

Robert Prudhomme
-
Posts
4,105 -
Joined
-
Last visited
Content Type
Profiles
Forums
Events
Store
Posts posted by Robert Prudhomme
-
-
From the HSCA interview of Lt. Lipsey:
"LIPSEY: The bullet has penetrated. It went into his skin. There was evidence of it inside his body. It had penetrated the body. There was no way it could have fallen out."
If I had a dollar for every time an HSCA interviewer was given an opening such as this, and did not follow it up with the obvious question "What evidence inside the body would that be?", I would be a rich man.
-
From the HSCA testimony of Lt. Lipsey:
"... They traced it through the back of his neck through, you know, when they did the autopsy, through the inside of his body and there was no where the bullet was then where it should have exited, it was not. And at the angle it was traveling, and from, you know, with the other things they saw visible in the chest area once they cut him open, you know, it had started down, but where was it?
Because, from their conversations, they tracked this bullet as far as they could in a downward position before they couldn't tell where it went. That's when they started taking organs apart and looking where ever they could look without going ahead and just cutting him apart. And I think their decision finally was, we're just, you know, not going to completely dissect him to find this bullet. So they tracked the bullet down as far as it went. Obviously, by that point it wasn't that important.
... The bullet has penetrated. It went into his skin. There was evidence of it inside his body. It had penetrated the body. There was no way it could have fallen out."
BINGO!!
Why oh why did no one ask Lt. Lipsey to elaborate on this sentence?
".... the angle it was traveling, and from, you know, with the other things they saw visible in the chest area once they cut him open, you know, it had started down, but where was it?"
WHAT OTHER THINGS DID THEY SEE VISIBLE IN THE CHEST AREA???
-
You ask why the low back wound was a problem on 22/11/63. [And/or why was it a problem for the WC.]
Now, suppose Lifton is right, that the low back wound was faked. What would have been the purpose of faking the wound? If it was to couple it to the throat wound, then why would they have placed the wound so obviously low?
The purpose of the back wound was to create the visual appearance that Kennedy was shot from the rear. IMHO--and as developed in Best Evidence--the shallow wound was to be "matched" to a bullet panted on a Dallas stretcher.
Remember: when the back wound was created, it is very likely that the conspirators did not now the tracheotomy wound was anything more than a trach incision. I think the "trouble" started when it was realized that the throat defect was not just the site of a trach incision, but a bullet wound.
That's when the real problem began: what the heck happened to the bullet that entered at the throat? It had to be located and extracted. Under no circumstances could it be permitted to enter the official "evidence stream" and go to the FBI Lab. I believe it was extracted and that is what accounts for the original FBI "receipt for a misle" (sic). Then some sleight of hand was performed and two tiny fragments from the brain were substituted. The actual missile has disappeared.
Now back to the back wound(s). All of this gets somewhat hypothetical. The bottom line is that the wound was placed "too low" and that led to the creation (at Bethesda, I believe) of a "higher" wound, and the necessity to hide the "lower" one via the adroit placement of the ruler to during autopsy photography. This is one line of speculation. But the bottom line is this: the rule doesn't measure anything, and its location is such that it would conceal the "opening" reported by FBI agents Sibert and O'Neill.
DSL
10/24/15 1:50 A.M PST
Ballistically speaking, what kind of bullet do you think could enter JFK's throat and either a) not exit the back of his neck or
 not totally destroy the vertebrae in line with the path of this bullet?
not totally destroy the vertebrae in line with the path of this bullet? -
To Pat Speer
I read the excerpt below from a post made by you in 2013:
"4. Shortly after I used the ruler to measure the wound, I was contacted by, if I'm not mistaken, Martin Hinrichs,. He'd cleaned up the back wound photo considerably, and was able to demonstrate to my satisfaction that the ruler in the photo was not 12 inches, but a centimeter ruler closer to 15 inches, if I recall. So Robert's assumption the ruler is 12 inches long--the assumption I'd made as well--is incorrect."
I am intrigued by this. Did Martin clean the photo up to the point the numbers could actually be read on this ruler? The reason I ask is that I believe a known anatomical landmark can actually be seen in this photo:

The outline of the scapula (shoulder blade) is clearly visible in this photo. However, something else is equally visible here, and is referred to medically as the "scapular spine" or "spine of the scapula".

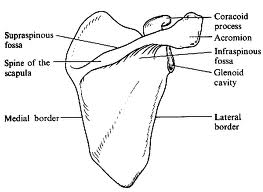
As seen in this diagram, the thoracic vertebrae are the ones with ribs attached to them, with T1 being the uppermost thoracic vertebra. Counting down, we can see the innermost end of the scapular spine is at a level about midway between T4 and T5.
Looking again at the photo, I believe the same innermost end of the scapular spine is visible at about the same level as the smaller dark spot some think may be another wound. It is also on the same level as the space between the fingers of the top hand and the fingers of the bottom hand. Now looking at the entrance wound, how far is it from the scapular spine to the entrance wound? I would say not more than the width of Boswell's two fingers. If we could read the ruler, we would know precisely.
-
I'm afraid this is where I have to disagree with him. There is simply too much medical evidence from Parkland Hospital that points toward an injury to the right lung causing a tension pneumothorax in that lung, and an entrance wound at the level of the T3 vertebra (5.75" below the collar) is a perfect match for such an injury.
