

Robert Prudhomme
-
Posts
4,105 -
Joined
-
Last visited
Content Type
Profiles
Forums
Events
Store
Posts posted by Robert Prudhomme
-
-
Robert Prudhomme,
This diary of yours, about autopsy landmarks, goes to the heart of the matter.
The photo you present is outrageous. It has been offered up many times. What does it tell a reasonable observer? Nothing. Yet it has been marched out out over 50 years as proving something. It proves nothing.
This may very well be true. On the other hand, this may actually be a photo of JFK's back. The only alteration may be the hiding of the large gaping wound in the right rear of JFK's head.
The entrance wound in the back may be genuine. When this photo was taken, there may not have been a need yet to move the back wound up to the level of C7/T1, from the real location at T3, to accommodate the throat wound as an exit wound. However, when this need arose, a careful study of this photo would tell the conspirators all they had to do was tell the public they were looking at a C7/T1 entrance wound, and the public would believe it. Why not? It seems to have worked quite well for all of these decades. Are you able to look at a photo of someone's back, especially one such as this with the head bent backwards, and pinpoint precisely where C7/T1 is located?
If the entrance wound is genuine, and that is JFK, this photo tells us a world of information.
-
Oops, just read a little closer. It's Retting, not Redding. My bad.
I'll see what I can do, Chris.
-
Well, I just spoke with Alex at the Martin B. Redding Inc. sales dept. He says they no longer regret the original purchase of the batch of Ordnance Optics Inc. 4 x 18 scopes, and that, with the rising price over the years, consider it now a very sound investment.
Alex seemed to be a very accommodating fellow, and took the time to retrieve one of these scopes from the shelf and remove the elevation and windage caps. Much to my disappointment, there was no "<UP-DOWN>" or "<LEFT-RIGHT>" on either of the adjustment screws.
He did say, though, that the lettering on the side of the scope looked more natural with the windage cap on the left, and that the lettering was actually upside down with the windage cap on the right. I guess we'll just have to go with that, and assume the Japanese manufacturers made a very unique scope with the windage cap on the left.
-
i said carousel club
Yes, I noticed, and without a capital "C"

You diverted thread topic by attempting to draw DVP in to a discussion about Tan Jacket Man, which has absolutely nothing to do with the topic of this thread.
As you diverted the topic, I decided to go along with it and post an irrelevant to the thread topic video on Lee Odom.for those who may be interested in discussing a possible match between Odom and TJM.
can't get a decent thread started on that dunc the button man, advertised saturated, cookie-riddled forum of yours? tsk-tsk.

-
From David Lifton:
"Finally, your argument about the chest tubes baffles me. One cannot substitute a theory about whether this or that person is a xxxx, with genuine anatomic evidence. Three doctors signed an autopsy report which made clear those tubes were not pushed all the way in. That's data which I respect--and certainly more powerful and substantive (as evidence) than a hypothesis as to whether someone who lied about "A" might also have lied about "B" (or not). etc."
The Parkland surgeons wrote medical reports a few hours after JFK was pronounced dead, and not only stated that a chest tube(s) was inserted, but that it was also connected to a sealed drain. Is this not data worthy of respect as well?
-
Three autopsy doctors also told the world there was not a large gaping wound in the right rear of JFK's head, yet this seemed to be the prevailing observation not only of Parkland witnesses but also of Bethesda witnesses. So much so, it was necessary to suppress the contents of the HSCA interviews with Bethesda witnesses, tell outright lies about these interviews and not reveal the contents of these interviews until the formation of the ARRB over a decade later.
Do you believe the autopsy doctors were truthful about everything? If you don't, how can you tell when they were being untruthful, and when they were not?
None of the surgeons at Parkland saw the back wound, for the simple fact that they never rolled him over. I know this may have been poor medical practice, as even we, as paramedics, are trained to do a ten second Rapid Body Search to determine the full extent of injuries but, our RBS does NOT involve rolling a supine patient into the prone or semi-prone position. Even if they had done a Rapid Body Search, it only involves quickly passing the hands under the back to look for bleeding. With the amount of blood present from the rear head wound, and the fact JFK was essentially pulseless, would this search have revealed anything? I don't believe so.
Under the circumstances, I believe the surgeons in Dallas can be forgive for not seeking out every single one of JFK's wounds. The Parkland surgeons were simply too involved with basic life support and critical interventions to begin turning JFK over to look for bullet wounds. They say this themselves in every interview they have ever given. Once their job was over, they quite naturally did not feel it was up to them to begin exploring JFK's corpse for any other wounds, and quite rightly so. This is why they have autopsies.
Why did the staff placing JFK into the coffin at Parkland not see the back wound. Quite simply, it was on the back, and they were not looking for a wound. How much rolling over of JFK's corpse would they have done? Lt. Lipsey described, in his HSCA interview, the great amount of blood caked onto JFK's upper torso, and how much time was spent by the autopsy doctors scrubbing through this blood, prior to examining JFK's corpse. Would the post-mortem staff at Parkland not also be looking at a blood caked corpse? Would a tiny entrance wound be discernible in such a mess?
