
By turning the scapula to put the scapular spine in a horizontal position, the superior border of the scapula has been moved much higher up on the back. This is a very strange depiction of a thoracic skeleton.
-
Also, look at your diagram
and compare the scapula to this photo of a real scapula:
Do you see how the artist of your diagram has exaggerated the superior border of the scapula, placing it as high (or higher) as the acromial process? If we use the scapular spine as a guide, we can see the actual superior border is nowhere near as high as your drawing depicts.
-
James
Look at your photo of the thoracic skeleton. Do you see something odd about the scapula on the right?
-
Robert,
I use an app called “Anatronica.”I find it very helpful and mostly accurate.
My main textual reference book is “Principles of Anatomy & Physiology” by Gerrard J Tortora and Bryan Derrickson.
The two images below from “The Brief Atlas of the Skeleton” that comes with the set.
Link to Skeleton:-
The Skeleton – which is clearly a real skeleton – suggests that the “superior angle” may actually be closer to T1 than T2
As regards the Scapular, from what I can see your “superior angle” does seem a little flat and not as sharp as it should be. That may account for some of the difference. Also the atlas appears to use real bones to describe an anatomical feature. Your images appear to be drawings.
Link to Scapular:-
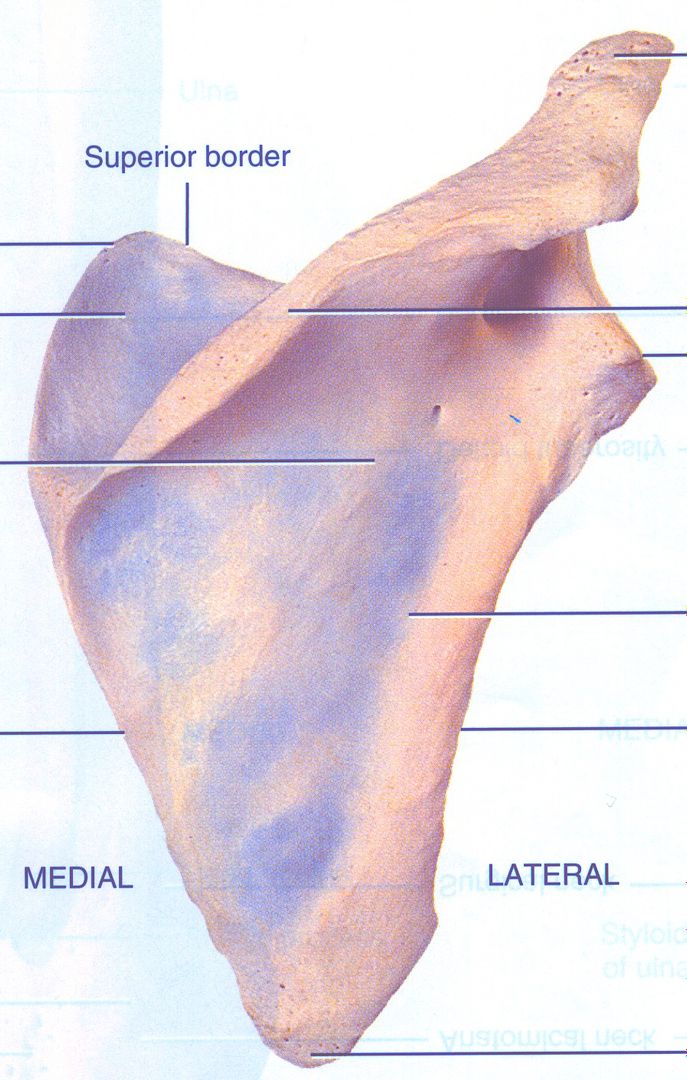
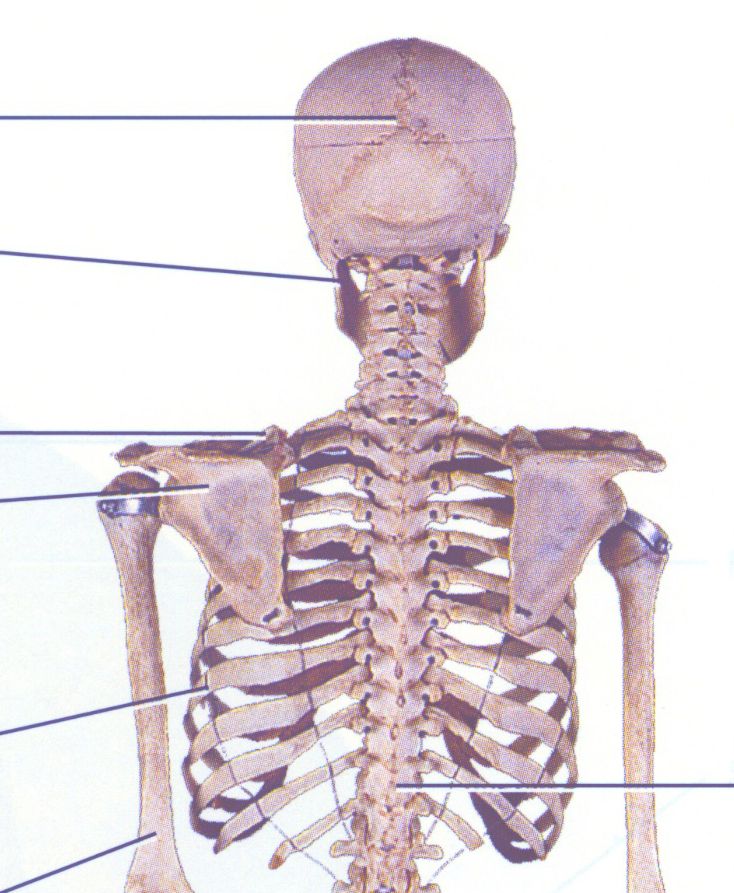
Photo of real human skeleton. Note location of the upper borders of scapulae a substantial distance below T1 vertebra.