Any chance the throat wound could have caused the pneumothorax? BTW, although Humes insists photographs were taken of the 5 cm bruise at the apex of the eviscerated right pleural cavity (above the apical portion of the removed lung), per Horne that photo is not in the autopsy collection at NARA. I wonder why someone would remove THAT photo???
BTW, the x-ray section of "Inside the ARRB" is ALL about the skull x-rays. Nothing to add to what I wrote earlier regarding the chest x-ray.
And as I mentioned earlier, my suspicions regarding the x-rays were correct. Kennedy Family permission is required to view them.
The autopsy descriptive sheet is included in "Inside the ARRB", and along with the blank space for brain weight, it includes the following:
Right Lung: 320 grams
Left Lung: 290 grams
Obviously the right lung is peppered with 30 grams of bullet fragments!

Tom
Hi Tom
The right lung is actually larger than the left lung, as the heart is slightly offset to the left and displaces some of the volume the left lung would occupy.
I do not believe it would have been possible for the throat wound to have caused a tension pneumothorax in JFK's right lung. While there was an opening in JFK's trachea, this wound also extended through the skin of his throat. This would tend to vent any accumulated air pressure to the atmosphere. It would be different if the trachea were fractured, say from a sharp blow to the neck, and air escaping the trachea had nowhere to go.if it did cause a pneumothorax, there would have been one in the left lung, as well, and Dr. Perry would not have seen JF's trachea deviated to the left, as he performed the tracheostomy.
Also,
-
I think David Lifton was saying he believed the lower back wound was the original and true back wound, and that the upper back wound, which was actually at the level of the collar (5.75" higher), was created to allow a connection with the throat wound. In the autopsy photo, the ruler is likely covering the lower back wound.
...later that evening, and by the time of autopsy photography of that area occurred--i.e., by the time a permanent photographic record was
being made--there existed (i.e., "was created" --again, my quotes) a higher (and equally false) wound.
Bob & Sandy,
I believe Mr. Lifton is stating that both "wounds", high and low, are "false". See above quote; "a higher (and equally false) wound".
Hi Tom
I see what you mean. I mistakenly assumed Mr. Lifton had stated the lower wound was genuine, but didn't match up with the throat wound, and had to be "moved" up to JFK's collar line.
I'm afraid this is where I have to disagree with him. There is simply too much medical evidence from Parkland Hospital that points toward an injury to the right lung causing a tension pneumothorax in that lung, and an entrance wound at the level of the T3 vertebra (5.75" below the collar) is a perfect match for such an injury.
-
You ask why the low back wound was a problem on 22/11/63. [And/or why was it a problem for the WC.]
Now, suppose Lifton is right, that the low back wound was faked. What would have been the purpose of faking the wound? If it was to couple it to the throat wound, then why would they have placed the wound so obviously low?
I think David Lifton was saying he believed the lower back wound was the original and true back wound, and that the upper back wound, which was actually at the level of the collar (5.75" higher), was created to allow a connection with the throat wound. In the autopsy photo, the ruler is likely covering the lower back wound.
-
Did any of the other x-rays have these "dirt artifacts" on them, BTW?
Funniest thing...there's no mention of dirt on ANY of the other 14 x-rays... AND enlisted tech Edward Reed explained that the film was removed from all the cassettes, and they were cleaned every Thursday.
I'm only about 1/2 through the x-ray section from Volume II of the ARRB report, so I can't say for certain.
I haven't been able to find the x-rays yet. I'm not finished with the section in the ARRB 5 Volume set devoted to the x-rays, so they MAY be located someone in these 5 volumes, but I do NOT recall seeing them during a previous reading.I had seen references made to the "dirty" chest x-ray but, until you pointed out the possible connection between the "dirt" and the powdered metal that would be left in the lung, following the disintegration of a frangible bullet, I had never put the two together. Wow!
How does one access the x-rays, especially Nos. 9 & 7?
It would be nice if it is this easy, but I'm not convinced yet by any means. I certainly intend to keep looking though...I sincerely hope that everyone reading this thread understands the importance of what you have pointed out here. You may have answered the favourite LN question, "What happened to the bullet, then, if it did not go through JFK and hit Connally?"
Tom
Hi Tom
Yes, we are far from producing conclusive evidence of a frangible bullet coming apart in the top of JFK's right lung. However, at least in my mind anyways, the other possibilities for the "shallow" back wound are systematically being eliminated, with the frangible bullet scenario slowly emerging as the only viable possibility.
As I said in another post, every lie has an element of truth in it. Bruising was reported in the top of JFK's right lung. What if this "bruising" was actually more than just bruising?
Another thing to consider; Would Humes recognize the damage to the lung, inflicted by a frangible bullet, as damage inflicted by a bullet? I certainly hope you are successful in locating the JFK autopsy x-rays.
-
As it turns out, it looks like Doug Horne misspoke when he said that James Jenkins could see Hume's little finger push on the pleural membrane. Here is what Jenkins said in an early interview (his first, I think) with David Lifton. From Best Evidence:
[Jenkins] remembered very clearly Humes’ probing the back wound with his little finger. “What sticks out in my mind,” Jenkins told me, “is the fact that Commander Humes put his little finger in it, and, you know, said that.... he could probe the bottom of it with his finger, which would mean to me [it was] very shallow. .... I remember looking inside the chest cavity and I could see the probe.... through the pleura [the lining of the chest cavity]. .... You could actually see where it [the probe] was making an indentation.... where it was pushing the skin up. .... There was no entry into the chest cavity.... no way that could have exited in the front because it was then low in the chest cavity.