What caused the damage to the right lung, and where did it go? An unjacketed frangible bullet entered the right pleural space at the level of T3 and entered the top of the right lung. As the bullet passed through intercostal and lung tissue, its hollow point nose filled with this tissue, exerting a tremendous pressure on the rest of the bullet. Shortly after entering the lung, this internal bullet pressure caused the frangible bullet to disintegrate into the metal powder from which the bullet was made, damaging the lung and leaving no large sized fragments for the autopsy doctors to find. If these doctors were genuinely unaware of the game afoot, and knew nothing about frangible bullets, they must have been seriously baffled by what they saw; so much so, they did not recognize grainy material on a chest x-ray as minute particles of a bullet, and chose to call it "dirt" instead.
-
I managed to find the post. The guy's name was Alex, and he works for the Martin B. Redding Co. Here is the full post:
"
Ordnance Optics Scopes.....the complete storyOkay guys, here's the complete story (as best I know) on the Ordnance Optics Scopes.
When Ordnance Optics went out of business, we (Martin B. Retting, Inc.) bought their remaining inventory of 4x scopes. From what I hear...it was a pretty big lot and the scopes were such poor quality that Jim Thompson (who was the mgr. at the time and responsible for the purchase) never heard the end of it.
For while the scopes were sold on the floor for use with .22 rifles, I think they were under $10.00 in the late 70's. I remember buying one as a kid for my 10/22.
Their more infamous role came when one of the scopes that we sold Kline's ended up on a certain Carcano.
Here are the fact as I know them to be:
a) there was only one lot of scopes sold off buy Ordnance Optics....but there were to slight variations within it. The one on Oswald's rifle had a knurled ocular lens bell housing. The remaining scopes have smooth ocular bell housings. Otherwise the markings are the same. there is only one type of mount, both the 3 hole and 4 hole started out the same. some mounts were ground to fit 95 mausers (in order to clear the bolt stop). the carcano should have had a four hole mount, with no need for grinding...but Kline's had both styles and simply installed the wrong one.
there is only one type of mount, both the 3 hole and 4 hole started out the same. some mounts were ground to fit 95 mausers (in order to clear the bolt stop). the carcano should have had a four hole mount, with no need for grinding...but Kline's had both styles and simply installed the wrong one.
c) the best photo of the rifle, for reference of the scope and mount, appears in the November, 1983 issue of Life Magazine. A photographer was allowed access to the Oswald rifle...the resulting photos show much more detail than the Warren commission pics.
d) the scopes themselves are horrible....very poor optically....very frail crosshairs! In addition, the crosshairs are not self centering, so depending on the rifle, the sight picture may be a little annoying. The mounts are also prone to bending. If I had to vote, I go along with the school of thought that argues that Oswald either used the iron sights or simply pointed the rifle by looking over the scope.
that being said, I have a few left...the price is $250.00 with mounts, plus $20.00 if you want Keith (the guy who as a kid, ground them originally) to grind the mount like the 95 mount. the actual availability issue isn't the scopes, it's the mounts..... which will run out before the scopes.
I used to advertise them occasionally, with a brief history and a certificate of authenticity, but I got tired of all of the hate mail that I would get... never ceases to amaze me how mean supposedly "enlightened" liberals can be if you're what they consider "politically incorrect"
anyhow.... if anyone ever has any question, you can call me at the shop. 310-xxx-xxxx....ask for Alex"I thought it best to hide the phone number for now, as I don't want this guy getting a flood of calls before I have a chance to speak to him again.
