

Andrej Stancak
-
Posts
1,262 -
Joined
-
Last visited
Content Type
Profiles
Forums
Events
Store
Posts posted by Andrej Stancak
-
-
I took the picture which Micah has posted as it looks to be of a better quality compared to those which I was able to view via a Google search. Of course, the wound is dark and the resolution not perfect, however, I guess it is still possible to reconstruct parts of what was the original incision made by Dr. Perry and a crude alteration performed later.
The picture below shows a cropped view of the autopsy photograph with the throat wound area (top), and the outcome of the photographic processing. The processing consisted in increasing the contrast and adding the light to the dark tones, adding hues which helped to resolve the contiguous patches of pixels (middle part), and resampling. The lower panel gives the description of different features of the wound. using numeric labels. This is explained in the next figure zooming only on the wound.
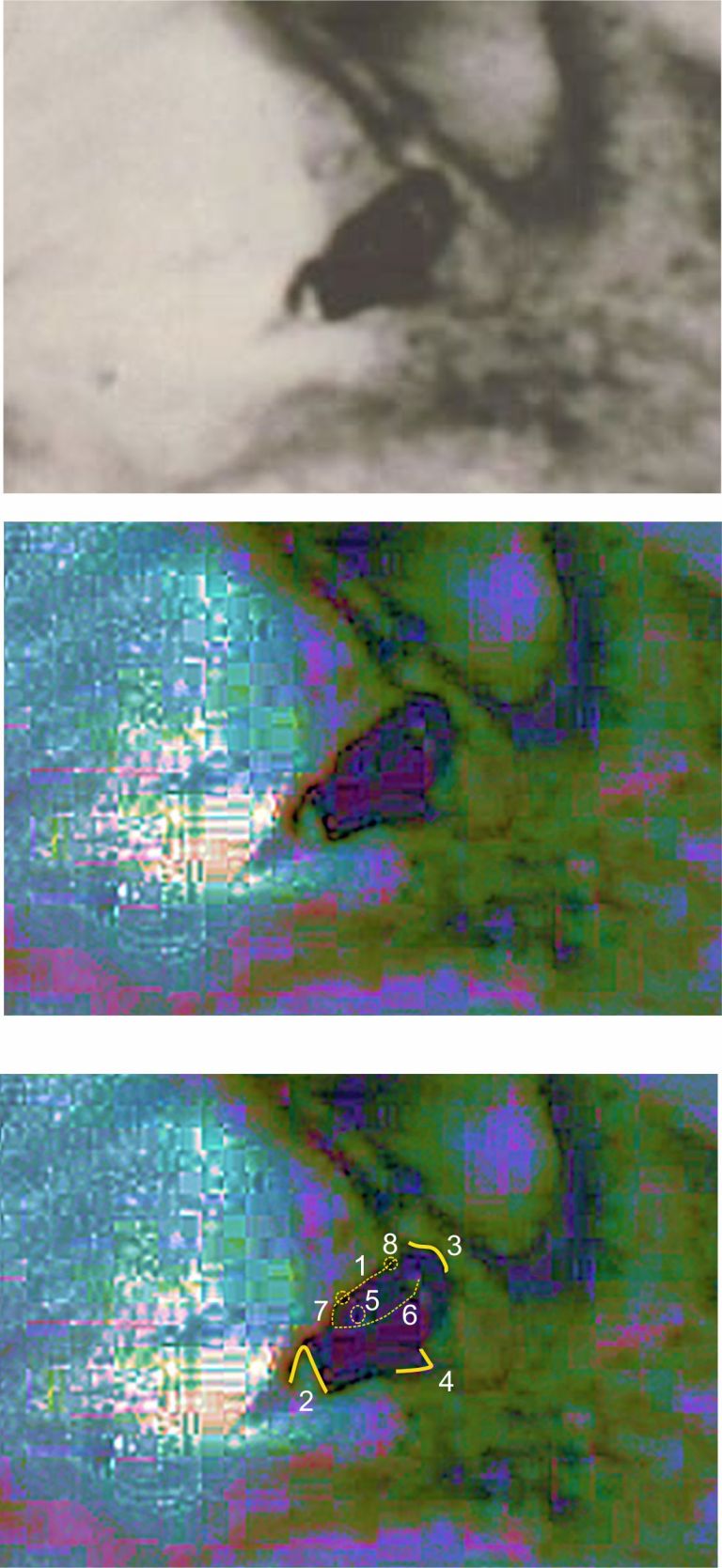
The next figure is the enlargement of the gash on the throat.