This resolves (to my satisfaction) a number of problematic things. First, it means that there is no reason to believe that Humes probed deeply with his finger, and so the question of how his finger could possibly fit becomes a non-issue. Second, if the official size of the wound (4 mm by 7 mm) is correct or near that, Humes could not have probed very deeply at all, and yet was able to hit bottom. Which means the wound was very shallow indeed. This could be a important clue as to what exactly made the wound. Third, apparently Humes did indeed probe the pleural membrane with a probe, just as he (and at least one other autopsy physician) had testified. This gives me more confidence in Jenkins as a witness.
Sandy:
This is a very interesting (and important) thread.
As you probably know from reading Best Evidence, I believe the back wound to be false (i.e., man made; but certainly not by shooting a gun at the corpse of JFK).
But in this post (that I am now writing), let me focus on just one point: the question of Humes "probing" the back wound with his finger.
If you look at the Clark Panel Report (1968, released in Jan 1969), you will see that they write that it was obvious (based on their examination of the autopsy photos) that the rear entry (let's call it "the back wound" for the sake of this post) could not permit the "insertion" of a finger.
Yet we know that credible witnesses saw Humes insert (at least part of the way) his finger. They did not imagine that; they witnessed it.
So. . . : How to explain that situation? i.e., that "contradiction"
What I believe to be the answer:
I call your attention to the autopsy photographs--which I obtained in December 1982 and published (for the first time) in the Carroll and Graf edition of Best Evidence (1988). You will note the existence of a ruler (which doesn't measure anything) and which covers the location where the back wound (as reported by FBI Agents Sibert and O'Neill) was located. This situation of the placement of that ruler is discussed in Chapter 30 of B.E. --under the breaker "The Puzzle of the Ruler." ( Its my belief that the "back wound" (which the two agents are referring to) is concealed by that ruler.
I also call your attention to the fact that in their FBI report, the two FBI agents refer to that "lower" back wound (my quotes on the word "lower") as an "opening" in the back.
So here's the bottom line: there was (I believe) a "lower" back wound, which was indeed probed by Humes with his finger. That "lower" wound was indeed on the body.
I do not know how deeply Humes finger went in; and that's not the point. My point is that later that evening, and by the time of autopsy photography of that area occurred--i.e., by the time a permanent photographic record was being made--there existed (i.e., "was created" --again, my quotes) a higher (and equally false) wound. A ruler was used to conceal the lower wound--i.e., to conceal it from posterity.
The result: there are witnesses (e.g., the two FBI agents) who actually saw Humes probe the "lower" wound; but the wound that is present in the autopsy photographs (which show the ruler) show a "higher" wound, and that higher wound is definitely too small "to permit the insertion of a finger" (just as reported by the Clark Panel).
Humes - - How Complicit?
If true, does this mean that Humes was directly involved in autopsy chicanery? (Yes, unfortunately it does). I write "unfortunately" because when I wrote Best Evidence, back in the mid-to-late 1970's, I had a more innocent view of Humes. But I'll be writing more about that in Final Charade.
But now back to another (and very important) point: Is there anyway to definitively prove this? Yes, but its never going to happen--at least not in my lifetime. But I predict that if an exhumation is ever conducted, there will be discovered a "wound" or "opening" beneath the ruler.
All of this goes to the larger question of whether the Bethesda autopsy was a fraud.
Was it a fraud? (Or a "perfect medical forgery", which fooled the autopsy doctors?).
My answer to that has changed, over time.
So let me repeat the question: was it a fraud?
My answer (today): yes, it was.
Let's restate this somewhat: Was Humes merely confused, or a "useful idiot" in following some higher authorities "orders" in a scheme to re-arrange (or fabricate) certain medical facts? My answer (today): Yes, I believe Humes was complicit ( but I did not believe that when I wrote Best Evidence).
AN IMPORTANT QUALIFIER: Humes did not do the "surgery of the head area"
However--and this is an important qualifier--I do NOT believe that Humes was responsible for the enlargement of the head wound. In other words, I do not believe that Humes was responsible for creating what he himself described as "surgery of the head area, namely in the top of the skull." That FBI statement was based on what the FBI agents heard Humes say aloud (See Chapter 12 of B.E., for a detailed discussion of this point). (Nor do I believe that the Boswell diagram showing that huge hole, along with the measurements --10 x 17--is a "con job". This is where I diverge (completely) from Doug Horne's beliefs. He believes that Humes did the surgery and then Boswell acted to conceal Humes complicity by creating a bogus diagram. I don't believe any of that.
Instead. . .
I believe the account of Paul O'Connor --as told to the HSCA--that the body arrived with an empty cranium and a huge hole in the head. (FYI: O'Connor not only told that to the HSCA in August 1977; he told it to the Florida newspapers, at around that time.) So O'Connor is "on the record" with regard to all of this in four locations:
1. 1977: The Florida newspapers
2. Aug 1977, the HSCA (Purdy's report)
3. Aug 1979, my original telephone interview (as set forth verbatim in Chapter 26 of B.E.)
4. October 1980: My original filmed interview (as set forth in the Best Evidence Research Video. Now available on the Internet).