-
It is a preposterous idea that the wound is at the level of T1/C7. The image itself may be vague, but the geography of the body is very clear where the hole is located. I suspect it is slightly above T3, but it would be perfectly possible to argue it was at the level of T3
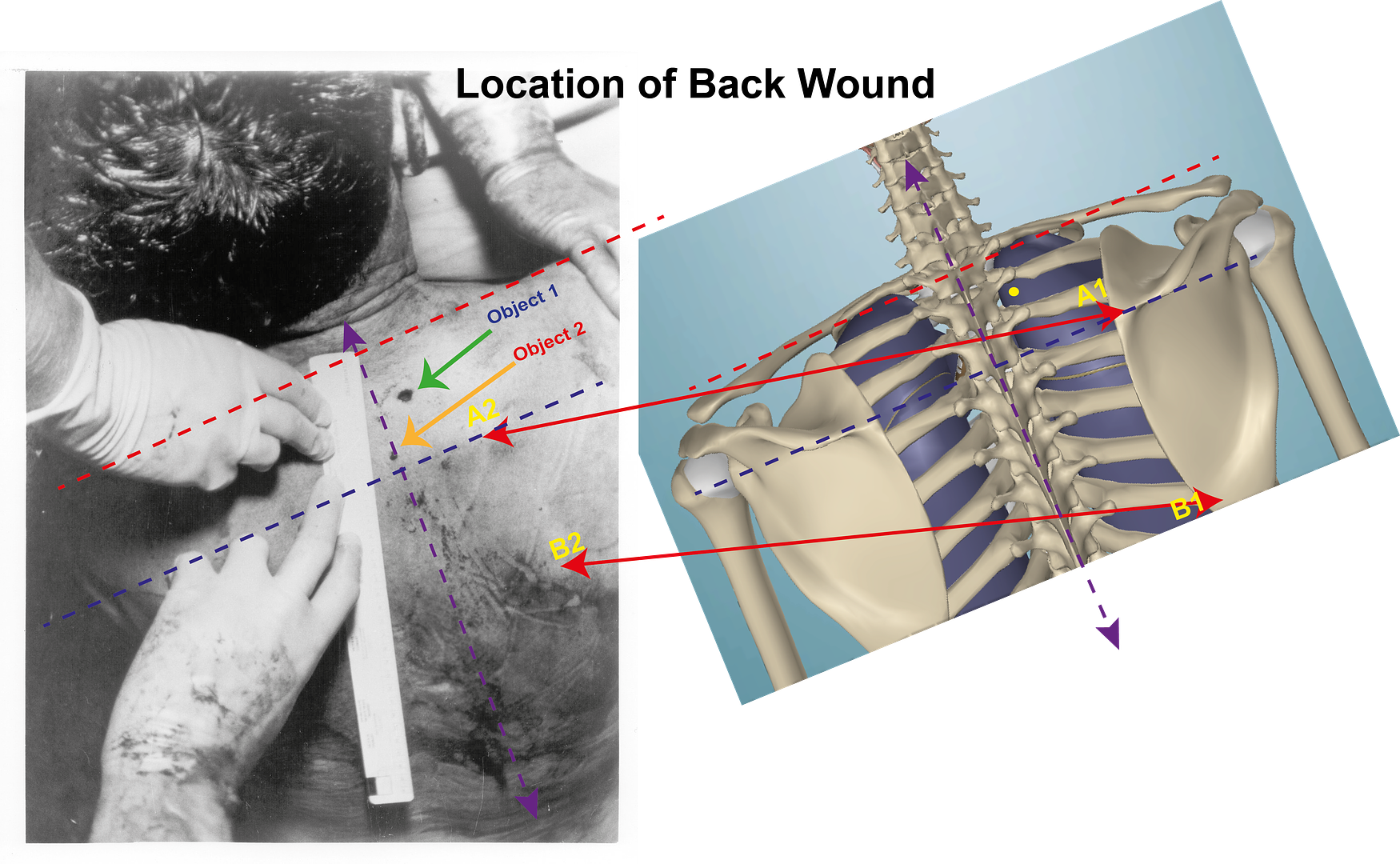
Object 2 is the blood spot.
On the back of JFK you will see two labels in yellow A1 + B1. Between these two labels and below the B1 label you will see an outline shape underneath the skin. The shape that is being seen is the outline of part of JFK’s right Scapula.
If you look at the anatomical model that is to the right of the image you will see the complete Scapula on the skeleton. The two labels A1 + B1 in cyan on the skeleton point to these same parts that can be seen through JFK’s body that are labelled A1 + B1 in yellow.
The A1 point is at the Medial edge of the Scapular spine. The Scapula spine is that ridge crossing the Scapula and the Medial edge is the edge of the Scapula nearest the vertebral column.
In order to gain a reference by which to judge the location of the wound, I have drawn a blue line across the model as well as the body from this A1 point. Having done that I now have a base line on the body. This base line is midway between T3 and T4.
If you look at the upper right corner of BE 5, you will see the right hand of Commander Boswell holding JFK’s shoulder. I am assuming that it is Humes doing the measuring. I have tried to guess where Costa IR is on the JFK’s body and have drawn a red line across the body, as well as on the model, signifying where I believe Costa IR is. I accept that, this line signifying the position of Costa IR might be slightly out, but it will not be very far out. This red line now gives me an upper limit beyond which this wound is not located.
What can be said, for certain, is that the wound lies between those two lines. If you look at Boswell’s right hand [ I assume it is Humes that is measuring ] you will see that the nail of his pinkie, just to the right of the label A1, is roughly on the same plane as the wound.
I suspect the position of this wound is above T3 but below T2. One thing is for certain it is nowhere near C7/T1.
Hi James
Well done! I couldn't have explained things any better than that.
I'm finding it a bit difficult to believe how many years we have been looking right at a photo of a bullet hole near the level of T3, and have believed it to be at C7/T1, simply because that is where Humes told us it was. As you say, the spine of the scapula is the only really prominent landmark in that area, and there is no mistaking it in that photo.