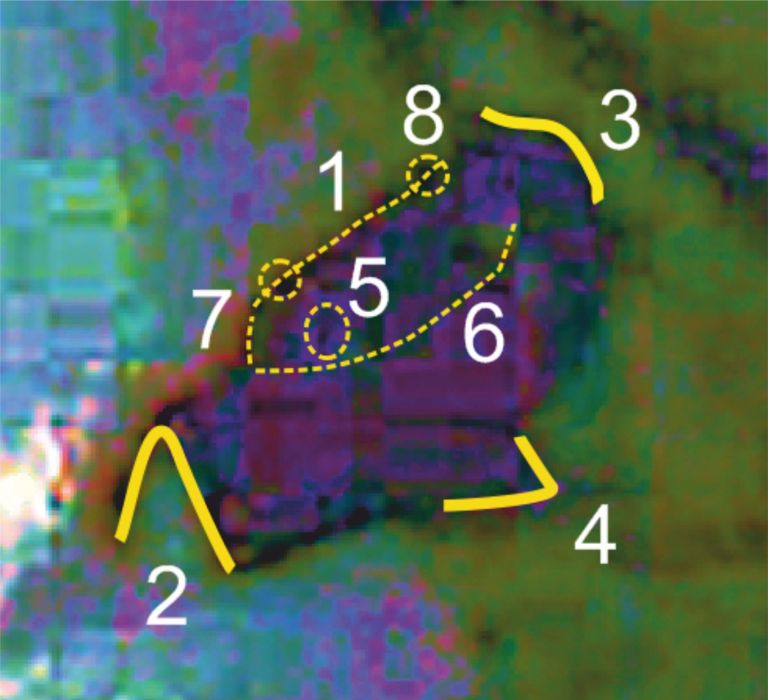
Residuals of the original tracheostomy:
1: The upper edge of Dr. Perry’s clean horizontal incision. 5. Existing gunshot hole or a tracheostomy opening. 6. A hypothetical line delineating the inferior edge of Dr. Perry’s incision. 7-8. Small openings related to sutures?Expansion-related signs: 2. A cut expanding the upper horizontal edge of Dr. Perry’s incision on the right-hand side of President’s throat. A raised flap of skin forms a triangle. 3. A raised skin flap on the left side of President’s throat. 4. A vertical mid-saggital cut.
Of course, some of the signs are debatable, however, the neat about 3-cm line (1) clearly differs from the lines (cuts) on each side (2-3) or in the lower lip of the wound(4). These are different cuts made by different persons. What was likely to happen was that Dr. Perry made a clean incision (1) and performed a tracheostomy. The skin incision was very likely sutured with 2 stitches, one on each side, during or after the tracheostomy. Since the skin incision was very professional and neat, it would have been possible to inspect the original skin injury related to the gunshot as to whether it was an entry or exit wound. I assume the wound was sutured by some junior staff member after the senior staff left and the body was being in the process of preparation for the transport for the autopsy.
This neat wound was apparently seen by Dr. Ebersole (BE, Chapter 23) and since there was a stitch over the midline as well, he was confident that this was related to the tracheostomy. Surgeons would close the wounds which were created by themselves and would leave those wounds which existed and did not threaten patient's life intact for forensic purposes. The pathologist knows in such a case what was a wound related to the crime and what was a wound created by the surgeons. It is also a part of a good surgical practice to close any wounds arising during a surgery no matter whether the patient survived or not.
The wound was heavily tampered with though. The sutures from Dallas, if they existed, were removed, and cuts were made to extend the top lip of Dr. Perry's incision wound to each side. These cuts were about 1.5-2 cm each. Then, the lower lip of the original incision wound was cut vertically with about 1 cm cut. This cut eventually destroyed the rounded gunshot wound. A retractor was used to pull the lower lip of what is now an expanded incision, and as the wound was expanded by at least 2 cm, it was necessary to relieve the tension around the edges by two other cuts. This is why a triangular flap (2) can be seen in the gash on the throat.
As Dr. Ebersole claimed he had seen the neat sutured wound at Bethesda and attributed it to the tracheostomy made in Dallas, this expanded wound was very likely caused after Dr. Ebersole's first view of the body. Could it then be during the time elapsing between the first presentation of the body and the official start of the autopsy? I am aware that David (L) assumes that this time was used to reunite the body with the bronze casket, however, the alteration of the throat wound would be a matter of 3 minutes, and could be squeezed into more than 30 minutes elapsing between the first and second presentation of the body.
-
10 hours ago, David Lifton said:
But there’s no “trace evidence” of any such event—i.e., no trace evidence of any suturing at Parkland.
So, with all due respect for the effort you have put into your post, I believe you can (and should) set that aside and “edit it out” of your possibilities.
David:
Did you ask directly Dr. Perry or any other doctor who was in ER1 if they made any suture while doing the tracheostomy? The thing is that they may have done some stitches but did not tell because it was automatic and they would not describe all details of how they did the tracheostomy - for them it was a routine. Sometimes, two sutures are placed directly on the cut tracheal ring on both sides of the catheter, and sometimes two stitches are made on the skin on each side. These sutures help to keep the catheter stable in the trachea. The doctors could have told about making stitches were they asked, and they did not bother to tell if no one asked. Who knows.
However, I agree it would be strange that no one would report that any sutures have been made in the neck area.
------------
Addition (07/03): I have now refreshed my memories of Best Evidence by re-reading Chapter 23 and some other chapters. Dr. Ebersole testified for the House Select Committee on Assassinations that he has seen "neatly sutured by a surgeon in Dallas". I also got that you have asked Dr. Clark about the possibility of applying sutures to any of the wounds which he has denied. Dr. Ebersole claimed that the neck wound has been sutured including the hole which he thought at that time that it was related to the tracheostomy. Your book says that the medical staff got into contact with Dallas doctors about 11-11.30PM and that was the time when they realized that there was sewing on the throat. Dr. Ebersole reasoned that a tracheostomy was made, the tubes were pulled out, and only then the stitches were made. Dr. Ebersole repeated this to the reporter Gil Dulaney.
-------------
Well, this opens one more possibility besides a body alteration after the body left Dallas and before it was presented for an autopsy. If there is a surgery causing opening of patient's body and even if the patient dies, all wounds caused by the surgeons would be sutured. Suppose there is a patient undergoing a cardiac surgery, and the patient dies during the surgery. The surgeons would not abandon the body as it was when the patient died, they would close the chest and suture the wounds. Could something similar happen in Dallas? Most of the doctors leave and while the body is being prepared for a transfer to the pathology department, stitches are applied to the neck.