-
Robert,
I am sorry, but Pat's diagram is much more accurate in describing the placement of T1 than your diagram.
In your diagram the Superior angle is between T3 and T2 when actually it is between T2 and T1. Essentially T1 is just above the Superior angle.
Where did you find that diagram, James? These diagrams below seem to disagree with your diagram.



-
FWIW, Cliff, you really should stop pretending T-1 is at the base of the neck.
T-1 is most definitely not at the base of the neck...which is why the HSCA's trajectory panel turned around and moved the wound back up to the base of the neck.

What is amusing about this HSCA drawing is how it portrays the T1 vertebra (bottom vertebra in their drawing) as being on the same level as the top of the scapula (shoulder blade).
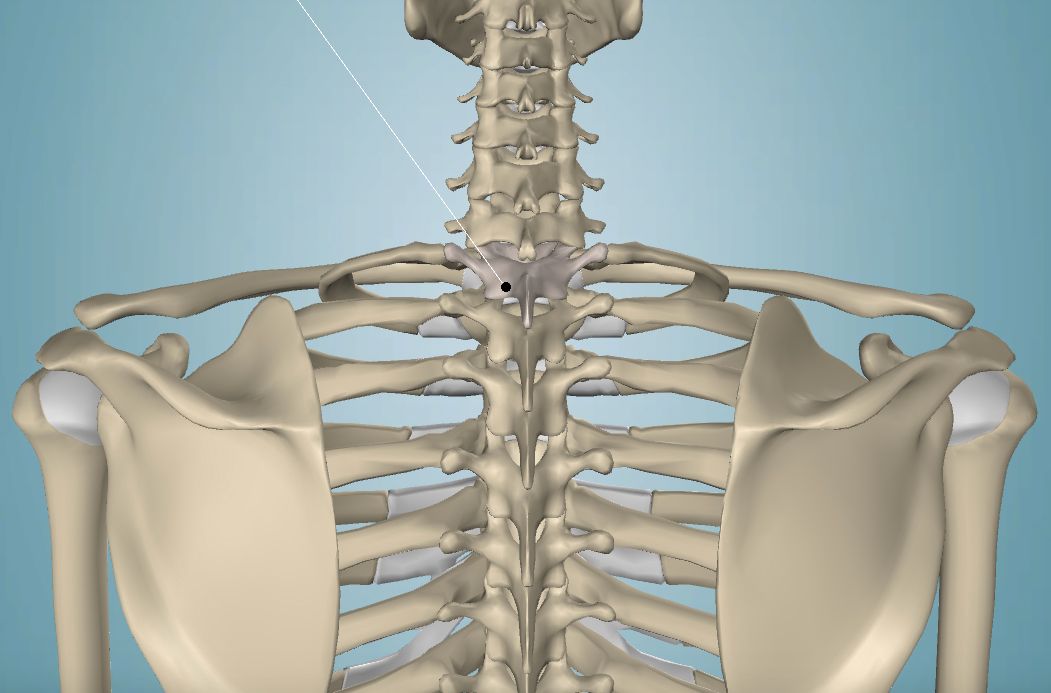
Here is a diagram showing a much more accurate placement of the T1 vertebra and the scapulae:

T1 is the first vertebra, below the cervical (neck) vertebra, that has ribs attached to it.
The HSCA drawings were created to deceive the public.
-
Baloney! Show me one doctor who would measure a back wound from the top of the head. I've never heard of such nonsense. Why not just measure from the bottom of the heels? Makes about as much sense.
Now, look at your diagram, specifically the left hand drawing made by Boswell and showing the back wound well below the collar AND equi-distant from the mastoid and acromion processi. There is a very good chance we are saying the same thing, but just not communicating properly with each other. Do you believe the entrance wound depicted by Boswell in the Autopsy Face Sheet made on 22/11/63 was at the level of T1 or T3?
Also, are you saying that the collar of a suit jacket is normally at the level of the earlobes? Plus, how did you know the mark on your back was precisely where the entrance wound was in the photo? What did you use for landmarks?