-
That's too bad, Chris. I was hoping something unique, though I have no idea what.
I'm not having a lot of luck getting info on the windage adjustment cap. I might try something a little different. I saw a post on a firearms thread from one of the managers of a company that purchased the remaining stock of 4x18 scopes when the Ordnance Optics Inc. went out of business. He left a phone number on this post, and I actually spoke to the man earlier this year. If I can find the number, I'll try again.
-
Hi Dave
That font thing is driving me nuts, too. It seems as soon as I cut and paste a text, the rest of my post adopts whatever font the quote was in. I'm not computer savvy enough to correct it.
Anyways, back to the back wound. I'm a relative newcomer to the JFK assassination research scene, having only really started to do any serious investigation into this matter in the late 90's, and even then it took me several years to get over all the nonsense conspiracy theories, and begin to look at the real evidence.
One thing I have noticed, and I am probably just as guilty as anyone in this regard, is that we all have our own pet theories about Parkland and Bethesda, and tend to get defensive when anyone challenges that theory.
I tend to somewhat agree with your idea of alteration to the head wound, but I get deeply puzzled when I read Tom Robinson describing a gaping rear head wound, and a 1/4 inch round hole in the hair just behind the right temple, right where the autopsy report says there was a large wound. This is true of so much of the information in this case. Just when you think you have nailed down something as being valid, another piece of information invalidates the first piece of information. And what is with Tom Robinson, anyways? Had he never, in all his career, seen a gunshot wound from a rifle before? He actually let the ballistics "expert" (FBI?) at the autopsy tell him the gaping rear wound was an entrance wound (caved in from the impact or some such nonsense) and the neat little round 1/4 inch hole up near his forehead was from a piece of shrapnel exiting his head. Were people in 1963 really that much in awe of anyone in authority?
But, I digress...
From reading what you have written, I have deduced three things.
1. You believe serious alterations were done to the head wound between Dallas and Bethesda.
2. You believe the throat wound was the result of a shot from the front.
3. You believe there was no back wound, neither a genuine one inflicted by an assassin's bullet in Dallas, nor one inflicted as part of a cover up between Dallas and Bethesda.
Nos. 1 & 3 require the autopsy doctors to do some serious lying, especially since the altered head wound magically managed to hide the original right posterior cranial wound reported by so many witnesses, including the surgeons at Parkland. You seem to accept that they lied their butts off about these major wound points, but accept as Gospel that the Bethesda doctors saw incisions made to insert chest tubes, but no chest tubes were actually inserted. I don't follow you. If they lied about so many things, why not lie about the chest tubes?
For starters, chest tubes would not have been left in JFK's chest at Parkland. I know this from personal experience, as I am a part time paramedic on our ambulance here, and have been attending on a number of cardiac arrest calls. Once at the hospital with these patients, many devices, ranging from intraosseous infusion devices to intubation devices to chest tubes, are applied in an effort to resuscitate a patient in cardiac arrest. My partner and I inevitably will be there, too, when resuscitation efforts are abandoned, and are often asked by ER staff to assist in getting the patient into a body bag, prior to taking the patient to the morgue. Every single case I have been on, great care is taken by ER staff to remove all of these devices prior to bagging.
The chest tube is actually nothing more than a large bore needle, varying in size depending on the purpose it is being inserted for. In cases where the patient is unconscious or pulseless, the surgical incision step is often omitted, and the needle inserted directly through the epidermis. While my ticket does not allow me to insert a chest tube, for the purpose of relieving a tension pneumothorax, I have seen an emergency chest tube inserted into a conscious patient's pleural cavity in the field, and no scalpel incision was ever made. The patient never complained, either, as he was too busy trying to draw in enough oxygen to make up for what he had not been getting prior to insertion of the chest tube.
As the chest tubes are not that big, and removal of the chest tube would cause the intercostal tissue to close up after it was removed, only someone within a couple of feet of JFK's corpse during the autopsy, and actually looking directly into the incisions, would actually be able to tell whether or not chest tubes had ever been inserted at all. Humes had a perfect opportunity to lie about the chest tubes.
Why lie about the chest tubes? Simple. If JFK was shot at the level of T3 with a FMJ bullet, especially a great penetrator like the 162 grain 6.5mm FMJ bullet, there would have been an exit wound on the front of JFK's chest. No doubt about this in my mind whatsoever. In fact, at that short range, that same FMJ bullet would have had enough energy left to go through the jump seat and Connally, and possibly have made it through the front seat and into Kellerman. Instead, it vanished. It was easier to tell the bubbas in the cheap seats that the bullet only penetrated an inch or so, than to tell everyone that some exotic fragmenting (hell, disintegrating) bullet, likely of CIA origin, had come apart and turned to powder after penetrating JFK's lung for a couple of inches. Know why this was so dangerous? That is simple, too. If you give information like this to the unwashed masses, how long is it before they start to look at the massive head wound, and start to wonder how an FMJ bullet could have had such an explosive effect? Remember, many of these men would have been WWII or Korean War vets that had likely seen many people shot in the head with FMJ bullets.