I am just trying to make any sense of the different testimonies regarding the neck wound, with not too much of success I see.
-
Michael:
I do not know how exactly was President's body transported to Bethesda Naval Hospital. However, it surely arrived in a different coffin compared to the heavy ceremonial casket, and President's body was in a plastic zipper bag, not in a blanket and towels. This is enough to assume a massive clandestine manipulation with the President's body. How exactly this all has been done is a matter of research, and David has put forward a reasonable hypothesis. I myself do not have my own theory because I feel I do not know enough about this problem. As you may know, I am continuously working on a 3D reconstruction of the Depository doorway, and after three years of a systematic work, I can see some humble fruits. While one can be a good expert only in one aspect of the case, I am also interested in medical aspects and other aspects of the case because this helps me two understand the events unfolding in the Depository better.
I am familiar with David Von Pein's comments and appreciate them even if they are biased towards the lone-nut side. I could not see any point in David (VP) posts which David L would not have responded in great detail ("ultra-detailed" in David von Pein's words).
I hope this helps.
-
26 minutes ago, Michael Walton said:
What a joke, Larsen. You're just as bad as Josephs and all of the other paranoid people on here. Why would Perry - a quiet doctor down there minding his own business and suddenly thrust in a historical event - suddenly become a boogey man here? He said he cut through the wound to try to save Kennedy's life. He didn't even want to talk about it to the WC but he did anyway and clearly explained what he did. If you don't want to believe him, then that's your problem just like it's your problem if you don't want to believe the world is round.
Further, the stare photo confirms this. And he said it again in the broadcast Von Pein put on here.
You and your "I'm only about the facts" really makes me sick. You're considered a joke not only on here but on other forums what with your INDISPUTABLE PROOF of a missing tooth and all of the other malarkey you spout out. You do this all of the time and Lord knows if I'd not called you out for you even saying you thought one of the old guys had a pistol (cop out term = black object) you'd probably even be saying THAT is evidence and the facts according to you. And that was several years.
Sheesh!!!
Michael:
may I ask you to stop ventilating your aversion to David Lifton and other forum members in this thread? Please set up your own thread, and you will see how many people will respond to it.
David Lifton is a distinguished researcher and author and deserves all respect. We are privileged to have such expert among forum members. David put his name and much of his life into his research. He was also lucky but also perseverant to be able to speak with a number of witnesses in person, record their reports, gather different materials, and visit the critical places such as the morgue at Bethesda hospital. Those of us who came late (and may not even live in the USA) can only refer to secondary information which has been filtered and perhaps tainted. The closeness to the sources is also one of the reasons why David's work is original, essential and unreplicable. Here I need to correct myself a bit because a large part of David's research has been actually confirmed, e.g. by Mr. Doug Horne.
I take David's presence on this forum and his sharing with us his original ideas as a sort of another Christmas. However, you need to understand that when someone is working more or less alone on a research problem and is very deep and advanced, there are not too many people who can help. It is like digging a deep tunnel which narrows down as you progress and at end, there is no one nearby to help you. While David knows his stuff very well, he also needs to hear an independent view else it is very easy to commit a mistake and jump to conclusions too fast. Can you second David's theses? Can you provide a feedback which may not be accurate or elaborate but which could still highlight a potential problem?
If not, may I then kindly ask you to withdraw your insulting comments.
-
David (L):
your research and hypotheses are mind-boggling. I confess that I need more time and reading to be able to swallow all new information.
However, let me come back to the neck wound. Even here I am in a state of confusion, seeing that any attempt to make sense of it would not survive the next round of posts. Anyway, let me review the three possibilities of how a tracheostomy could have been achieved.
1. Inserting a tracheal catheter straight into the neck wound without making any incision or tracheotomy. This is a very unlikely possibility because there was blood frothing from the wound. Such option would be risky as it could result in suffocating the patient. Without a detailed inspection of the wound, it would not even be clear where this opening would lead to. This possibility is not supported by most of the testimonies and reports. A skin incision and a tracheotomy were performed.
2. An incision was made through the neck wound which allowed inspection of the wound. This is what Dr. Perry told the Warren Commission, and he also provided some details about the wound which details were obvious to him after making a horizontal cut through it. Further, the wound would be expanded above and below the opening in the trachea (caused by the gunshot), and that allowed to expose the second or third tracheal ring and to make a tracheotomy below the existing hole in an undamaged part of the trachea. This would be consistent with both a tracheotomy below the wound and an incision through the wound. Dr. Perry's statement for the ARRB, quoted in one of previous David Von Pein's posts, provides some support to this possibility. The wound would be very large by now and it would be fully understandable if Dr. Perry would also suture the neck wound with 1-2 stitches on each side. Suturing the skin and fascia around the tube used for a tracheostomy is a part of the procedure. The tracheostomy allegedly lasted 5 minutes (William Manchester's book) which long time might have involved also making some 4 surgical knots. After the President was pronounced dead, all the tubes were removed from President's body. This left the neck wound sutured and narrow, with an opening in the midline which opening was related to the neck gunshot wound. There was no suture through the opening in the neck because sutures were made with the tube in its place. The resulting picture of the neck wound was that of a neat incision because it was sutured and a rounded hole in the middle of the throat because of the gunshot wound and the circular tube which was just removed. Therefore, Dr. Perry did not remember ever causing a gash on the neck seen in the autopsy photograph. He might have said that he left the neck wound inviolate because it looked after removing the catheter more or less the same as he saw it when he first approached President's body.