And there are three more instances of Paul O'Connor going through all of this:
5. October 1988 - filmed interview with KRON-TV (Stanhope Gould and Sylvia Chase, arranged by me)
6.. Spring 1989 - my very lengthy and detailed follow-up filmed interview with O'Connor at his home (not yet released)
7.. 1990 - Still another lengthy interview --conducted by me--with O'Connor when he was flown to California for the show HARDCOPY
STILL ANOTHER IMPORTANT WITNESS: "Wayne". . .
For those interested in this point (re the empty cranium), I have a witness (who you'll be reading about in Final Charade) who was close with FBI Agent O'Neill; a businessman who was a strong supporter of my work, and who lived in his area, and was a financial supporter. Before O'Neill--who was rather thick-headed and totally pro-Hoover--realized the significance of what he was saying, he repeatedly maintained (this is back in 1992) to this businessman, whose first name was Wayne: "Wayne, there was not brain." He said this repeatedly, and with great emphasis on the word "was". I provided Gunn and Horne with this information. It was never properly followed up.
Bottom line: O'Neill (before he modified his story) corroborated O'Connor: the body did indeed arrive with "an empty cranium."
If that is so, of course that makes Humes (and Boswell) complicit in autopsy fraud. And so their shenanigans with a ruler, during the autopsy photography, pale in comparison with their failure to tell the truth about the condition of the body, when it arrived.
As you all may know, I spoke with Humes twice in November 1966; this is all laid out in Best Evidence in Chapter 8 (and repeated in Chapter 18). As Humes burst out at me, when I confronted him with the Sibert and O'Neill report, he said: "I'd like to know by whom it was done, and when, and where."
This tape was played aloud at the mid-West Convention in 1993. I am going to make it available on the internet, soon.
Humes knew the body was altered. Almost certainly, he was given the "World War III" cover story, and so he ended up participating in this fraud.
What he said about the body in front of the FBI agents (that it was "apparent" that there had been "surgery of the head area, namely, in the top of the skul") is one aspect of this fraud. What he did with the ruler is still another. Humes did not appear before the WC with "clean hands." I thought he did when I wrote B.E.; I no longer believe that. But still, his data --when properly analyzed and interpreted--is invaluable.
DSL
10/23/15 - 5:55 AM PDT
Los Angeles, California
David,
Thanks for dropping in and offering us some valuable insight. I was unaware of the 1968 Clark Panel Report. Yes, that certainly sheds light on the topic. It just didn't make sense that Humes would be trying to probe with his finger a 4 mm 7 mm wound, and yet credible witnesses testified that he did.
My mistake was in assuming that Humes was referring to the lower back wound (what I've considered to be the real wound) when he reported the 4 mm by 7 mm size.
I am aware that that the ruler (not measuring anything) likely was used to cover up the lower wound. There are others posting on this topic -- most perhaps? -- who believe the same. In my opinion it's not just a possibility, it's a fact. (Even so I reserve the right to change my mind.) All the evidence points in the direction.
Now, you say:
My point is that later that evening, and by the time of autopsy photography of that area occurred--i.e., by the time a permanent photographic record was being made--there existed (i.e., "was created" --again, my quotes) a higher (and equally false) wound.
Are you saying that the lower wound is false too? (I know that topic was covered in Best Evidence. But I was primarily focusing on the gaping head wound when I read your book. Plus, I didn't realize at the time that I wasn't reading the latest edition... mine being dated 1980 I believe.) It sound like you're saying that the low wound was fabricated in the pre-autopsy surgery, and the upper wound was fabricated by Humes. Is that right?
Today I've been reading the testimony Lt. Lipsey gave before the HSCA regarding the back wound. According to him, a good portion of the autopsy was spent searching for bullet fragments from the back wound. He says they even cut organs up looking for fragments... but they never found any. That, if true, begs the question, what were they searching for if they knew the wound (the lower one) was fake?
Oh, I think I know... I think you're going say that Humes didn't know the wound was fake. Or if he could see it was, he played along with the charade.
Anyway, reading Lipsey's testimony got me to wondering this: What was the problem, on 11/22/63, with the low back wound?? How exactly did it conflict with the LN narrative at that time?
It wasn't till much later that the WC determined LHO had only enough time to get off three shots, one of which missed. That's what created the conflict with the back wound, right? There were only two bullets for three wounds. Arlen Specter fixed that problem with his magic bullet theory, with Gerald Ford's help when he relocated the wound a few inches higher. But this conflict wasn't known on the day of the autopsy.
As a matter of fact, this is very strange... Humes raised the wound at the autopsy, AND Gerald Ford did the very same (on paper) later for the WC. Did Gerald Ford merely make a change on paper that Humes had already made on flesh? Did Specter's magic bullet theory merely reflect the revised autopsy report? If so, why do these men's actions raise so many eyebrows?
What am I missing here? Can somebody please straighten me out?
Also, why was the low back "wound" fabricated? Surely they couldn't have thought that that, coupled with the throat wound, constituted a reasonable trajectory from the 6th floor of the TSBD.
David, thanks for updating us on your current take on the pre-autopsy surgery. I'm looking forward to reading Final Charade.
Hi Sandy
This has certainly been a morning for revelations, at least for me anyways, and I must say that Mr. Lifton has indeed dropped quite a bombshell here. I have looked at the autopsy photo of the "back wound" many times and have long tried to figure out why the ruler was in the picture, as it did not seem to be measuring anything. Not once did it occur to me it might be concealing the real back wound, and that the wound we are seeing is the fake.