Finally, I cannot overemphasize the importance of the trachea being deviated to the left, as Perry observed during the tracheostomy procedure. Remember, it was deviated to the point Perry was obligated to sever the left strap muscle, just to gain clear access to the trachea. I have spoken to many ER doctors about this, and they are unanimous in their belief that the only thing that could cause deviation of JFK's trachea to the left would be a tension pneumothorax in the right lung.
And, if a tension pneumothorax was not caused by a bullet wound in JFK's back, what do you think caused it?
-
"I suffer from C7/T1 Derangement Syndrome, I must confess.
It's the most mild of JFK-related maladies, imho..."
Hey, that's okay, buddy, love ya anyways!

-
I had planned to write more about the scope but, I'm beginning to doubt if one of the things I stated about the way Klein's mounted the scope is true or not. Once again, the scope:

As you all may or may not know, rifle scopes inevitably have the elevation adjustment cap on the top, and the windage adjustment cap on the right side of the scope, as viewed from the rear. On C2766, and presumably all the other Carcanos that Klein's mounted scopes on, the windage cap is on the left, opposite of what is normal. I was told, by what I considered a reliable source, that Klein's had elected to do this for the same reason the scope is offset to the left; that being it would not be possible to load the en bloc clip into the magazine with the scope or the windage cap above the magazine.
Looking at the above photo, I am now beginning to wonder if the Ordnance Optics 4x18 scope was not manufactured with the windage cap on the left, and if it might have been specifically selected by Klein's to mount on Carcanos because of this unique feature. If the scope in the photo was turned 90° to the right, the printing would almost be upside down. Wouldn't a manufacturer want his name to appear in a legible fashion?
I currently have feelers out on a number of forums to see if I can find someone who owns one of these scopes. Answering my question should be as easy as removing the caps and seeing which one says "<UP-DOWN>" and which one says "<LEFT-RIGHT>".
-
The photo below has been shown on JFK assassination thousands of times, and it is widely accepted that the upper "spot" is an entry wound, presumably made by a bullet, at about the level where cervical vertebra C7 comes into contact with thoracic vertebra T1.

Now, outside of the fact the autopsy results from Bethesda told us this wound was at the level of C7/T1, how could we actually prove this was the level the bullet entered the back at, simply by looking at this photo?
You can't.
The properly prepared medical evidence -- Burkley's death certificate, the autopsy face sheet filled out in pencil -- as well as the holes in the clothes and the overwhelming witness testimony put the wound at T3.
JFK was shot in the back at T3.
Period.
The bullet holes in the clothes are definitive landmarks for the T3 back wound.
Improperly prepared autopsy photos with no chain of possession do not count as evidence.
Hi Cliff
I, too, believe the entry wound was at T3. However, I believe this photo actually is showing us an entry wound at T3, and we have just believed it was showing us an entry wound at C7/T1 because that is what the autopsy results told us.
Bob, I must respectfully and fundamentally disagree.
There are two kinds of autopsy evidence -- that which was properly prepared, and that which was not.
The C7/T1 wound rationale was based on measurements which violated 3 different autopsy protocols.
They used a movable landmark, the mastoid process, instead of a fixed landmark; they used a cranial landmark for a thoracic wound; the measurements were recorded in pen, not in pencil as per proper autopsy protocol.
The BOH autopsy photo violates numerous protocols -- there's no evidence it's Jack Kennedy in that photo; the use of the ruler is anti-scientific, and there is no chain of possession for any of the extant autopsy photos.
There are anatomical landmarks that are faintly visible in this photo that will back up what I am putting forward here.
You can polish this turd all you want but it's still a turd.
And a fake debate.
That JFK was shot in the back at T3 should be the subtext for ANY discussion of the murder of JFK.
Cliff
Can you not comprehend when someone is agreeing with you?
-
The photo below has been shown on JFK assassination thousands of times, and it is widely accepted that the upper "spot" is an entry wound, presumably made by a bullet, at about the level where cervical vertebra C7 comes into contact with thoracic vertebra T1.
Now, outside of the fact the autopsy results from Bethesda told us this wound was at the level of C7/T1, how could we actually prove this was the level the bullet entered the back at, simply by looking at this photo?
You can't.
The properly prepared medical evidence -- Burkley's death certificate, the autopsy face sheet filled out in pencil -- as well as the holes in the clothes and the overwhelming witness testimony put the wound at T3.
JFK was shot in the back at T3.
Period.
The bullet holes in the clothes are definitive landmarks for the T3 back wound.
Improperly prepared autopsy photos with no chain of possession do not count as evidence.