The gash on the throat might have been the result of tampering with the body or a part of the autopsy in which the sutures were cut for an inspection of this wound.
3. An incision was made below the neck wound and a tracheotomy and tracheostomy were carried out on an undamaged part of the trachea. This solution would contradict Dr. Perry's testimonies for the WC and ARRB, and it is therefore not the most likely scenario.
Unless some novel information pops up which is entirely possible given how dynamic this thread is, I am inclined to believe in (2) : there was a cut through the wound, Dr. Perry created a space above and below the wound, and used a healthy part of trachea below the site of injury for tracheotomy and tracheostomy. As a standard part of any tracheostomy, he sutured the tissues on both sides of the catheter. After the catheter was removed, the incision was appearing as a narrow horizontal line, well sutured, and the opening caused by the gunshot wound was seen as it looked before any surgery to the neck - it was "inviolate". This wound, in my opinion, could have still be used to decide whether the gunshot wound to the neck was an entry or an exit wound.
-
Let me add one more source which provides some authentic information relevant to the case of the neck gunshot wound, William Manchester's "The Death of A President", 1967 (2013 edition).
On the neck wound, page 182:
"They could not win now. The throat wound - which was then assumed to be an entry wound, because there was no time to turn him over - was small, and it exuded blood slowly".
On the tracheostomy, page 184:
"The great need was, however, for some sort of breathing passage. The tube that the resident had inserted wasn't working, apparently because of the wound in the neck. Analgesics were unnecessary. Kennedy was in coma. "Scalpel", Perry muttered. A nurse slapped one in his rubber palm. Incising the President's throat just below the mediastinal wound, he began a five minute tracheostomy ("a mouth in the throat"). Meanwhile, the tube between Kennedy's lips had been connected to the respirator in an attempt to start him breathing again."
On page 186:
"Perry had just finished the tracheostomy when Clark arrived; he was inserting a cuffed tube in the windpipe. Jenkins attached it to an anesthesia machine , the controls of which were more delicate that those of the respirator.
-----------------------------------------------
The use of "mediastinal" in the 2nd quote was not correct because mediastinum is the soft tissue in the chest that separates different organs. Anyway, Manchester's description fits well with Mr. Breslin's account of what Dr. Perry told him, and with Dr. Perry's "inviolate" to Dr. Stewart (in David's messages). The presence of bleeding from the neck wound (which I learned from Manchester's book by checking again what I read a while ago) excludes the possibility of using this wound as it was for a tracheostomy. Taken together, it is very likely that Dr. Perry made an incision below the gunshot wound in the neck and he therefore was sure he left it "inviolate" and could deny causing the damage to the throat seen in the autopsy photograph.
What followed next, Dr. Perry's testimony for the WC and his CBS interview, are in my view deceptions prompted by expanding the wound to obfuscate the frontal shot to the neck. While they are important to document the level of the cover-up, they only distract from the true course of events in the ER1.
-
David (L):
thanks for your very systematic account which sheds new light on the throat wound. This is an important addition to the data on President's head wounds (BE).
As for the audio clip with "rendrd ..... uh... inv..", it could have been tampered with. There could have been two versions of the tape, one with "...inviolate" and one with "... invalid". It is just difficult to prove and this is why if I would press on this point I would be accused of being a paranoid conspiracy theorist seeing alterations and falsifications everywhere.
I look forward to reading about the neck wound and other new work in your upcoming book.
P.S. I asked my son who is a medical doctor (orthopedist) about whether he would perform an emergency tracheostomy with an existing throat wound located advantageously in the midline. He recommended asking a trauma surgeon which is something I recommended in my earlier post. After pressing more, he admitted he actually would use an existing wound in case of an emergency.
-
15 hours ago, David Von Pein said:
Conspiracists will try to find conspiracy and "distress" and cover-up everywhere they look. It's just their nature. But in my view, Dr. Perry was merely trying to find the right word there. And he came up with "invalid". How many times in your life have you started a sentence and then reached a point where you groped for an appropriate word to finish your thought? Hundreds of times? Thousands?
David:
it is not relevant whether I am a conspiracy theorist or not (as a matter of fact I am). My post pointed to the early statements by Dr. Perry about making a treacheotomy below the neck wound (to Mr. Breslin) and leaving the neck wound "inviolate" (to Dr. Stewart). I have pointed out to a logical and factual impossibility to make a tracheotomy at a place where an opening already was which questions Dr. Perry's statement about making a tracheotomy.
Thus, the conflicting statements, the early statements and the ones for the WC and CBS, suggest that Dr. Perry had to change his view if he claimed that he made a cut through the neck wound which claims differ from the statements he made shortly after the fact. As far as the CBS interview is concerned, such programs are prepared to the minute details with scenarios and scripts available before actual recordings. Actually, Dr. Perry's talk sounds to me like a rehearsed narrative. The more I was surprised by hearing much of hesitation in his speech and the swallowed word "render" in the audio clip you kindly posted.
-
15 hours ago, David Lifton said:
On November 23, 1963, Dr. Perry told Jimmy Breslin that he made an incision "below" the bullet wound. On that occasion, he did not use the word 'inviolate," (as far as we know); he simply said (i.e., told Jimmy Breslin) that he inserted the tracheotomy tube "below" the bullet wound; and Breslin then used that word--"below"-in the article he wrote for the Saint Louis Post-Dispatch which was published on 11/24/63, and which was then reprinted as "Death in O.R. 1" in the Sat Evening Post of 12/14/1963.