-
It is a preposterous idea that the wound is at the level of T1/C7. The image itself may be vague, but the geography of the body is very clear where the hole is located. I suspect it is slightly above T3, but it would be perfectly possible to argue it was at the level of T3
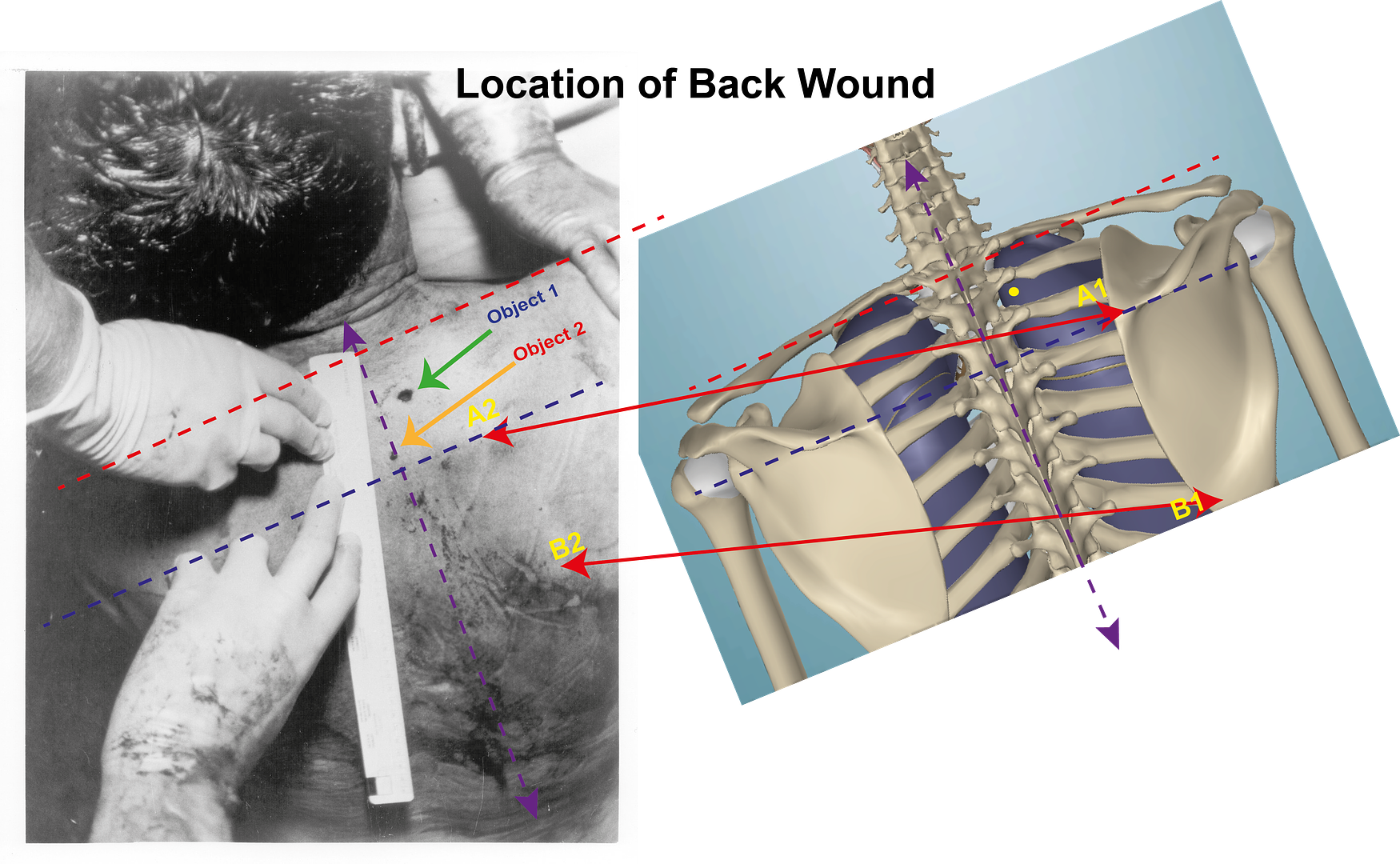
Object 2 is the blood spot.
On the back of JFK you will see two labels in yellow A1 + B1. Between these two labels and below the B1 label you will see an outline shape underneath the skin. The shape that is being seen is the outline of part of JFK’s right Scapula.
If you look at the anatomical model that is to the right of the image you will see the complete Scapula on the skeleton. The two labels A1 + B1 in cyan on the skeleton point to these same parts that can be seen through JFK’s body that are labelled A1 + B1 in yellow.
The A1 point is at the Medial edge of the Scapular spine. The Scapula spine is that ridge crossing the Scapula and the Medial edge is the edge of the Scapula nearest the vertebral column.
In order to gain a reference by which to judge the location of the wound, I have drawn a blue line across the model as well as the body from this A1 point. Having done that I now have a base line on the body. This base line is midway between T3 and T4.
If you look at the upper right corner of BE 5, you will see the right hand of Commander Boswell holding JFK’s shoulder. I am assuming that it is Humes doing the measuring. I have tried to guess where Costa IR is on the JFK’s body and have drawn a red line across the body, as well as on the model, signifying where I believe Costa IR is. I accept that, this line signifying the position of Costa IR might be slightly out, but it will not be very far out. This red line now gives me an upper limit beyond which this wound is not located.