Hi Cliff
I, too, believe the entry wound was at T3. However, I believe this photo actually is showing us an entry wound at T3, and we have just believed it was showing us an entry wound at C7/T1 because that is what the autopsy results told us.
There are anatomical landmarks that are faintly visible in this photo that will back up what I am putting forward here.
-
The photo below has been shown on JFK assassination forums thousands of times, and it is widely accepted that the upper "spot" is an entry wound, presumably made by a bullet, at about the level where cervical vertebra C7 comes into contact with thoracic vertebra T1.
Now, outside of the fact the autopsy results from Bethesda told us this wound was at the level of C7/T1, how could we actually prove this was the level the bullet entered the back at, simply by looking at this photo?
-
ain't buying it. more like a "miss"-deal than a winning hand.
the sleeves
duplicate
I've been saying for a long time now that I think the person's sleeves are rolled down (notice the cuff line near the wrist), but have more sunlight reflecting off them than other parts of his / her body, thereby creating a large area of light-colored "spectral highlights" which many people have mistaken for that person's having a bare forearm.
Let me add that FWIW, I still think that the person in question is probably Oswald.
But PM's "buttons" are intriguing. And the cuff of the "shirt" is up the forearm a bit, not unlike like the woman's coat / dress.
BTW, as many of you already know, a fairly recent post (on another thread?) said something about the WC's knowing that there was an unidentified person on the steps who was taking photographs during the motorcade. Prayer Man / Prayer Woman does seem to be lowering both arms / hands from his / her face area about the time that the shots started ringing out, as though he or she was holding a non-TLR type camera (or binoculars) from his / her eyes...
--Tommy

Edit: Duncan's blond-haired lady in the black dress was also captured in the Cook-Cooper film.
(It is generally believed that the arrow is pointing to Vicki Adams.)

Yes, here she is in motion, carrying the bag(s)

WHAT OUTSTANDING EVIDENCE!!! I NOMINATE DUNCAN CINQUE FOR "RESEARCHER OF THE YEAR"!!!!
LOLOLOLOLOL!!!!
-
I think David Lifton was saying he believed the lower back wound was the original and true back wound, and that the upper back wound, which was actually at the level of the collar (5.75" higher), was created to allow a connection with the throat wound. In the autopsy photo, the ruler is likely covering the lower back wound.
...later that evening, and by the time of autopsy photography of that area occurred--i.e., by the time a permanent photographic record was
being made--there existed (i.e., "was created" --again, my quotes) a higher (and equally false) wound.
Bob & Sandy,
I believe Mr. Lifton is stating that both "wounds", high and low, are "false". See above quote; "a higher (and equally false) wound".
Hi Tom
I see what you mean. I mistakenly assumed Mr. Lifton had stated the lower wound was genuine, but didn't match up with the throat wound, and had to be "moved" up to JFK's collar line.
I'm afraid this is where I have to disagree with him. There is simply too much medical evidence from Parkland Hospital that points toward an injury to the right lung causing a tension pneumothorax in that lung, and an entrance wound at the level of the T3 vertebra (5.75" below the collar) is a perfect match for such an injury.
The Parkland Hospital evidence of an injury to the right lung is. . . is what? Are you referring to Perry's request for a chest tube? Also, I have a serious problem with the argument that the circumstantial evidence of a pneumothorax is a "perfect match" for a T-3 rear injury; when:
(a) no one saw any such T-3 injury at Parkland Hospital, in the reports and testimony written at the time
(b ) Admiral Burkley (at Bethesda) referred to the T-3 wound as a wound that "occurred" in the back. As I posted elsewhere on this thread: just consider the implication of the verb "occurred". (To appreciate the absurdity of it: can you imagine any Bethesda doctor--even Humes--stating that a wound "occurred" in Kennedy's head? Just imagine the response if AP or UPI reported Kennedy's fatal head injury that way!).
I'll take it one step further: Can you imagine a police report, about a homicide in any city, being written that way? That the deceased died of a fatal gunshot wound which "occurred" in his head?
(Perhaps its the lateness of the hour here in West Los Angeles, but I can just imagine the dialogue in a police station where such language is used to report a homicide. Really: it belongs on Saturday Night Live. And if Admiral Burkley were still around, perhaps he could play the reporting police officer!)
To recap: I think there is a serious logical problem of attempting to take the T-3 wound--which (in Burkley's report) "occurred" (a wound which no one reports at Parkland Hospital in the contemporary records), and that includes people who washed the body --and then combining that with the inference that, because a chest tube was called for, that justifies a connection between the internal chest injury and an impact at T-3.
The undeniable fact is that the putative rear entry wound was not reported (that weekend) by any Parkland observor.
The language used to describe the wound at Bethesda (that it "occurred") is fishy.