On that same weekend (according to Dr. Dave Stewart, who first related this to me in a telephone interview in 1982) Dr. Perry told Stewart --that he left the wound "inviolate." Steward told me this in 1982, by phone; and then repeated all of it in considerable detail i a filmed interview that I conducted in June 1989, with Pat Valentino also being present. (See paragraph below, starting "In June 1989").
David (von Pein) and Sandy:
the 1966/67 CBS interview was aimed to calcify the WC outcomes and therefore, I am not surprised that Dr. Perry had admitted making a cut through the neck wound in that interview which was just a confirmation of what he had said to the WC. However, please also read the statements collected by David (quoted above) in which Dr. Perry claimed cutting below the neck wound and leaving the neck wound intact (my interpretation of "inviolate"). These statements were close to the event and are therefore the most valid and genuine statements, in my view.
Please consider the logic for a moment: Dr. Perry cuts through the neck wound. What will he find? An opening in the trachea from the gunshot. However, he also claims to make a cut to the trachea - but where could he cut the trachea if there was only one cut to the skin and fascias and this cut only exposed the part of trachea with the opening from the gunshot? He did not need to make a tracheotomy if he made a cut through the neck wound, however, he did (confirmed also by Dr. Carrico).
In the 1966/67 audio clip with Dr. Perry, please mind about 2 seconds gap elapsing between a swallowed "rendered" and the next word "inv....", with an "uh". Does this look natural when other parts of the clip contain a fluent speech? In my view, Dr. Perry was in severe distress when saying this.
It is a mess and I understand that it is hard to find an explanation that would satisfactorily explain all the statements, interviews and the gash on the neck in the autopsy photograph. The common denominator could be that Dr. Perry made an incision below the neck wound, and then he made a tracheotomy and a tracheostomy on an undamaged tracheal ring. The neck wound was, according to this interpretation, expanded later to exclude any chance of interpreting the neck wound as an entry wound. This is why Dr. Perry did not accept his authorship of the crater in the throat. The rest is just a mess and confusion, intentional or non-intentional, I do not know. Dr. Perry went with the official version during his WC testimony. I am not sure what exact word was used in the CBS interview - "inviolate" or "invalid", however, I see signs of a strong distress on the part of Dr. Perry at those moments.
-
David:
congratulations on your finding of Dr. Perry's original statement "left the wound inviolate" which also has an interesting history, and thanks for sharing it here.
I read your two detailed posts on this matter carefully. It may be difficult to draw a conclusion which would not leave a grain of doubt. All three scenarios appear possible. I would line them up starting with the least probable:
1. The catheter was inserted into the wound directly without any tracheotomy being performed. In my view, a trained emergency surgeon would avoid this and would prefer doing a tracheotomy and tracheostomy as they are trained and always do, starting with an incision. The reason is that even if there is a hole in the neck which seemingly offers the chance to introduce a tube, the terrain is not known to the surgeon. There may be tissues and blood clots around that neck wound which would then be blown down to the bronchi and could suffocate the patient. It is, therefore, more likely that an emergency tracheostomy was made quickly at a different spot below the neck wound but not too low as there are large jugular veins around the clavicular bones. I would recommend to make a small survey among the emergency surgeons and ask them if they would use a gunshot wound apparently completely perforating the trachea for a tracheostomy.
2. Dr. Perry might have done a horizontal incision through the wound to expose the trachea, and finding the situation favorable, he inserted the tube into the existing perforation. While doing it, he would still see the original entry wound, especially after removing the tube because the edges of the incision wound would retract due to recoil force of the tissues, leaving just a line on the neck (incision) with a rounded hole (gunshot wound). This would explain his statement "...inviolate", as he still could see the original wound as it was before a tracheostomy. The gash wound with deeper tissues exposed which is seen in the autopsy photographs would be then related to an attempt to cover up the rounded hole.
The statement " From Dr. Carrico 11/22/63 report: "a tracheotomy was performed by Dr. Perry (WCE 392 [17 WCH 5]); " suggests that an incision and a section of the trachea were indeed made to accomplish the tracheostomy.
3. Dr. Perry made a tracheostomy starting with an incision which was made just below the gunshot hole in the neck. This is, in my humble opinion, what I would expect Dr. Perry to do. Dr. Perry could do the tracheostomy as he was trained to do and, therefore, he would be able to say "left the wound inviolate" in the strongest possible meaning of this statement. What happened later was that someone took retractors and pushed the edges of the incision apart to connect this incision with the rounded hole above. This would have to be an aggressive approach causing further injury to the tissues (the incision would not form a thin line anymore) which is what we see on the autopsy photograph.
Sorry for maybe contradicting your preferred explanation, however, I just would like to provide some independent view which may (or may not) help you to refine your explanations. I am not a medical doctor myself, however, I made several tracheostomies in rats during my junior lectureship period when I as was an assistant professor of medical physiology at Charles University Prague.
-
George:
you are missing a lot.
Temperature: it will slowly rise in a thermos, on a bus, in warm weather conditions. As a result, the cells will basically boil. You can have live cells in culture flasks for few days but the flasks will be kept at room temperature, some 22 degrees Celsius.
pH: depends on the metabolism of cells. The waste products of metabolism is CO2 which inevitably creates H2CO3 by interacting with water, and this is an acid. So, you need to exchange the medium regularly else the pH will be continuously dropping (becoming more acidic) until the cell metabolism stops because the cell would not work at low pH.