You ask why the low back wound was a problem on 22/11/63. It wasn't a matter of how many shots were fired, at least not at that point in time anyways. The problem was that the assassin's firing position had been "discovered" shortly after the assassination, and that position was behind JFK. It was necessary to establish medically, via the autopsy, that all of JFK's wounds had been inflicted by bullets that originated from behind him.
So, what did the autopsy team have to work with? According to Parkland witnesses, there was a large gaping wound in the right posterior of the cranium that was obviously an exit wound, and a small round wound in the throat that was expanded in the tracheostomy procedure. No one at Parkland knew anything about a back wound, as the surgeons at Parkland never turned him over. I do wonder, though, how the people preparing JFK for his trip to Bethesda could have not seen the back wound.
Luckily for Humes, the back wound did not exit the front of the chest cavity, although it was far too low to have any chance of corresponding to the throat wound. It makes perfect sense that another "entrance wound" would be found up near the collar, and the real wound hidden, just as it makes perfect sense that an exit wound that was originally in the right posterior cranium should migrate up to the area just behind the forehead.
In their haste, though, I believe they under estimated the angle from the 6th floor window to the limo, placing the new back wound still too low to exit through the throat wound, and the entrance wound in the skull (at the EOP) too low to exit near the top of his head. Of course, as we all know, the skull entrance wound was merely moved upward 4 inches a few years later to accommodate this problem.
In short, the head wound and the throat wound were in the wrong places for LHO to have caused them. This was known the night of the autopsy, and had to be dealt with immediately, or the conspiracy would have been exposed.
-
Funniest thing...there's no mention of dirt on ANY of the other 14 x-rays... AND enlisted tech Edward Reed explained that the film was removed from all the cassettes, and they were cleaned every Thursday.Did any of the other x-rays have these "dirt artifacts" on them, BTW?
I'm only about 1/2 through the x-ray section from Volume II of the ARRB report, so I can't say for certain.
Something else that I JUST learned: John Ebersole, a Radiation Therapist, was the ACTING Chief of Radiology on 11-22-1963. For some reason CAPT Brown, Chief of Radiology just happened to be out of town that night. Ain't it A-mazin' how many top officials were unavailable on 11-22-1963, and were replaced by 2nd or 3rd stringers? Why it's ALMOST as if they knew something was going to happen that they wanted no association with...
Hi Tom
I've been sitting here this morning mulling this whole thing over and I have to say, this has stopped me dead in my tracks.
I had seen references made to the "dirty" chest x-ray but, until you pointed out the possible connection between the "dirt" and the powdered metal that would be left in the lung, following the disintegration of a frangible bullet, I had never put the two together. Wow!
The only problem I can possibly see with this is that the jacket of the frangible rifle bullet does not disintegrate to dust, as the core of the bullet does, and pieces of the bullet jacket would show up in the x-ray. However, this is assuming the frangible bullet that caused the back wound actually DID have a jacket. DRT Ammo Inc. makes frangible handgun ammunition that is unjacketed. These disintegrate to powder so perfectly and completely, it is possible to shoot them at the sidewalk between one's feet without concern for a ricochet of any kind injuring one's feet, and yet, these bullets are capable of penetrating skull bone without breaking up.
How does one access the x-rays, especially Nos. 9 & 7?
I sincerely hope that everyone reading this thread understands the importance of what you have pointed out here. You may have answered the favourite LN question, "What happened to the bullet, then, if it did not go through JFK and hit Connally?"
-
Did any of the other x-rays have these "dirt artifacts" on them, BTW?
-
what are your thoughts as to the minimum size of the fragments for a 'typical' 1963 era frangible bullet?
That's EXACTLY what I wanted to hear.Fragments that might possibly show up as "hundreds of dust like particles" in an x-ray of a skull?
X-ray #9, the elusive Chest X-ray taken with heart and lungs still in the body, and X-ray #7 Abdomen and Lower chest also with heart and lungs is described by Dr. Ebersole and the HSCA Panel as having "many dirt artifacts which appear to be metal but are not."
Ain't THAT a surprise?
Tom
Yup, I'm shocked, I tell you, SHOCKED

-
Frangible 6.5mm Carcano cartridge on extreme right, adjacent to 6.5mm Carcano armour piercing round:

Note sand in base of bullet jacket, compressed lead powder above that, and lead/maillechort nose pellet above that. Note also reduced gunpowder charge in cartridge, as compared to armour piercing round beside it. Judging from this photo, the lead powder appears to be fairly coarse, and I wonder if my source was mistaken about the lead powder being compressed, as the material in the middle appears to be quite loose.
-
...there is no reason to assume that a lethal frangible bullet in 1963, when they were still in the developmental stage, would be made from the identical materials
as these ultra-modern frangible bullets.
Thanks for the info, Bob.
I wasn't making that technological leap -- I'm trying to keep things as low-tech as possible. Now that you've opened the door, what are your thoughts as to the minimum size of the fragments for a 'typical' 1963 era frangible bullet? I'm sure CIA people had access to 'better' than typical frangibles, but if low-tech would do the job, why make it more complex?
Tom
Fragments that might possibly show up as "hundreds of dust like particles" in an x-ray of a skull?