What can be said, for certain, is that the wound lies between those two lines. If you look at Boswell’s right hand [ I assume it is Humes that is measuring ] you will see that the nail of his pinkie, just to the right of the label A1, is roughly on the same plane as the wound.
I suspect the position of this wound is above T3 but below T2. One thing is for certain it is nowhere near C7/T1.
Hi James
Well done! I couldn't have explained things any better than that.
I'm finding it a bit difficult to believe how many years we have been looking right at a photo of a bullet hole near the level of T3, and have believed it to be at C7/T1, simply because that is where Humes told us it was. As you say, the spine of the scapula is the only really prominent landmark in that area, and there is no mistaking it in that photo.
Humes never "told us" the wound was at C7/T1. He and Boswell prepared a face sheet that placed it around T-1, and provided measurements which placed it around T-1. When asked to create drawings for the Warren Commission, however, they catered to the commission's concerns this wound was too low to support the single-assassin conclusion, and prepared drawings placing it around C-5. The Johnson Administration then pressured them into standing by these drawings. In 1978, however, the HSCA decided to publish a tracing of an autopsy photo which proved these drawings to have been in error. They concluded that the wound was at T-1, and reflected in this in their exhibits. There was a problem with this, however. A bullet headed downwards from the sniper's nest and striking Kennedy in this location would have smashed right into bone, or lung. This then led some single-assassin theorists (such as John McAdams) to start claiming the HSCA claimed the bullet entered at C7/T1. This allowed them to pretend this bullet sailed over the first rib at T-1. I spotted this, moreover, and began correcting McAdams and others whenever the opportunity arose. I even corrected Wikipedia on this point.
So, in sum, the T1 entrance was not something proposed by Humes, but something presented years later by the HSCA which proved Humes to have lied when he pretended the entrance was at C-5. And it is not something proposed by single-assassin theorists, who either insist the HSCA was wrong, and that the bullet entered higher, or pretend the HSCA concluded the entrance was at C7/T1, and not T-1, as depicted in the HSCA's exhibits.
Unfortunately, the entrance wound in the photo still appears to be two finger widths (or slightly less) above the plainly visible scapular spine, placing the entrance wound just above T3 vertebra. If it was at the level of T3, it would have struck the 3rd rib.
-
Thanks for answering my question, Pat.
So Humes raised the back-wound location so that it could be associated with the throat wound. But alas he didn't raise it enough, so the WC had to raise it further.
But why didn't Humes raise it higher to begin with? I suppose because then it wouldn't have jibed at all with what witnesses had seen and were recording about the wound.
Yeah, that makes sense.
Only if you're desperate to claim the autopsy photos are fake. To my way of thinking, the back wound in the photos proves the lie orchestrated by Ball and Specter at Warren's urging. It proves the lie, and disproves the SBT.
Good point.
Well, except, the photo in question must have been altered given that the hole in the shirt doesn't line up with the wound shown on the back. I very much doubt that a shirt rises up with a jacket when raising a hand. It doesn't on me.
The hole on the back was 14 cm down from the bottom tip of the mastoid process. The hole on the clothing was measured at 14 cm below the top of the collar. So...could the bottom tip of JFK's mastoid process have come into alignment with the top of his collar, while he was sitting against the back seat of a limousine? I don't see why not. I tried this on myself and came away convinced that it makes sense.
No one has proven otherwise, that's for sure. For all their bluster, those holding that the clothing measurements prove the autopsy photos a fake have never done a series of re-enactments using clothes marked 14 cm below the top of the collar. There's a reason for that, IMO. It's because the clothing measurements are consistent with a wound at T-1.
Now, to my way of thinking, this ought to fill them with delight. This proves the drawings created for the Warren Commission, which moved the wound up to about C-5, even though the simplest of re-enactments involving the clothing would have proved the wound to have been around T-1, to have been a sham. But no, instead of marveling at the hubris of the Warren Commission, and Arlen Specter in particular, those pushing that the bullet entered at T-3 have chosen to act as though my failure to march in lockstep with their theory is the problem.
Pat
You're not making sense. One second you are saying the wound was 14 cm. down from the tip of the mastoid process, the next second you are saying the hole in JFK's suit was 14 cm. below the top of his collar. Then you go into something about the mastoid process and the top of his collar lining up during the assassination, and that this somehow proves (in your mind) that the wound was at the level of T1.
Sorry, Pat, it doesn't work that way. First, the use of the mastoid process as a landmark was a complete joke, and several physicians I have spoken to say quite clearly that a landmark on the skull would NEVER be used to pinpoint a back wound. It would make far more sense to use landmarks located on the back itself. The use of the mastoid and acromion processi was clearly done to spread as much confusion as possible.
Second, if the mastoid process was used as a landmark, it would be with JFK's head and body in the anatomically neutral position. This does not mean that, in order to make your theory work, you are allowed to bend JFK's head back until his mastoid process is touching his collar.