Mechanical insults: you carry the cells in a medium in a thermos in a standard bag, on a bus. This means that the content of the thermos will be shaking continuously causing many cell to damage their membranes as they hit the wall of the thermos. The cells die and spill their content into the medium which will increase the osmolality, and they will start losing water, shrink and die. To protect the cells in a culture flask, it would have to have some kind of gel lining around the inner surface of the flask. Which Judyth's thermos did not have.
Osmolality: Lee received something like glucose, some sort of nutrient to add it to the medium. Judyth had it for a fish bowl. The problem is that you do not have fish in a thermos and the cells will not eat big chunks of Lee's crackers which he drops into the thermos. That cracker or whatever it was would dissolve in the medium and since the cracker contains solid organic and inorganic particles, it will increase the total concentration of particles in the medium relative to water. As a result, the water from the inside of cells will start to be sucked off out of the cells, the cells will shrink, their membranes would rupture, and the cell would die.
Time: the cells fate would need to be sustained for the entire trip to Mexico City, then to the contact person, then to Havana, then pretreat Castro with X-rays, small or large, repeated over many days. The thermos would contain a stinking soup at this stage as it all will take maybe 3 weeks?
Havana side: who from several Castro's trusted and checked doctors would kill his/her patient? They all had to follow the Hippocratic Oath to which every doctor has to swear. Besides, how to convince Castro to ruin completely his immune system with many repeated X rays and then let himself inject a chicken broth - this is how Judyth described it when it was fresh.
George, I suggest you contact a medical doctor in your environment and ask him or her if it is possible to kill someone by injecting mice cancer cells into a human with an idea to cause a fast growing cancer. The person may die but not because of cancer but because of sepsis caused by the chicken broth being injected into the bloodstream. Although I gladly offer my limited knowledge to describe the problems, you do not believe me anyway. This is why I would like you to deal with these problems on your own.
-
Ray:
I understand that the cells in the case you describe have been maintained in a lab environment in which pH, temperature, osmolality etc. are continuously controlled. This is nothing like a thermos style which Mrs. Baker tried to sell.
-
9 minutes ago, George Sawtelle said:
Andrej
Who cares who brought it up.
THE FACT IS CANCER CELLS CAN SURVIVE OUTSIDE THE HUMAN BODY IF GIVEN ENOUGH OXYGEN, NUTRIENTS AND WASTE ELIMINATION.
So Oswald could have transported the cancer weapon in the thermos.
George:
sure not, however, you wish to believe that this is possible, and I will not interfere.
-
7 hours ago, George Sawtelle said:
Andrej
Nitrogen, either liquid or solid, is not needed to preserve the cancer outside the body.
Cancer cells can survive outside the human body as long as they are kept in a well-aerated liquid medium containing all the nutrients they need and the medium is replaced regularly to get rid of waste products.
According to JVB, Oswald was given a new batch of cancer cells in Houston which gave the cancer cells two more days of shelf life. One day from NO to Houston and then two days from Houston to Mexico City. Did not need to replace the medium until Mexico City.
I provided an article that indicates low level radiation can suppress the immune system. I think you are correct 100 rem is too much radiation for a x-ray machine. It's more like one rem. I would consider 1 rem low level radiation.
It is all right, George. You brought the nitrogen idea.
-
36 minutes ago, George Sawtelle said:
Andrej
I discussed with you some issues you had with the bio-weapon ...
1. transportation of the cancer cells. You did not answer what I posted about transporting cancer cells in nitrogen. In her book, JVB said Oswald carried the cancer cells in nitrogen.
2. low level radiation and it's effect on the immune system. I cited an article which indicated levels as low as 100 rem could negatively effect the immune system. You never answered.
George:
Liquid nitrogen would freeze and damage the live cells. 100 rem is an unusually strong dose of radiation, not a low level.
However, nitrogen was not the medium used by Lee while allegedly transporting the bioweapon. This is what Judyth has to say:
"In a few minutes, Clay Shaw arrived with a zippered bag like the blue one Lee owned. It held two thermoses: one contained the deadly cancer cells. The other contained a sterile medium for replenishing the liquid in other thermos to keep cells alive. There were also packets resembling packets of sugar to make more sterile medium, if necessary. There were also crackers and bananas in the bag, to make it look like a punch pack that could pass a simple border inspection. If inspected visually, the cancer cells would look like a chicken broth".
This would be a comedy in blue if it were not sad.
"
-
I am reposting a part of my June 17, 2017 message as somehow the most crucial aspect where Mrs. Baker's story fails has not been taken on board. There cannot be a cancer bioweapon which would use live cancer cells taken from an animal model and injected into a human. Cancer can be facilitated or provoked by injecting a radioactive substance, however, this is not the same as an infection caused cancer. And Mrs. Baker was not preparing plutonium or other radioactive capsules for Castro.
It is a physiological and medical nonsense to think of cancer as an infectious disease. If we care for someone with cancer, we are not at risk of being infected by patient's cancer. Similarly, it is also a nonsense to transport any live cells in a jar just like that, in some medium, for days. After excluding bioweapon as an utter hoax, the whole story becomes a list of encounters which may or may not happen.