-
this is a significant point. bullets do not strike objects and maintain their same trajectory. period. (except for melons placed on ladders by hollywood sleight-of-hand artists).
if the shooter were anywhere on target and the bullet struck the tree branch en route (some say one hit the traffic-signal) then i do not believe for an instant that it would have stayed true enough to hit K. No way.
I agree Glenn, that is significant. And is one reason I've dropped the idea that a bullet hitting JFK's back could have been slowed down enough to make a shallow wound.
There are just too many problems with the idea:
- A sniper probably wouldn't have attempted to make a shot through tree limbs in the first place.
- Hitting a limb would have changed the trajectory. And the bullet would still have more than 25 yards to go, thus multiplying the effect of the new trajectory. Hitting another limb could have corrected the trajectory, but that's a highly unlikely possibility.
- Even if the bullet managed to hit JFK's back, what are the odds that it would make a shallow wound, stop short of the pleura, and THEN disappear?
Okay, on the last point, instead of disappearing the bullet might have fragmented within the flesh, and Humes could have put on an act (part of the "charade" Robert suggested) and made everybody believe there was no bullet to be found. But if that were the case, Humes would have done the same had a frangible bullet lodged itself within the lung. There is no reason to believe the highly unlikely scenario bulleted above when a a much-more likely scenario exists -- the frangible bullet one.
As such, I would revise Tom's list of possible scenarios accordingly. He wrote:
At the moment I [Tom] can only accept two possible scenarios:
1. The pleura and probably the lung were punctured, and Humes et al are lying to protect the LN scenario
2. Some form of an 'exotic bullet' penetrated his back and then broke up to such a degree that it left little or no trace. "Ice bullets", "blood soluble bullets", mercury bullets, etc. have been mentioned. On the one hand I don't see any reason to dismiss them as a possibility, but on the other hand, I don't know if they could inflict the shallow back wound we seem to be dealing with.
To this I would tentatively add a third possibility, in red here:
At the moment I [sandy] can only accept three possible scenarios:
1. The pleura and probably the lung were punctured, and Humes et al are lying to protect the LN scenario
2. Some form of an 'exotic bullet' penetrated his back and then broke up to such a degree that it left little or no trace. "Ice bullets", "blood soluble bullets", mercury bullets, etc. have been mentioned. On the one hand I don't see any reason to dismiss them as a possibility, but on the other hand, I don't know if they could inflict the shallow back wound we seem to be dealing with.
3. A frangible bullet disintegrated and lodged itself within the right lung.
My reasons for making #3 tentative are two-fold. First, I want to know how it is that technicians interviewed by researchers made no mention of the collapsed lung. Second, I'd like to know how the frangible bullet just happened to fragment precisely before entering the lung. Or if it's possible for lung tissue to cause the bullet to break up
Robert, can you comment on this?
Tom, have you ruled out #3?
As I pointed out earlier, a frangible bullet designed for lethal purposes has a hollow point nose that is the key to making this bullet disintegrate back into the metal powder from which it was made. As it travels through flesh (or organ material) the frangible bullet's hollow point nose fills with semi-liquid material. Due to the velocity of the bullet, this semi-liquid matter exerts an enormous hydraulic pressure on the nose of the compressed metal powder bullet core. Within a few inches of penetrating only flesh, this high pressure will cause the bullet to disintegrate into a cloud of metal powder that will literally destroy everything around it for a 2-3 inch radius.
As I stated earlier, the frangible bullet would not have begun disintegration until it had actually entered the lung. This is true of head shots with frangible bullets, in which all that is usually seen on the exterior of the skull is a small neat entrance wound.

Dynamic Research Technologies Inc. .223 calibre frangible bullet fired into block of lye soap from 100 yards. No exit.
bump
-
The clip I posted was the most comparable to a carcano. imo
This was 90 micron powder loaded into a frangible bullet? I expected small buckshot...
Would this powder even appear on an X-ray taken by portable equipment manufactured prior to 1963???
Tom
I would imagine it would, Tom, although there is no reason to assume that a lethal frangible bullet in 1963, when they were still in the developmental stage, would be made from the identical materials as these ultra-modern frangible bullets.
Below are two views of Italian issue M37 "Magistri" 6.5x52mm Carcano frangible bullets, manufacture date likely in the 1930's, although collectors have M37 cartridges with headstamps dated as late as 1953:


Before you all get excited, thinking we've found the bullets that killed JFK, I should explain that this type of frangible bullet was designed as a "safe" bullet for shooting in indoor and urban ranges. One of the properties I neglected to mention about all frangible bullets is that they will also disintegrate to powder when they impact something hard like concrete, steel or rock; meaning there is no danger from ricochet. This feature, plus their incomparable stopping power, is making frangible bullets very attractive to urban law enforcement agencies.
The M37 Magistri frangible range bullet was a very odd bullet indeed. As seen in the top photo, the copper alloy bullet jacket was made in two pieces (soldered together I believe though I am not certain), plus there was often a deep groove at the cannelure, seen just above the mouth of the cartridge in the top photo. This tells me that, on impact and penetration, there was a good possibility the bullet jacket would quickly be in three pieces. Consider the potential of this information when considering all of the WC's evidence regarding bullet jacket material recovered from the head shot.
What is even stranger is the internal construction of this bullet. Just inside the nose of this bullet is a tiny pellet made from lead or "maillechort" (copper/nickel alloy). Behind that, the middle section of the bullet is made from compressed lead powder, the fineness of which I have been unable to determine. Behind that, the base of the bullet jacket was filled with sand.