Further, do you really believe that a bullet entering JFK's coat (and back) 14 cm. (5.5 inches) below his collar is going to leave an entrance wound at the level of T1 vertebra? SERIOUSLY??
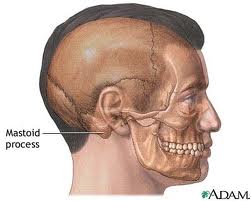
See the mastoid process, just behind and at the same level as the earlobe? Bit high for a suit collar, wouldn't you say?
-
Robert,
If you are suggesting that the source of the shot is the TSBD, then both:-
a) The angle Connally has turned at that point approx 35-40º
AND
 The angle of the bullet through the body.
The angle of the bullet through the body.Prohibits it.
Use a map of the plaza. Place Connally as he is positioned in the car and then draw a line along the angle of the 5th rib and project backwards.
That way you will see the source is somewhere between the Daltex and the Records building
Hi James
Below is Frame z223 of the Zapruder film, and below that is Frame z255.


Look closely at these two frames, and then look at the Altgens 6 photo below.

As we know the Altgens photo was taken at the same time as Frame z255 of the Zapruder film, we can make comparisons from it. If you look at z255, you can see that JBC has turned roughly 90° in his seat. In this position, I could believe JBC was shot from a position between the Dal-Tex and the County Records Buildings. However, at z223, I do not see JBC turned 35-40° to his right. I can see him turned very slightly to his right, possibly to look at TUM, but he is barely turned more than Kellerman and, by all accounts, Kellerman was facing forward at this time.
In case I have been misunderstood, it is my contention, understanding what I do about JBC's chest wound, that if JBC was shot from the SE corner of the TSBD, he had to be turned much further to his right than he was at z223. Of course, this completely excludes any firing position further east of the TSBD, such as between the Dal-Tex and the County Records Buildings.
The other problem with JBC being shot at z223 is that his right arm just happens to be covering the mid axillary line of his chest. Once again, I refer you to the interview Dan Rather gave after viewing the Zapruder film on 25/11/63. The part about JBC being hit starts about 1:27.
Dan Rather clearly describes JBC turning back toward JFK with his right hand extended outward toward JFK, and that this was the moment JBC was hit. This was echoed in the WC testimony of Sam Holland, a witness standing atop the Triple Underpass at the time of the shooting:
"Mr. HOLLAND - And she was looking in this direction [indicating].
Mr. STERN - "She," is Mrs. Kennedy?
Mr. HOLLAND - His wife. And about that time---
Mr. STERN - Was looking in a southern direction?
Mr. HOLLAND - In the southern direction.
Mr. STERN - South side of Elm Street?
Mr. HOLLAND - And about that time he went over like that [indicating], and put his hand up, and she was still looking off, as well as I could tell.
Mr. STERN - Now, when you say, "he went like that," you leaned forward and raised your right hand?
Mr. HOLLAND - Pulled forward and hand just stood like that momentarily.
Mr. STERN - With his right hand?
Mr. HOLLAND - His right hand; and that was the first report that I heard.
Mr. STERN - What did it sound like?
Mr. HOLLAND - Well, it was pretty loud, and naturally, underneath this underpass here it would be a little louder, the concussion from underneath it, it was a pretty loud report, and the car traveled a few yards, and Governor Connally turned in this fashion, like that [indicating] with his hand out, and another report.
Mr. STERN - With his right hand out?
Mr. HOLLAND - Turning to his right."
Sam Holland also corroborates Dan Rather's observation that JFK's right hand was raised at the moment the first shot struck him.
Clearly, we do not agree about the nature of JBC's chest wound, or about the moment he received the chest wound. The Zapruder film has also clearly been altered.
What is most interesting about Dan Rather's account is that he claims JBC was knocked over by the shot, and that Nellie Connally immediately covered JBC with her own body. During interviews, JBC is quite adamant that the shot that hit him was powerful enough to knock him over. What a coincidence, and how very strange we do not see JBC knocked over at Frame z223 of the Zapruder film.
-
"
The trajectory of the bullet through Connally's body prohibits a shot at Z223/4 - which I assume you are suggesting. As I have pointed out many times before, the source of a shot at Connally at Z223/4 is somewhere between the DalTex building and The Records building. Looking at frames after 223/4 we see Connally's hand rise with his palm towards his chest. The injury Connally sustained could not be achieved if his palm was towards his chest." I cannot see how you have come up with this location for the source of the bullet that caused JBC's chest wound, if you believe JBC was facing forward when struck in the chest. Dr. Robert Shaw clearly states that the bullet entered at the "mid axillary line" and exited just below and MEDIAL to the right nipple. Once again, for clarity, "medial to the right nipple" means somewhere between the right nipple and the centre of JBC's chest.
One more time, the mid axillary line:


Taking into account the position of the mid axillary line, and the position of the nipple, this bullet almost travelled sideways across JBC's chest. If JBC was facing forward at the time the bullet hit him, it would have to be travelling, if measured from a line running lengthwise through the centre of the limo, at an angle of 45° measured from the line running through the centre length of the limo.