The tension pneumothorax to which you are alluding was apparently not so serious (or obvious) that the chest tube --which was called for--was not pushed all the way in. In fact, according to the autopsy report, it didn't go further in than the epidermis.
So, given the above factors, I do not agree with the notion that one can (or should) "connect the dots" as you do; or that such a nexus constitutes a "perfect match."
Since its clear to me (at least) that JFK's body was intercepted and altered between Dallas and Bethesda, I think it is poor methodology to attempt to combine anything from Bethesda (i.e., post alteration) with data from Parkland (pre-alteration) to draw a reliable inference as to what was going on inside JFK's body.
Anyway, that's where I stand on this issue.
Always willing to change my mind, if there is evidence; but I call your attention again to what I wrote about what happened on the night of December 11, 1963, when reporter Bill Burrus received a call from "higher authority" (my quotes) to lay the groundwork for his story (the next day) that (based on his "authoritative"source) JFK was hit in the back--something not a single medical observer at Parkland Hospital reported on 11/22/63.
Beware. This road is filled with logical and linguistic and anatomical potholes.
DSL
10/26/15 - 5:40 AM PDT
Los Angeles, California
Malcolm Perry made an observation while performing the tracheostomy on JFK. He observed JFK's trachea to be deviated to the left, so much so that it was necessary for him to sever the left strap (sternohyoid) muscle that lies just outside the trachea, in order to successfully complete the tracheostomy.


Deviation of the trachea to one side or the other is one of the signs of a tension pneumothorax. As air pressure builds in either the right or left pleural cavity, it exerts a strong force on the unaffected side of the chest, displacing everything in the unaffected side.
Just as you do not believe many of the findings from the Bethesda autopsy, I do not believe the chest tube(s) procedure only got as far as shallow incisions in the epidermis of JFK's chest. If you have ever watched the insertion of a chest tube, you will know that, once the tiny incision is made in the intercostal space between the ribs, insertion of a chest tube takes only a few more seconds, and connection of that tube to drainage not much longer than that.
From the Healthline website:
http://www.healthline.com/health/chest-tube-insertion#Procedure4
What Happens During Chest Tube Insertion?
A surgeon or a pulmonary or critical care specialist usually performs a chest tube insertion.
- Your doctor will prep a large area on the side of your chest, from your armpit down to your abdomen and across to your nipple. This will involve sterilizing the area using Betadine and potentially shaving any hair from the site, if necessary.
- An intravenous (IV) and/or local anesthetic may be used to make you more comfortable during the chest tube insertion, which can be painful.
- Using a scalpel, he or she will then make a small (¼ inch to 1½ inch) incision between the ribs near the upper part of your chest (the specific location will depend on the reason for the chest tube).
- Your doctor will gently open a space into your chest cavity using a finger and clamps, and guide in the chest tube. (Chest tubes come in various sizes for different conditions.)
- A small suture keeps the tube in place, and a sterile bandage is applied. The tube is then attached to a special one-way drainage system that only allows air or fluid to flow out. This prevents drainage back into the lung.
While the chest tube is in, a doctor or nurse will continually monitor your breathing, pain, and chest tube status.
Why would the surgeons go so far as to make the shallow incision(s) in JFK's chest, and not take a few more seconds to insert the chest tubes?
-
However, for the above reasons, it was necessary for the gunsmith at Klein's to make a further modification to the scope.
Bob,
At the moment I can't find the source of the quote, but according to the Klein's gunsmith, they did NOT mount scopes on the Carcano model allegedly sent to LHO. Only on the longer type. IIRC, this was discovered when Kleins asked the FBI "how" they wanted the scopes mounted on the rifles the FBI ordered for test purposes.
Tom
Hi Tom
Actually, it was the shorter carbine (17 inch barrel) that Klein's was mounting the scopes on, as opposed to the 21 inch barreled short rifle found on the 6th floor.
I find it very odd that Klein's would ask the FBI how they wanted the scopes mounted on the test rifles they ordered, as all Carcanos, be they a short rifle, long rifle or carbine, have the identical receiver and chamber on them. Once you know how to mount a scope on a carbine, the procedure should be identical on the other rifles, and I cannot see any other way to mount a scope on a Carcano than the way they did.
-
Hi Chris
The mounts supplied by Klein's were also used to mount scopes on a model of Mauser. For the Mauser, it was necessary to grind away a portion of the rear of the four-hole mount, leaving three holes on the base.
From what I can gather, it seems they had an excess of three hole mounts for the Mauser, and simply used them as is to mount scopes on Carcanos.
P.S.
I'd be interested to know what you were able to glean in the way of instructions from the photo I posted.
P.P.S.
I think it entirely possible Klein's might have mounted this scope.
-
Thanks, Pat, although I am still unable to make out any numbers on the enlargement. However, if it is a 15 inch ruler, at 1 inch = 2.54 cm. the ruler would be about 38 cm. long.