The M37 frangible bullet weighed only 108 grains (sand being much less dense than lead), compared to the standard Carcano FMJ bullet at 162 grains. To keep the velocity of the M37 bullet the same as the FMJ bullet, the gunpowder charge in the cartridge was reduced.
As can be seen in the lower photo, the nose of this bullet is not complete, and the lead/maillechort pellet can be seen through the small opening. I am not sure of the purpose of this opening but, I am told the pellet served to break up the bigger jacket on impact, and to fracture the bullet's core into dust.
God only knows what effect would be obtained by shooting this bullet into a skull or lung but, I believe drilling a tiny hollow point into the open nose of the M37 Magistri bullet would give us something quite similar to the hollow point frangible bullets seen in Chris' video.
-
Frangible test.
Just curious, Chris. Was that an actual frangible hollow point bullet? The caption below it read HPBT which stands for "hollow point boat tail". I can speak from experience; even the humble hollow point rifle bullet (just by coincidence, the ones I experimented with were also .308 calibre, although the ones I hand loaded were only 110 grain and flat based) will produce dramatic results travelling through a semi-liquid medium.
Edit: Just saw your post with the full length video. Pretty amazing, eh?
-
I still find it somewhat odd that Humes would declare his finger had bottomed out in the back wound, and then still attempt to explore this wound with a probe after the lungs had been removed. If Humes knew anything about human anatomy, which I assume he did, being a doctor, he would know the thickness between the outer back and the pleural lining was not very thick, and a probe could not have gone any further than his finger without entering the pleural cavity. Was he trying to determine if there was a bullet hole in the pleura? A quick look with a flashlight inside the pleural cavity would have determined that.
Are you aware that one witness (at least) later described to a researcher how the autopsy physicians were at one point probing all over the place, trying to figure out the path(s) of the bullet(s)? Unfortunately I don't remember who it was that gave the interview, and I don't remember if they were probing primarily from the throat wound or back wound. But I'm pretty sure the person said they did try to see if there was a path from the back wound to the throat. Or if such a path was possible.
The reason I make a point of this is perhaps it explains why Humes probed through to the pleura. Having probed everywhere else, why not there too?
Upon read the description of this probing, I came away with the impression that it was a far-from-methodical thing. More like frantically looking for an explanation.
If the back wound was at the level of thoracic vertebra T3, as claimed by many witnesses, and Humes knew the basics of human anatomy (one would assume a doctor of his standing would have such knowledge), he would have been aware of the fact the only way to get to the throat wound, from the back wound, was by going through the top of the right lung. As Paul O'Connors' sketch clearly shows, there is only a thin layer of skin, intercostal muscle and ribs between the outside and the pleura.
If Humes did any probing of the back wound, it was all part of a charade.
this is what my question is - why is it assumed that there was a shallow wound? it sounds almost as if people think this is a given, but given the propensity of those involved in the autopsy to be disingenuous, isn't it more possible that it was simply a bullet wound that was disguised as superficial or whatever? this "probe" that's described sounds much more suspect than a low velocity, "puncture wound."
Hi Glenn
I'm not sure you quite understand what I am saying when I say any probing of the back wound was part of a charade.
If the back wound was indeed 1.5-2 inches to the right of the spinal midline, as seems to be the overwhelming consensus of witnesses at Bethesda, any first year medical student (hell, any high school student with an interest in anatomy) would know the bullet could not penetrate much more than an inch through intercostal tissue before entering the pleural cavity and, inevitably, the right lung. In other words, any probe over 2 inches long would be in JFK's right lung. It is quite simple; the entrance wound location described by most witnesses is directly over the top of the right lung.
If this probing was conducted before the lungs were removed, the probe would easily poke through the soft lung in any direction he probed, and tell him absolutely nothing.
If this probing of the back wound took place AFTER the lungs, Humes was either an ignorant fool with no knowledge of human anatomy whatsoever, or deliberately misleading people watching the autopsy. One doctor could have looked inside of the chest cavity while Humes poked a probe into the wound, and seen the probe entering the chest cavity.
Probing for an hour? Do you see now why I call it a charade?
-
this is a significant point. bullets do not strike objects and maintain their same trajectory. period. (except for melons placed on ladders by hollywood sleight-of-hand artists).
if the shooter were anywhere on target and the bullet struck the tree branch en route (some say one hit the traffic-signal) then i do not believe for an instant that it would have stayed true enough to hit K. No way.
I agree Glenn, that is significant. And is one reason I've dropped the idea that a bullet hitting JFK's back could have been slowed down enough to make a shallow wound.
There are just too many problems with the idea:
- A sniper probably wouldn't have attempted to make a shot through tree limbs in the first place.
- Hitting a limb would have changed the trajectory. And the bullet would still have more than 25 yards to go, thus multiplying the effect of the new trajectory. Hitting another limb could have corrected the trajectory, but that's a highly unlikely possibility.
- Even if the bullet managed to hit JFK's back, what are the odds that it would make a shallow wound, stop short of the pleura, and THEN disappear?
Okay, on the last point, instead of disappearing the bullet might have fragmented within the flesh, and Humes could have put on an act (part of the "charade" Robert suggested) and made everybody believe there was no bullet to be found. But if that were the case, Humes would have done the same had a frangible bullet lodged itself within the lung. There is no reason to believe the highly unlikely scenario bulleted above when a a much-more likely scenario exists -- the frangible bullet one.