"However, there are parts of the story which have never been analysed properly and which cast doubt on the essence of the story. Lee and Judy were supposed to work on a bioweapon which Lee would transport to Mexico where he would meet a contact, a young Cuban doctor, who would in turn arrange injection of living cancer cells into Castro's body. To make sure that the cancer cells would kill Castro, Castro would have to go for X ray(s) to suppress his own immunity. Well, this is a complete hoax. Living cells cannot be transported in a jar in a shopping bag for days. Living cells need either to be frozen or kept in a controlled solution in which ion concentrations and temperature would be continuously monitored - this requires a lab. We cannot be injected with cancer cell and die because those cells would be immediately recognised as coming from a foreign body (there is a marker called major histocompatibilty complex on every cell which tells whether the cell is own or foreign) and would be destroyed by recipient's own immune system. One can suppress the immune system by X-rays, however, each dose of such immunosuppressive X-ray would be about 10 times stronger than a standard diagnostic X-ray dose of radiation, and it would have to be repeated for quite many days. Would you believe that Castro's doctors would consent to it? Would Castro undergo such treatment without asking? At the end of the X-ray "therapy", Castro would be good to die without Judyth's injection anyway. Leukemia patients undergoing immunosuppression to receive bone marrow grafts are kept in ultra-protected environment because even such a minor infection as having a caries in one tooth would kill the patient."
-
19 hours ago, Bart Kamp said:
Check my post at the bottom of page 1.
With regards your drawing.
There is no Lovelady as he is gone
No Shelley as he is gone
No Calvery as there is no proof to ID her.
No Hicks as there is no proof to ID her.
No McCully as there is no proof to ID her.
No Williams as he is gone
No Davis as there is no proof to ID her.
Stanton may be the short heavy set lady you found in Darnell
Sanders is nowhere to be seen.
Bart:
I may not be able to change your mind on your string of No's . However, I will do all I can to convince you that the light object next to Mr. Lovelady's face was actually a partial face of a person standing behind him. Therefore, I will reconstruct Altgens6 scene as a priority. It will take me about a week or two. Eventually, you will be the judge. I do not know the outcome of that analysis yet, however, I am sure that in the process we will learn a lot about what was going on in the doorway during the critical period. And that is another purpose of this threat.
-
Hello Gary and Tommy:
thanks for your expert suggestions. I have tried Google Maps to measure the distance from the western corner of the Depository doorway to the nearest of four trees mentioned in Gary's message. This distance turned to be 14.8 meters or 49 feet. However, Google Maps also allow measuring the distance from the doorway via a selected route the ladies may have taken. If I guessed the ladies' locations in Z-film correctly, their total distance from the doorway was only 42.5 meters or 140 feet. This is not a long distance at all. I guess 20 seconds is more than enough for an untrained person to walk fast over a 43-meter distance.

-
2 hours ago, Thomas Graves said:
Andrej,
I'll concede that the lady in dark (including a dark headscarf and a boldly patterned skirt with dark horizontal stripes that's a lighter color than her sweater) is on that step before lady in white (including a white headscarf) arrives. Both of those ladies have been spotted by Sandy and I in the Z-Film, standing with a couple of other close-together, headscarf-wearing ladies which group is immediately to the left of the positively identified guys, Templin and Brandt.
IIRC, in the Z-Film the lady in white can be seen wearing "heels," whereas the lady in dark two people to her right is wearing "flats". Which could help to explain how lady in dark arrived at the steps a few seconds before lady in white (whom I believe grabs a-hold of her friend's right arm as she's ascending the steps.
In short, I believe you have Lovelady and Calvery and Hicks/(Reed?) labeled correctly in your drawing.
Keep up the good work.-- Tommy
 5
5Tommy,
would it be possible to maybe measure the distance from the spot the two ladies occupied during the shooting (in Z film) and the Depository doorway? We can then estimate their time possibilities they had to reach the doorway better.
Your impression that the two ladies had their arms intertwined was not silly at all, I fell for it as well. Only when I failed to fit the white lady in this way did I realise that she was a freelancer. There was an alley in the crowd of people in the western half of the doorway whichis visualized in the top view of the doorway in one of my earlier posts. The lady in white had a clear path if she wanted to enter the building.
-
17 minutes ago, Chris Davidson said:
Andrej,
I would agree that Baker reaches the curb some 30 seconds after the last shot.
I do not agree with your assumption that everyone reacts the same way and therefore no-one moved(maybe they did, maybe they didn't) within that time period. Thirty seconds can be an eternity in terms of movement.
As for Baker:
The time it takes for Wiegman panning back to the TSBD after the head shot, until the Hester sync = 21seconds.
Bell films Wiegman filming the Hesters. The sync point between Bell and Wiegman is Hester stepping up onto the Colonade.
Bell continuously films afterwards for 1.3 seconds and picks up Wiegman starting to rise for his run down the knoll.
Gerda’s dual-sync of Couch/Darnell shows both Wiegman and Baker in there respective runs.
There is 3.5 seconds of missing footage from the Wiegman sequence.
Take those 3.5 seconds and apply that to Wiegman after we see him start to rise in Bell and to
Baker before we see him in Gerda’s dual-sync.Baker’s run to the curb equals 4 seconds.
This total = approx 29.8 seconds.