This is why the SBT is an absurdity, and why JBC could not have been shot from directly behind the limo, UNLESS he was turned far to his right at the moment he was shot.
COINCIDENTALLY, this is exactly the position Dan Rather claimed JBC was in when Rather viewed the Zapruder film shortly after the assassination. Oh, and Rather saw him extending his right arm toward JFK, something also witnessed by someone on the Triple Underpass, explaining why the bullet, travelling at such an angle, did not hit his arm.
-
I hate to disagree with you James but, the very mechanism that causes a frangible bullet to break up is the very reason it may have survived reasonably intact from its tangential contact with Connallly's rib.
Frangible bullets are normally made from powdered metal that is either compressed, glued or "sintered" into the shape of a bullet, although it appears the frangible range bullets made for the 6.5mm Carcano since the 1930's, designated as the M37 "Magistri" frangible bullet, were made with uncompressed powdered lead in a copper alloy jacket; with a tiny lead or "maillechort" solid pellet just inside the nose of the bullet. From the cutaway photos I've seen of the M37, the powdered lead appears to be quite coarse.
While lethal frangible bullets made for hunting and law enforcement differ slightly in their construction from frangible range bullets, such as the M37, frangible bullets all have one thing in common; they will disintegrate back to the powder they were made from if they impact a very hard surface, such as steel, concrete or stone. They are more than capable of penetrating bone and remaining intact, such as a human or a deer skull, but there are reports of them disintegrating if they impact a large, thick or particularly hard bone.
The 5th rib is neither hard enough nor thick enough for a frangible bullet to disintegrate simply by impacting it with a tangential blow.
The only way for a frangible bullet to have disintegrated by impacting the 5th rib tangentially is if it possessed the one feature that all modern frangible bullets possess. That feature is a hollow point nose. As I have tried to explain countless times on this forum, it is not striking bone that gives the lethal frangible bullet such deadly results. Just like the standard hollow point solid lead bullet, it is when it travels through semi-liquid tissue that the frangible bullet is at its deadliest. Quite simply put, semi-liquid tissue fills up the hollow nose of the bullet and exerts tremendous hydraulic pressure on the compressed core of the bullet, to the point the compressed core can no longer withstand the pressure and disintegrates into a cloud of powdered metal.
Frangible bullets are available both jacketed and unjacketed. If jacketed, the solid remains of the jacket will still be visible. If not jacketed, only powder remains.
I have no idea whether or not the bullets that struck JFK and JBC were jacketed, nor do I know if they had hollow point noses, or if their cores were plain powdered lead, or compressed lead. While the M37 bullet was considered a "safe" frangible bullet for use in indoor ranges, its safety was based on the fact that a concrete wall was placed behind the target area and, instead of ricocheting when the bullets struck the concrete, they would disintegrate into powder. I have no idea what would happen to one of these M37 frangible bullets if it was fired directly at someone's head.
If the frangible bullet that caused JBC's chest wound did have a hollow point nose, the question is, why did it not behave as it should passing through 10 cm. of JBC's rib? The answer may be that the epidermis and bone it went through was not liquid enough to fill the hollow point and exert sufficient pressure on the core of the bullet to cause it to disintegrate.
As the bullet only went through JBC's shirt cuff, and not the cuff of his mohair suit, the fibres Gregory described, in JBC's wrist, could only have come from its passage through the front and back of the suit. The "star" shaped hole in JBC's shirt cuff is also no indication of the condition of the bullet that made the hole, especially if that bullet struck tangentially, instead of square on. There is indication of a partially tangential blow in that the wound on JBC's wrist was quite a bit longer on one axis than the other. A good way of explaining this is to look at paper targets at a shooting range. Instead of making neat little round holes, bullets tend to tear their way through paper targets. This is one reason why "wadcutter" bullets were invented.
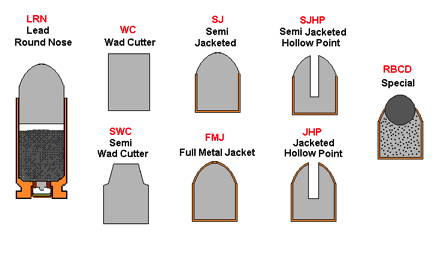
Wadcutter bullets have a square nose, as seen above, and make a perfect round hole when passing through a paper target; something that is only of any concern to competition shooters.
As the wound data from JBC's chest wound clearly tells us, the bullet traversed the front of his chest at about a 45° angle. This means one of two things:
1. The bullet that struck JBC's chest did not originate from the east end of the TSBD but, rather, came from much further west in the TSBD.
or
2. JBC was turned to his right in his seat by at least 35-40° when he was struck by the bullet; something we do not see in the Zapruder film until long after JFK is struck in the back.
With this in mind, is it really fair to say JBC's right wrist was not in line with his chest wound, when we have no clear idea when JBC was shot in the chest?
-
I agree about the bullet not tumbling, as Dr. Robert Shaw goes into some detail describing how the intercostal tissue, above and below the path of the bullet through the outer surface of the 5th rib, was left relatively untouched. Considering the narrowness of the rib at this point, this would suggest a non-tumbling bullet flying straight and true. I have always found it somewhat miraculous, though not unbelievable, that the bullet followed the precise downward angle of the 5th rib for the entire time it was in contact with it.