As such, I would revise Tom's list of possible scenarios accordingly. He wrote:
At the moment I [Tom] can only accept two possible scenarios:
1. The pleura and probably the lung were punctured, and Humes et al are lying to protect the LN scenario
2. Some form of an 'exotic bullet' penetrated his back and then broke up to such a degree that it left little or no trace. "Ice bullets", "blood soluble bullets", mercury bullets, etc. have been mentioned. On the one hand I don't see any reason to dismiss them as a possibility, but on the other hand, I don't know if they could inflict the shallow back wound we seem to be dealing with.
To this I would tentatively add a third possibility, in red here:
At the moment I [sandy] can only accept three possible scenarios:
1. The pleura and probably the lung were punctured, and Humes et al are lying to protect the LN scenario
2. Some form of an 'exotic bullet' penetrated his back and then broke up to such a degree that it left little or no trace. "Ice bullets", "blood soluble bullets", mercury bullets, etc. have been mentioned. On the one hand I don't see any reason to dismiss them as a possibility, but on the other hand, I don't know if they could inflict the shallow back wound we seem to be dealing with.
3. A frangible bullet disintegrated and lodged itself within the right lung.
My reasons for making #3 tentative are two-fold. First, I want to know how it is that technicians interviewed by researchers made no mention of the collapsed lung. Second, I'd like to know how the frangible bullet just happened to fragment precisely before entering the lung. Or if it's possible for lung tissue to cause the bullet to break up
Robert, can you comment on this?
Tom, have you ruled out #3?
As I pointed out earlier, a frangible bullet designed for lethal purposes has a hollow point nose that is the key to making this bullet disintegrate back into the metal powder from which it was made. As it travels through flesh (or organ material) the frangible bullet's hollow point nose fills with semi-liquid material. Due to the velocity of the bullet, this semi-liquid matter exerts an enormous hydraulic pressure on the nose of the compressed metal powder bullet core. Within a few inches of penetrating only flesh, this high pressure will cause the bullet to disintegrate into a cloud of metal powder that will literally destroy everything around it for a 2-3 inch radius.
As I stated earlier, the frangible bullet would not have begun disintegration until it had actually entered the lung. This is true of head shots with frangible bullets, in which all that is usually seen on the exterior of the skull is a small neat entrance wound.
Dynamic Research Technologies Inc. .223 calibre frangible bullet fired into block of lye soap from 100 yards. No exit.
-
Jerrol Custer, who was the x-ray technician during the autopsy, told ARRB interviewers that he and assistant were not present when the "Y" incision was made and the chest organs removed. Other than that, I have not seen any reference made by one of the technicians regarding the lungs.
-
-
When it comes to skulls, does it make a lot of difference whether you "penetrate" or "pierce"?
I was commenting on the sheriff's comment simply because we don't know how slow a bullet would have to be going to only penetrate the flesh of JFK's back a mere inch, and somehow we have come to the conclusion that this shallow penetration in flesh might be possible at 300 fps. Sheriff Baca would seem to disagree with that notion.
Penetrate means entering the skull but staying within the skull. Pierce means entering the skull and exiting the skull. It would take roughly twice as much energy to pierce a skull as opposed to simply penetrating a skull.
FWIW, the derringer bullet lodging within Lincoln's skull was traveling around 400 fps.
Interesting. I never knew the difference but now I do.
Only 400 fps? Wow, we might have to lower the velocity of the "short shot" a little bit here.
-
I hate to disagree with everyone here but, I do not believe JFK was knocked over by a bullet; either in the jet effect scenario or the frontal shot scenario. I believe what we are witnessing in the Z film at z313 is two things that look like one.
The recoil I see in the film, from the head shot, is very brief and sharp and of a duration of maybe a second at the most. In this recoil, you can see JFK moving back and to the left maybe, at the most, an inch or two, before rebounding back slightly. THEN, we see JFK moving to his left and back. However, while most of you see him being driven back and to the left, I simply see him falling over as he loses consciousness and all motor control over his body.
I have seen the same thing more times than I care to remember hunting deer.
-
Absolute nonsense, Pat. Lattimer's test skulls were long gone off the ladder before there was any "recoil" (i.e., backward movement) of the ladder.
Let's try this again. The bullet never touches the ladders, and yet they tip forward. This proves that the forward momentum of the skull is being transferred into the ladders.
Think of it like shooting pool. The cue ball is the bullet. The cue ball strikes the 13 ball at an angle when it's an inch or so away from the 8 ball. The 13 ball then strikes the 8 ball. Upon striking the 8 ball, the 13 ball rolls backwards, but the 8 ball rolls forwards. Lattimer claimed that the backwards motion of the 13 ball replicated the movement of Kennedy, and proved the Jet Effect, but totally ignored that it had transferred its momentum into the 8 ball. It was a trick.
I have to agree with you on this one, Pat. I never noticed the ladder moving in the opposite direction until you pointed it out. These connivers will do anything to perpetuate the lone nut myth.
 not totally destroy the vertebrae in line with the path of this bullet?
not totally destroy the vertebrae in line with the path of this bullet?

Buttons & Bags - Prayer Woman Identified - But No Name Yet
in JFK Assassination Debate
Posted
Garbage in, garbage out.