I think we have been looking at the back photo quite wrongly all these years, and forgetting that perspective does tend to foreshorten things. Also, we believe we are looking at an entrance wound at the level of vertebrae C7/T1 mostly because that is where the WC told us the wound is,
However, the scapular spine landmark tells us a different story, as this landmark is at about the level of vertebrae T4/T5. The entrance wound is, at most (and possibly less) two of Boswell's finger widths above this landmark. Unless Boswell had REALLY big fingers, this would, to me, place the entrance wound at T3 in this photo.
-
From the HSCA testimony of Lt. Lipsey:
"... They traced it through the back of his neck through, you know, when they did the autopsy, through the inside of his body and there was no where the bullet was then where it should have exited, it was not. And at the angle it was traveling, and from, you know, with the other things they saw visible in the chest area once they cut him open, you know, it had started down, but where was it?
Because, from their conversations, they tracked this bullet as far as they could in a downward position before they couldn't tell where it went. That's when they started taking organs apart and looking where ever they could look without going ahead and just cutting him apart. And I think their decision finally was, we're just, you know, not going to completely dissect him to find this bullet. So they tracked the bullet down as far as it went. Obviously, by that point it wasn't that important.
... The bullet has penetrated. It went into his skin. There was evidence of it inside his body. It had penetrated the body. There was no way it could have fallen out."
BINGO!!
I had a feeling you'd like that.
-
BUT... why did Gerald Ford have to raise the back wound by 2 inches?? Humes (via the autopsy) had already done so (in step #2 above).
The WC staff believed the back wound was below the throat wound until March 1964, when Chief Justice Warren demanded his staff bring him better witnesses, and Joe Ball--who was tasked with explaining how a shot fired from above could enter the back and exit the throat--made a sudden trip to Bethesda hospital and had a long talk with Admiral Galloway, Dr. Humes, and Dr. Boswelll. A few days later, Humes and Boswell testified, only now accompanied by some freshly-made drawings now showing---for the first time ever--a back wound above the throat wound. This is all documented and discussed in my presentation The Single-Bullet Theory, Voodoo Science, and Zombie Lies, which was delivered at the 50th anniversary of the Warren Report conference last fall. This presentation can be viewed here: https://www.youtube.com/watch?v=EHFvDw0VSb0
Thanks for answering my question, Pat.
So Humes raised the back-wound location so that it could be associated with the throat wound. But alas he didn't raise it enough, so the WC had to raise it further.
But why didn't Humes raise it higher to begin with? I suppose because then it wouldn't have jibed at all with what witnesses had seen and were recording about the wound.
Yeah, that makes sense.
Only if you're desperate to claim the autopsy photos are fake. To my way of thinking, the back wound in the photos proves the lie orchestrated by Ball and Specter at Warren's urging. It proves the lie, and disproves the SBT.
Hi Pat
Did you happen to see the post I directed to you, regarding Martin Heinrich's work on the autopsy back photo?
-
How long must we be subjected to the pseudo-science nonsense that Duncan MacRae attempts to pass off as "research"?
Dear moderators, I always believed this to be a serious forum. If you allow Mr. MacRae to turn this place into a circus, you could at least do the polite thing and invite Jim Fetzer and Ralph Cinque back to join Mr. MacRae in his comedy routine.
Dear Moderators,
Robert is just trying to get me banned because I banned him from my Forum for repeatedly posting, and despite generous repeated warnings by me, that I am being paid by the US Government to operate my forum. He's not right in the head, so please ignore his deliberately disruptive uneducated rants.
Thanks
Duncan MacRae
What ever you say, Duncan Cinque.
-
How long must we be subjected to the pseudo-science nonsense that Duncan MacRae attempts to pass off as "research"?
Dear moderators, I always believed this to be a serious forum. If you allow Mr. MacRae to turn this place into a circus, you could at least do the polite thing and invite Jim Fetzer and Ralph Cinque back to join Mr. MacRae in his comedy routine.


 there is only one type of mount, both the 3 hole and 4 hole started out the same. some mounts were ground to fit 95 mausers (in order to clear the bolt stop). the carcano should have had a four hole mount, with no need for grinding...but Kline's had both styles and simply installed the wrong one.
there is only one type of mount, both the 3 hole and 4 hole started out the same. some mounts were ground to fit 95 mausers (in order to clear the bolt stop). the carcano should have had a four hole mount, with no need for grinding...but Kline's had both styles and simply installed the wrong one. 

Landmarking the Back Wound
in JFK Assassination Debate
Posted
I am somewhat late with my findings but, I have also come to the conclusion that manipulation of JFK's head made it possible for us to believe the back wound was higher than it actually was.
There seems to be a great deal of discrepancy between anatomical drawings of the back of the human thorax. While many show the scapular ridge (spine) beginning at about the level of T4/T5 vertebrae, many others show it beginning at the level of T3 vertebra. I will try to find out which is accurate.