As to whether or not the bullet that caused Connally's chest wound was a frangible bullet, this is a point I am still leaving open for consideration, as there are several features regarding frangible bullets that might just make them possible candidates for this. I will go into this in the next post.
As you and I both know, and as you stated in (E) above, the material encountered by the bullet, in its circuitous path around Connally's chest, would not have greatly reduced the velocity of this bullet. With this in mind, we then must consider the severity of the wound in Connally's wrist. For those not familiar with the wrist wound, a bullet struck just above Connally's right wrist, hitting squarely on the back of the radius bone and breaking it into several pieces. It, or a fragment of it, either went through the radius bone or between the radius and ulna bones, and exited the bottom or palm side of his forearm through a tiny hole that was much smaller than the entrance wound.
I believe that it was Dr. Shaw that testified that such a wound from a rifle bullet, at normal velocities, would typically have destroyed the radius bone, and amputation might have been the only medical solution. As we are both aware, the wrist wound either was from the bullet that injured Connally's chest, or was from a totally separate bullet. In either case, shouldn't we have seen far more damage to the wrist?
-
As an afterthought, I thought I would share with everyone how the average person can deal with an open pneumothorax, should you come across a person with one and you just don't happen to have an Asherman Chest Seal in your back pocket. With the number of crazies running around with firearms these days, it is probably a good thing to know.
Pictured below is something referred to as the "Three Sided Dressing", and it can be made from a good quality plastic bag and a roll of tape. If the patient is one of those hairy "gorillas", you may have to shave a small area around the wound to get a good seal.

The opening in the chest is obvious here, and the plastic has been applied with that opening directly in its centre and then taped and sealed on three sides. The open side of the plastic is on the bottom side of the dressing to encourage any blood expelled from the wound to run downhill and out of the dressing, instead of accumulating inside the dressing.
How it Works
When the patient breathes in, his diaphragm moves downward and creates a vacuum in his chest cavity. Atmospheric air, with a pressure of 14.7 psi at sea level, rushes in through the trachea to fill the lungs and occupy this vacuum. With a hole in the pleura, air travels through the pleura to fill this vacuum and fills the pleural cavity, preventing the lung from filling and causing it to collapse. The plastic sheet of the Three Sided Dressing, or T.S.D., gets sucked against the skin of the chest during inhalation, sealing the wound, and prevents this, allowing the lung to fill.
Now, if it was that simple, you could just tape the dressing down on four sides, and pack the guy off to the hospital before he bleeds to death internally. The problem here is that whatever put a hole in his pleura has also very likely put a hole in his lung. When he inhales, our plastic dressing now allows the lung to inflate. If there is a hole in the lung, it will only partially inflate, and air will be pulled through the hole in the lung into the pleural cavity. When he exhales, the lung will collapse again, sealing off the hole in the lung and trapping the air in the pleural cavity. This is how an open pneumothorax can evolve quickly into a tension pneumothorax.
The solution is, of course, not to tape the bottom side of the dressing. When the patient exhales, the plastic moves away from the skin and allows the venting of any built up air pressure in the pleural cavity out through the open side of the dressing. As I stated earlier, it is important to leave the open side of the dressing on the downhill side to allow for drainage of blood.
It is actually quite fascinating to watch one of these dressings in action in the field as it pops open and closed, and it is very gratifying to the first responder to see such a simple dressing transform a patient's condition so rapidly in a matter of seconds.
P.S.
When dealing with chest wounds, especially those made by bullets, ALWAYS check the opposite side of the chest from the wound you have found for another wound. It is quite common to find entry and exit wounds in the chest (or multiple wounds) when dealing with a patient suffering a gunshot wound.
-
The first misconception, and one held by a surprising number of researchers, is that Connally suffered a "through and through" bullet wound to the right side of his chest. The reason for this belief is that Connally had a wound on his back and a wound just below the right nipple AND he had an open pneumothorax in his right lung cavity. However, even with these three established facts, it is also an established fact that a bullet never entered his right lung. I will attempt to explain.
Before I explain that, though, I should point out that while I believe JFK had a "tension" pneumothorax in his right lung, Connally most definitely had, in his right lung, an "open" pneumothorax or "sucking" chest wound. While the two are close cousins, there is a difference. In many instances, the two will have the same cause, such as a bullet piercing the pleural cavity and making a hole in the balloon known as the lung. In JFK's case, his condition was likely an open pneumothorax right up until they laid him on the ER table in Trauma Room One. At that point, the weight of his upper back pressing against the table likely sealed the opening, and created a tension pneumothorax. In Connally's case, the opening in his pleural cavity was more toward the front of his chest, to the point he would not be lying on it if he was on his back and it would remain open to the atmosphere. However, the open pneumothorax is just as dangerous as the (I'm going to start referring to the pneumothoraxes [actually pneumothoraces] as "O.P." and "T.P." to save myself a bit of typing) T.P., and, if not dealt with quickly, can lead to the demise of the patient. The best treatment for an O.P. is to seal the opening in the chest, and even a hand with a rubber glove over it is adequate. But, if the lung is compromised, as well as the pleural lining, and the seal on the chest is not removed periodically, building air pressure in the lung will quickly transform the O.P. into a T.P., and the patient may die anyways.