Chris:
some doorway occupants moved and some not during the period between Wiegman (Altgens6) and Darnell. Mrs. Reese, a short lady, stepped few steps up which would give a better chance to view what is going on up there over the Tripple Underpass. Carl Jones left the doorway entirely. Mr. Frazier moved about 2 feet forward. Prayer Man turned around towards his left compared to Wiegman. However, Mrs. Ruth Dean is exactly where she was in Wiegman film. So is Mr. Williams, the man shielding his eyes with one arm. And the same holds for the man in a black suit (Bill Shelley) who stands in the center-east part of the top landing in Altgens6, Wiegman and Darnell. Billy Lovelady moved towards the western wall and maybe a step or two down. Mrs. Stanton, if my analysis is correct, moved slightly back into the shadow of the top landing.
So, yes, people moved during the 30 seconds after the last shot but the doorway scene still shows the people who were there during the shooting at their locations or at locations not far from their locations in Wiegman. This what I believe my reconstruction shows.
-
A very instructive clip, Chris. The lady in white keeps moving the whole time while ascending the steps. The lady in dark cloth appeared to arrive sooner than the lady in white.
The point which I find important in the context of the reconstruction of Darnell doorway is that the scene corresponds to some 30 seconds of time that elapsed since the last shot rang out. Therefore, the people on steps would still be at identical or similar locations as evidenced in Wiegman film and Altgens6.
-
I did some research into the background of both ladies using publicly available data. Mrs. Stanton appeared not to be married. I was able to find an association with a person which was her sister, however, she also passed away. Thus, it is almost impossible to get any data on her appearance or a picture now. However, Mrs. Sanders was married and had children, and her son may live in Dallas. There is still a chance to at least ask about Mrs. Sanders and her appearance (height, body build), or even obtain her photograph. This would help to solve the problem of identities of the two ladies standing on the top landing on that fateful Friday afternoon.
-
Here is the doorway scene in Darnell film with provisional name labels. At least as I understand them currently. Happy to change if we can gather convincing evidence.

-
3 hours ago, Bart Kamp said:
And Shelley was nowhere on those steps Andrej. The person on top you have marked is Molina who is wearing a white shirt and not a jacket. Williams was gone as well.
Nor is that guy talking to the women going up the stairs Lovelady.
I suggest you amend your drawing and add the 5 women on the bottom of the East side. That is besides Stanton, Sanders, Dean and Reese. Those 5 women were not on the stairs in Wiegman they all arrived after the shooting.
In Altgens6 there is no one standing between Shelley and Lovelady. It is physically impossible and that tiny snippet you point out shows nothing that resembles a human.
Hello Bart:
it has been only about 30-40 seconds after the last shot when the doorway scene seen in Darnell was filmed. Almost all the players are still in the doorway. If anything like that (an assassination) happens, people are in the state of shock and, unless feeling a threat to their lives, they just stay frozen. Under the shelter of the doorway, the people there stared at the direction of the Tripple Underpass and did not need to throw themselves on the ground or flee. Some doorway occupants, sooner or later, moved to a better spot or even left the doorway but it was maybe still after a while. Carl Jones stood in the lower west corner and I cannot see him in the scene, so he may have left which was easy for him as there was no one in front of him obstructing his moves. Billy Lovelady moved a step or two down and to the west. He was constantly on the move, so he went closer to the spot which allowed him to view the events on Grassy Knoll/Tripple Underpass. His space was filled with Buell Frazier who moved a step or two forwards. Maddie Reese appeared to step up few steps. Mr. Williams still stays where he was in Altgens6, he only switched arms - he was shielding off his eyes with his right arm in Altgens6 and with his left arm in Darnell. His shirt is a long-sleeved shirt, unlike Mr. Molina's shirt which was a short-sleeved one. Mr. Molina stepped down one step in Darnell which allowed to see the short lady in the east part of the doorway.
This long comment wants to say that there was no reason for Mr. Shelley to run away from the doorway just yet. He is still there almost at the spot he had occupied in Wiegman and Altgens6. It is is a man showing the same body height in Altgens6, Wiegman and Darnell, and he wore a suit. There was only one person in the doorway in the suit - this one depicted in my model is him. He stood close to the edge of the top landing, and therefore only the lower part of his face is illuminated. This is also seen in Altgens6. I am aware that my reconstructions may cause ripples in some theories, however, this is the strength (and the risk as well) of photographic data - they always beat the self-reports which may be tainted by memory lapses, emotions etc. The timing reports given by witnesses during the shooting is sometimes difficult to accept.
Mr. Molina is in my view the man visoring with both arms connected in front of his head, the one with a white short-sleeved shirt.
As far as other ladies are concerned, I did not find it necessary to add still more people. I have no idea about their clothes and believe that they actually did not stand on steps. I cannot see how adding other people who were close to the doorway would help the case. Of course, it would be nice to model the whole Dealey Plaza!
Your comment on Altgens6 is interesting. The point is that the light object is just too large to be a continuation of Billy Lovelady's face, and too large to be just a photographic artifact. If you would think it was an artifact, could you find a similar artifact in Altgens6 which would be at the level of human heads? However, I understand fully that resolving geometrically the Altgens6 scene is very difficult. It is the last task in the sequence of my project: the next will be Wiegman, and then only Altgens6. Altgens6 was shot with a telephoto lens from quite a long distance. The doorway is a small section in that photograph, however, we view it enlarged as if it was shot from just a few feet distance. The geometry we expect to see in a standard photograph does not apply in Altgens6, and things which appear impossible can actually be possible. That said, I understand fully your comment about the geometric impossibility of an extra person to be between Billy Lovelady and Bill Shelley.

David Lifton teases Final Charade on the Night Fright Show
in JFK Assassination Debate
Posted
Thanks, Micah.