If I had been on an ambulance in Dallas that day and Connally was my patient, this is the thing I would have applied over the opening in his chest to seal it:

Asherman Chest Seal
The Asherman Chest Seal, or ACS, is an adhesive dressing to be placed over the opening in the chest causing an O.P. There is an opening in the centre of the adhesive section of this dressing that corresponds to the "stem" in the centre. If the opening into the pleural cavity is greater than the diameter of the ACS, such as from a laceration, the majority of the opening should be sealed with tape (duct tape works great if nothing else is available. remember, a life is at stake; worry about sterile dressings and infection later), leaving only an opening large enough for the vent of the ACS. The funny looking "stem" of the ACS is actually a vent, and also acts as a "check" or "one-way" valve. Any air pressure in the pleural cavity is enough to open this stem and allow air from the pleural cavity to vent to the atmosphere. When the patient breathes in, creating a vacuum, the stem instantly flattens, sealing the pleural cavity from outside air and allowing the lung(s) to expand.
As I said, it is a popular misconception that a bullet went through John Connally's right lung, and this was the cause of the O.P. he suffered. In actuality, a bullet entered the side of his right chest at the mid axillary line.
This bullet precisely followed the outside of the downward coursing 5th rib for 10 cm. (4 inches), before exiting just below and medial to Connally's right nipple. For those not familiar with medical references, medial means toward the centre of the body. In other words, the exit wound was actually between the right nipple and the centre of his chest.
To put this in simpler terms, Connally was hit with a grazing shot that was only a centimetre or two away from missing his chest altogether. Also, the path of the bullet was not from an origin anywhere near JFK, unless Connally was almost completely turned sideways toward JFK when he was hit. The proof of this is that a bullet entering the flesh at the mid axillary line, and exiting medial to the right nipple, is obligated to follow almost a 45° angle across the front of the chest to do so.
The 5th rib is quite soft at this point, and would have offered little resistance to the bullet. However, it would be just brittle enough for the bullet to shatter fragments from this rib, and it was these shards of the 5th rib that tore through the pleural lining, creating the O.P. This is how Dr. Robert Shaw described it in his medical report:
"The plura had been torn open by the secondary missiles created by the fragmented fifth rib."
http://mcadams.posc.mu.edu/russ/jfkinfo/app8.htm
Now, I'm sure it has occurred to you that the ribs are curved, and you are probably wondering how a bullet flying in a straight path could follow the curve of a rib for 4 inches. Well, it did, and the explanation for this can be found in Dr. Shaw's medical report, as well as in his WC testimony.
Dr. Shaw observed that the 5th rib actually seemed to be depressed into the pleural cavity, when compared to the 4th and 6th rib, and it was his understanding the force of the passing bullet actually depressed the rib inward, partially straightening it. Confirmation of this was the discovery the 5th rib had also suffered a stress fracture near the back end of the rib, just out from where it attached to the 5th vertebra. In other words, the force of the rib straightening out was great enough to snap the far other end of the rib where it attached to the backbone.
So, the question is, if the bullet that caused this wound was a frangible bullet, would this contact with the 5th rib be enough to cause the frangible bullet to disintegrate?
-
I'm curious about two issues:
1. if no shot came from the rear and hit JFK in the back then what do we make of the round or rounds that hit JC?
2. if frangible or exploding bullets did hit JFK in the back and disintegrated in the lung then how did a different type of round apparently hit JC?
I'm not entirely comfortable separating the two men's injuries and attributing them to separate shooters firing different loads. How does the shooting scenario "play" out in your minds?
Excellent questions, and ones that have kept me awake a few nights trying to answer.
To answer these questions, we have to take a hard look at Connally's wounds, and put the lie to the many misconceptions surrounding his wounds. In the process of doing this, the true nature of Connally's wounds will be seen, and the absurdity of Arlen Specter's Single Bullet Theory will also be revealed. It might take several posts to cover everything.





 The angle of the bullet through the body.
The angle of the bullet through the body.
Any prevailing theories on the back wound?
in JFK Assassination Debate
Posted
Look closely at this photo of the anterior surface of the left scapula, seen in the same Wikipedia article you linked to:
Now compare the level of the acromion to the superior angle, in this photo, to the same level of acromion to superior angle in the drawing provided in the same article:
Can you see the difference? In the photo of the scapula, the acromion is much higher than the superior angle, yet, in the drawing, the superior angle is as high as the acromion; placing the superior angle falsely at the level of the T2 vertebra. Further, this discrepancy cannot be explained away as being due to how much the scapula is rotated in relation to the rest of the body, as the scapula in the photo and the scapula in the drawing are essentially shown at the same angle.
The only difference here is that the artist has chosen to portray the superior angle of the scapula incorrectly in the way it relates to the rest of the scapula.